Embed Size (px)
Citation preview

Orthodontic treatment of dental open bite: A case report
Hasan I1 BDS, Mahamud AMS2 BDS, Hossain MZ3 BDS, PhD
INTRODUCTIONOpen bite is an occlusal characteristic where the upper and lower teeth are not in contact and vertical overlap does not exist. Although this type of malocclusion can occur unilaterally or bilaterally in the buccal segments, it is mostly seen in the anterior segment. Treatment of open bite is difficult, but relapse is easy. The multifactorial nature of the etiology of open bite is largely responsible for the indecision surrounding its diagnosis and treatment. The causes of open bite is multifactorial, which can develop from genetic and/or environmental factors. Open bite is generally classified in two categories: skeletal and dental. The diagnosis is important due to different treatment approaches. Generally, a dental open bite can be treated with orthodontics alone, while a true skeletal openbite requires a combination of orthodontics and surgery.
HISTORY AND DIAGNOSIS
24 years old female came to the department of Orthodontics and Dentofacial Orthopedics, Dhaka Dental College and Hospital with the chief compliant of problems in chewing foods and aesthetics.
The patient was in the permanent dentition. She had no relevant dental, medical or family history and had no history of previous orthodontic treatment.
On extra oral examination, we found that she had a convex profile, lips are incompetent at rest , she had normal nasolabial and labiomental angle and she had increased lower facial height.
Intraoral examination showed that she had an anterior open bite ,spacing in upper and lower anterior segment, canine relationship class-I on both sides, molar relationship class-I on both sides.
Patient history revealed that she had high frenal attachment and frenectomy was done earlier and her mother also has same problem suggesting that her malocclusion is hereditary.

Panoramic radiographs revealed that all teeth were present, no carious teeth were present. There was no bony pathology.
TREATMENT OBJECTIVES
Considering the above findings the objectives of orthodontic treatment of this patient were to –
1. Correction of anterior open bite.2. Correction of spacing of upper and lower jaw.3. Establish normal overjet and overbite.4. Establish normal interincisal angle.5. Correct nasolabial and labiomental angle.
6. Maintain profile7. Establish occlusal harmony and interdigitation for improved aesthetics and
proper function.
TREATMENT PLAN AND PROGRESS
Edgewise bracket was bonded and initial leveling and alignment was done with the use of 0.014 ss multiloop arch wires. Canine retraction and incisors approximation was done by power chain elastics on 0.016 ss arch wire.
As because the patient had normal naso-labial and mento-labial fold and her profile was normal, if we would go for upper and lower arch contraction, there was a chance that her profile could became retognathic. So, after canine retraction, we took a cephalometric x-ray to analyze her profile and dentition.
We know that the ideal position of lower incisors should be 2 mm infront of Apo line with an angulation of 90-95°to the mandibular plane and the ideal position of upper incisors should be 6 mm infront of Apo line with an angulation of 110°to the maxillary plane.

After canine retraction, pt’s cephalometric x-ray revealed that the lower incisors were 7 mm in front of Apo line with an angulation of 90°to the mandibular plane and the upper incisors were 6 mm infront of APo line with an angulation of 110°to the maxillary plane.
The molar relationship was 4 mm class-III. There was 6 mm and 5 mm space to close in upper and lower jaw respectively. The MM angle was 31°, so it was a high angle case and so cl-III elastics should avoid as because it might cause increased lower facial height.
8
7
6
5

So, we decided to 5 mm arch contraction in the lower jaw as because lower inisors could become 2 mm infront of APo line. After 5 mm lower arch contraction, the overjet now became 5 mm. In the upper arch, we had 6 mm space to close. But we should not do full arch contraction as because upper incisors to Apo line is 8 mm (Normal 6 mm) and full arch contraction would cause retrognathic profile. So, we proceed to 2 mm upper arch contraction and 4 mm anchorage loss of upper molars.
Arch contraction was done with tear drop contraction loops on 0.016x 0.022 inch rectangular stainless steel arch wires on both jaws. Interdigitation was done with up-down elastics. Then arch co-ordination, finishing, debonding was done and retention was given by Hawley retainer.
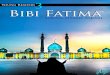
Extraoral photograph (before treatment)
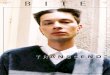
Intraoral photograph (before treatment)
Facial photo-Frontal view Facial photo-Right view Facial photo-Left view
Facial photo-Frontal view Facial photo-Right view Facial photo-Left view

Photograph during treatment
Fig: approximating upper & lower incisors by 0.016 ss round wire with power chain.
Fig: Arch contraction by .016*.022 ss rectangular wire with tear drop loop-lower arch

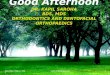
Pre and Post treatment Intra Oral photographs
Pre-treatment Post-treatment
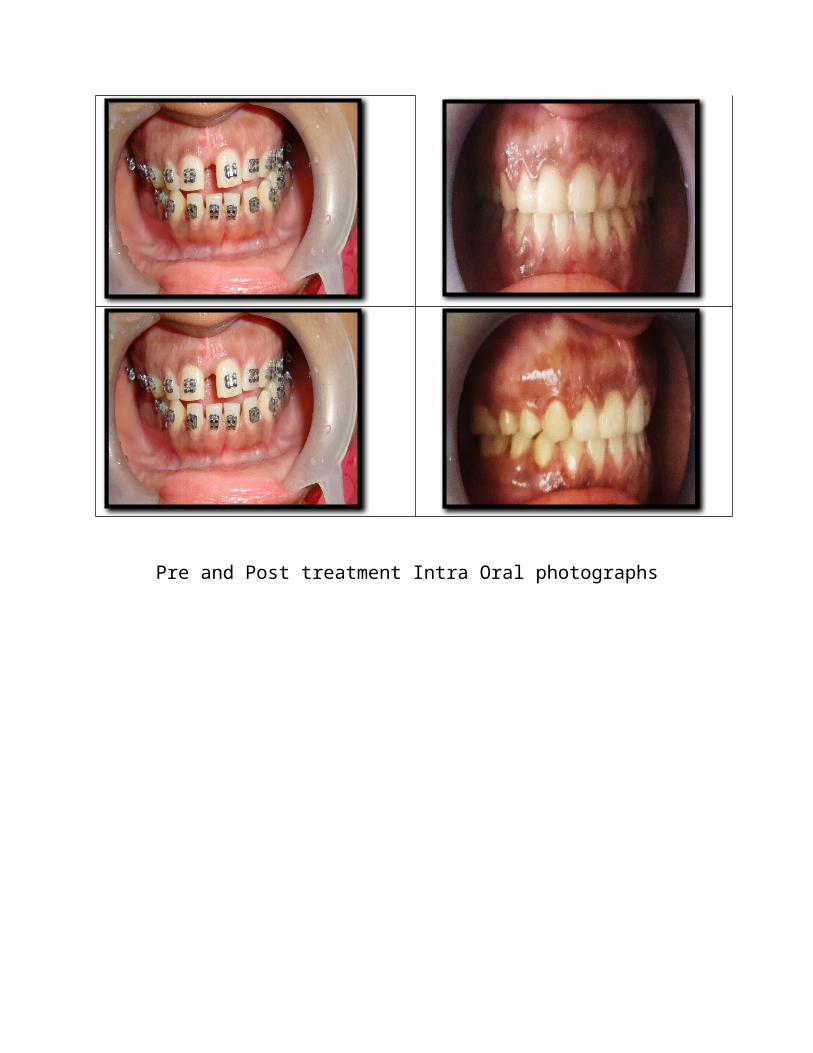
Pre-treatment Post-treatment

Pre and Post treatment extra oral photographs
DISCUSSION AND RESULTS:
Total treatment time was 24 months. The Class I Canine and molar relationship were maintained with satisfactory interdigitation. The overjet and the overbite were
established. The dentition and the periodontal tissues remained healthy. The patient was happy with his appearance.
Correspondence
Dr. Md. Ishtiaq Hasan, BDSFCPS-II TraineeDept. of Orthodontics and Dentofacial OrthopedicDhaka dental College and HospitalMirpur-14, Dhaka-1206Mobile: +8801716213184, E-mail: [email protected]