Embed Size (px)
Citation preview

MANAGEMENT OF MULTIVALVULAR
DISEASE
26-09-2017

DEFINITION
• Multivalvular disease (MVD) — the combination of stenotic
or regurgitant lesions, or both, on two or more cardiac valves
— is a highly prevalent clinical condition among patients with
valvular heart disease.

EPIDEMIOLOGY
• EUROHEART SURVEY
a) patients with native valve disease - 20.2%
b) patients undergoing valvular surgery - 14.6%
Lung, B. et al. Eur. Heart J. 2003.
• SOCIETY OF THORACIC SURGEONS (STS) database(1993 and 2007) -
Multiple-valve surgery accounted for 10.9% of the 623,039 patients
undergoing valve surgery.
a) 57.8% on the aortic and mitral valves,
b) 31.0% on the mitral and tricuspid,
c) 3.3% on the aortic and tricuspid,
d) 7.9% underwent triple-valve surgery.
Lee, R. et al. Ann. Thorac. Surg. 2011.

• In the PARTNER trials, the incidence of
a. concomitant moderate-to-severe MR in patients with severe
aortic stenosis - 20%,
b. moderate-to-severe TR - 27%.
• In the EuroHeart Survey,
• the mean age of patients presenting with MVD was 64 years,
and 83.6% of these individuals were male.

CAUSES OF MULTIVALVE HEART DISEASE

ACQUIRED
Cardiac diseases
Rheumatic heart disease(51.4%)
Infective endocarditis
Degenerative calcific(40.6%)
Cardiac remodelling/dilatation (functional)
Adverse effects of
treatment
Thoracic/mediastinal radiation therapy
Adverse drug effects (ergot agonist, anorectic agents)
Non-cardiac systemic
diseases
End-stage renal disease on haemodialysis
Carcinoid heart disease
CONGENITAL
Connective tissue
disorders
Marfan syndrome
Ehlers–Danlos syndrome
Other (rare)
Trisomy 18, 13 and 15
Ochronosis (alkaptonuria)
Shone's anomaly
Congenital polyvalvular cardiac disease
Unger P et al Heart .2011.

INDIAN DATA

RHD
• >9000 RHD cases, Orissa
MS 35%
MR 10%
AR or AS 3%
MS+MR 15%
MV+AV 25%
MV+TV 12%
Indian Heart J 2003;55:152-157

RHD
• >9000 RHD cases, Orissa
MS 35%
MR 10%
AR or AS 3%
MS+MR 15%
MV+AV 25% >50% MVHD
MV+TV 12%
Indian Heart J 2003;55:152-157

RHD
• 518 RHD cases, JIPMER Pondicherry
MS+AS+TS 2.5%
(Triple stenosis)
Indian Heart J 1999;51:667

RHD
• NIMS, Hyderabad 2002
MS+MR 12.9%
AS+AR 4.4%
MS+AR 13.9%
MS+MR+AR 2.0%
MS+MR+TR 8%
MS+AR+TR 8%

RHD
• 434 RHD AUTOPSY cases, Mumbai
MV 21%
AV 2%
MV+AV 21%
MV+AV+TV 27%
MV+TV 5%
MV+TV+PV 2%
MV+AV+TV+PV 19%
Indian Heart J 2002;54:676-80

• Grover et al
• MS = 35%
• MS + MR = 28%
• MR = 16%
• MR + AR = 12%
• MS + AR = 6%
• Padmavati series
• MS = 63%
• MS+ TR= 18%
• MR = 12%

PATHOPHYSIOLOGY
• The clinical effect of MVD depends on a complex interplay of
pathophysiological factors:
a. the severity of each individual valve lesion,
b. combination of valves are diseased,
c. the type (primary versus secondary),
d. chronicity of the lesions,
e. loading conditions,
f. ventricular compensation.

• The severity and clinical effect of one valve lesion can be
altered if loading conditions change or if another valve is
repaired.
• These haemodynamic interactions can promote, exacerbate, or,
by contrast, blunt the clinical expression of each singular
lesion.

AORTIC STENOSIS AND MITRAL
REGURGITATION

Unger P et al Heart 97, 272–277 (2011).

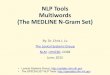
Figure .A patient with aortic stenosis and mitral regurgitation. a | This patient has severe,
symptomatic aortic stenosis with a mean transaortic gradient of 48 mmHg and an aortic
valve area of 0.7 cm2 on Doppler echocardiography. Left ventricular ejection fraction is
45%. b | Colour Doppler shows that moderate-to-severe mitral regurgitation is also present
. c,d | The same patient, 6 months after transcatheter aortic valve implantation. The mean
transaortic pressure gradient is 11 mmHg with only mild residual mitral regurgitation .
Left ventricular ejection fraction is 65%.

PRIOR TO TAVR POST TAVR

AORTIC STENOSIS AND MITRAL
STENOSIS

• Combination is infrequent in developed countries.
• As it is usually very poorly tolerated from a haemodynamic
standpoint.
• Treatment is sought early during the course of the disease.
• When both stenoses are severe, a greater reduction in cardiac
output occurs than with just one severe stenosis, decreasing the
flow rate and pressure gradients across both valves, which can
lead to underestimation of the severity of both aortic and
mitral stenosis.
Honey et al Br. Heart J. 23, 545–555 (1961).

• Physical findings – AS
• Clinical manifestations resulting from the MS — including atrial fibrillation, haemoptysis, and peripheral embolization —can occur.
• If concomitant severe AS not recognized, percutaneousballoon mitral valvuloplasty could impose a sudden preload increase to a small, hypertrophied, and stiff left ventricle, resulting in pulmonary oedema.
• Degenerative (or calcific) mitral stenosis in elderly individuals
• Due to progressive mitral annular calcification involving the base of the leaflets.


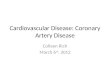
A patient with aortic and mitral stenosis. a | PLAX view of a patient with rheumatic aortic and mitral
stenosis and severe symptoms (NYHA class III).LVEFis 60%. b | The mean pressure gradient across
the aortic valve is 21 mmHg. c | Stroke volume, measured in the lvot (velocity-time integral [green
line tracing in top image] multiplied by the cross-sectional area [calculated from diameter: green line
in bottom image]), is 42 ml (26 ml/m2 of body surface area). The aortic valve area is 0.62 cm2,
consistent with a low-flow, low-gradient aortic stenosis. d | The mean pressure gradient across the
mitral valve is 8 mmHg, and the mitral valve area estimated from the pressure half-time method (red
diagonal line) is 1.65 cm2. e | Mitral anatomical orifice area (green outline) as measured by direct
planimetry is 1.2 cm2.

• This case highlights the inaccuracy of the pressure half-time
method to assess mitral valve effective area in the presence of
severe aortic valve disease.
• Moreover, this patient exemplifies the frequent and
challenging situation of low-flow, low-gradient stenosis,
present here at both the aortic and the mitral valves.
• This situation can lead to underestimation of the severity of
aortic and mitral stenoses.

AORTIC REGURGITATION AND MITRAL
STENOSIS

• The combination of AR and MS imposes opposite loading
conditions on the left ventricle.
• Both LV end-diastolic and end-systolic volume are lower than
with isolated aortic regurgitation.
Gash et al J. Am. Coll. Cardiol 1984
• Increase in SV typically associated with AR might be blunted
in the presence of MS,
• Clinical signs associated with increased pulse pressure might
not be observed.
Cohn et al. Am. J. Cardiol.1967

AORTIC REGURGITATION AND MITRAL
REGURGITATION

• Characterized by severe volume overload caused by the two
regurgitations and some pressure overload typically associated
with AR, is usually poorly tolerated.
• LV dilatation can be severe and the pattern of hypertrophic
remodelling is eccentric.
• Premature mitral valve closure — a protective mechanism
limiting the amount of backward flow into the left atrium and
the pulmonary veins in acute and severe AR — does not occur,
which contributes to poor clinical tolerance in patients with
concomitant AR and MR.

• Patients with this combination of valve lesions who are
symptomatic have worse LV performance than those with
isolated aortic or mitral regurgitation, resulting in a high
incidence of postoperative LV dysfunction.
Niles et al. Am. J. Cardiol. 1990.
Gentles et al. Ann. Thorac. Surg. 2015.

TRICUSPID REGURGITATION AND LEFT-
SIDED VALVE DISEASE

• Secondary TR - highly prevalent in patients presenting with
mitral valve disease.
Chikwe et al. J. Am. CollCardiol.2015.
• Common in patients undergoing surgical or TAVI for AS.
• Secondary TR is associated with reduced postoperative
survival.
• Complex interplay of factors — including free wall annular
dilatation, right ventricular enlargement and dysfunction, pulmonary
hypertension, and right atrial enlargement — underlies the presence
and severity of secondary TR in the setting of left-sided valve
disease.
Dahou, A. et al. TOPAS study JACC Cardiovasc. Interv.2015.

• No single factor is independently associated with secondary
tricuspid regurgitation.
• The severity of TR is highly sensitive to changes in loading
conditions.
• Absence of regurgitation at the time of treatment of the left-
sided valve lesion does not guarantee long-term freedom from
TR (i.e. annular dilatation alone can be a harbinger of future
tricuspid regurgitation).

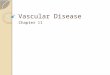
| A patient with mitral stenosis and tricuspid regurgitation before surgery. a | Colour
Doppler echocardiography shows moderate TR. b | On Doppler echocardiography, mitral
valve area is 1.2 cm2, and the mean pressure gradient across the mitral valve is 12 mmHg. c
| The tricuspid annulus, as measured from the apical four-chamber view in late diastole, is
41 mm.


DIAGNOSIS
• The haemodynamic consequences of MVD on blood flow, and on
ventricular size, shape, and function, as well as the specific
combination of valve lesions - influence the diagnostic process.
• Physical examination - misleading both in terms of the timing and
intensity of murmurs and other signs such as pulse pressure.
• Echocardiography - cornerstone of the diagnosis.
• As a general rule, measurements that are not dependent on loading
conditions, such as direct planimetry of a stenotic valve or, for
regurgitant lesions, assessment of the effective regurgitant orifice or
the vena contracta, are preferred.

ECHOCARDIOGRAPHIC CAVEATS IN THE
DIAGNOSIS OF MULTIVALVULAR DISEASE


• Catheterization is recommended when discordant or
inconclusive results are obtained on physical examination and
with noninvasive testing.
Nishimura et al.. J. Am. Coll. Cardiol. 2014.
• In the EuroHeart Survey, catheterization was performed in
30% of patients with MVD.
• Right-heart catheterization cannot be used accurately in this
setting because the stroke volume obtained using this
technique does not equal the stroke volume across the aortic or
the mitral valve in the presence of mixed aortic or mitral valve
disease, respectively.

MULTIMODALITY IMAGING
• Echocardiography - primary imaging modality.
• Other imaging modalities - when the information obtained
using echocardiography is not sufficient or is inconclusive to
determine the severity of each individual valvular lesion.
• Dobutamine stress echocardiography -low flow and a low
transaortic gradient to exclude pseudosevere aortic stenosis.
• In inconclusive echocardiography results, multislice CT can be
used to assess the aortic valve calcium score (severe stenosis:
>2,000 AU in men and >1,200 AU in women).
Clavel et al. J. Am. Coll. Cardiol. 2014.

• Real-time 3D transoesophageal echocardiography can be
useful to measure mitral valve area in rheumatic mitral
stenosis.
• Real-time 3D echocardiography with colour-defined
planimetry can be useful in selected patients with degenerative
calcified mitral stenosis.
Chu, J. W. et al. Echocardiogr, 2008.

TREATMENT

• Several factors are taken into account when determining the optimal management strategy.
1. Increased surgical risk of combined procedures and the long-term increase in morbidity associated with multiple prosthetic valves.
2. Risk of eventual reoperation and the prognostic effect of not correcting a less-than-severe lesion.
3. Likelihood of spontaneous changes in mitral or tricuspid regurgitation after surgery on a downstream valvular lesion.
4. Choice of surgical technique.
5. Emerging role of percutaneous approaches.
6. Crucial role of a heart valve team.

SURGICAL RISK AND LONG-TERM
MORBIDITY
• Combined surgical procedures on multiple valves are
associated with increased operative risk.
• In EuroHeart Survey, in-hospital mortality:
a. MVD - 6.5%
b. Single-valve surgery - 0.9% to 3.9% .
Lung, B. et al. Eur. Heart J. 2003

• In a series of 513 patients undergoing multiple-valve surgery:
• In-hospital mortality -12.5%,
• 5-year mortality - 32.9%.
• Postop, patients in NYHA functional class I or II- 80%.
• Patients in NYHA functional class IV – 0.6%.
• 5-year rate of freedom from late combined valve-related morbidity
and mortality - 71.7%.
• Pulmonary artery hypertension - main risk factor for postoperative
mortality.
Galloway et al. J. Am. Coll. Cardiol. 1992.

• STS DATABASE
• 1993 - 2007 - 623,039 patients underwent valve surgery.
• Multiple-valve procedures - 10.9% .
• Operative mortality doubled compared with single-valve
procedures - 10.7% versus 5.7%.
• Unadjusted operative mortality
a. Aortic and mitral surgery -10.7 %
b. Aortic plus tricuspid -13.2%
c. Mitral plus tricuspid- 9.7%
d. Triple-valve surgery- 14%
• Unadjusted operative mortality was 4.9%, 6.9%, and 10.0% for
isolated aortic, mitral, and tricuspid surgery.
Lee, R. et al. Ann. Thorac. Surg. 2011.

• Results demonstrate that, at the price of an increased operative
risk, acceptable clinical improvement and late survival can be
expected after a multiple-valve operation.
• In addition, the risk of late mortality after multiple-valve
surgery can be reduced by early surgical treatment, before
pulmonary hypertension, progression to NYHA class IV, or
deterioration of LVEF occur.

RISK OF OPERATION
• Treatment decisions for patients with MVD require knowledge
of the natural history of each specific valvular lesion.
• The risk of eventual reoperation and the prognostic
implications of not correcting a less-than-severe lesion should
also be taken into account.
• Increased operative mortality and poor long-term survival are
to be expected after a ‘redo’ valve procedure.
Fukunaga et al..Ann. Thorac. Surg. 2012.

• In patients with mild-to-moderate aortic stenosis,
the average yearly increase
a. in transaortic velocity 0.3m/s ,
b. mean gradient 7 mmHg,
c. decrease in valve area is 0.1 cm2 per year.
• The pattern of progression varies according to its aetiology;
aortic stenosis progresses faster in patients with degenerative
disease than in those with a rheumatic or congenital.
Otto, C. M. et al.. Circulation 1997.

• Patients with aortic regurgitation and normal LV systolic
function who are asymptomatic have a low likelihood of
progression to asymptomatic LV systolic dysfunction (<3.5%
per year)
• The risk of developing symptoms or LV dysfunction is <6.0%
per year, and the risk of sudden death <0.2% per year.
Borer et al . Circulation 2003.
• The rate of mitral valve narrowing in patients with rheumatic
mitral stenosis is variable, with an average decline of 0.09 ±
0.21 cm2 per year .
Sagie et al. J. Am. Coll. Cardiol.1996.

• Most recommendations on the management of less-than-severe
valve lesions in patients undergoing surgery for another valve lesion
have been extrapolated from data obtained with CABG surgery .
• During CABG surgery, concomitant aortic valve replacement for
moderate AS should be recommended if surgical risk is not
prohibitive.
• For mild AS, but concomitant aortic valve replacement can be
considered in patients who are expected to be ‘rapid progressors’
(those with documented rapid increase in aortic velocity, moderate-
to-severe valve calcification, or both), providing that reasonable life
expectancy is anticipated.
Sareyyupoglu et al. Ann. Thorac. Surg. 2009.

RISK OF MITRAL OR TRICUSPID
REGURGITATION
• Spontaneous changes in mitral or tricuspid regurgitation can occur
after surgery on a downstream valvular lesion.
• The severity of MR can be influenced by the presence of aortic
valve disease.
• After AVR, the LV systolic pressure drops, thereby reducing the
transmitral pressure gradient.
• In addition, reverse LV remodelling can be initiated as early as the
postoperative period, which contributes to reduced mitral
regurgitation.
Regeer et al. J.Am.Echocardiogr.2015.
• Primary MR is less likely than secondary regurgitation to improve
after aortic valve replacement.
Toggweiler, S. et al. J . Am. Coll. Cardiol.2012.

• The use of self-expanding valves seems to be associated with
less improvement in mitral regurgitation than balloon-
expandable valves.
• Finding explained by anatomical or functional interference
with mitral leaflet excursion annulus geometry, or by the
increased incidence of LV dyssynchrony resulting from left
bundle branch block or pacemaker insertion.
Nombela-Franco et al. Heart, 2015.

• Secondary TR - independent predictor of long-term mortality.
• Mitral and aortic valve replacement tend to decrease pulmonary vascular pressures and so reduce right ventricular overload.
• Conservative management of moderate secondary TR has been postulated.
Nath, et al J. Am. Coll. Cardiol. 2004.
• Presence of untreated moderate-to-severe TR at the time of aortic or mitral valve surgery is associated with reduced postoperative survival.
• Redo surgery for secondary TR is associated with operative mortality of 10–25%.

CHOICE OF SURGICAL TECHNIQUE
• VALVE REPAIR OR REPLACEMENT ???
• In a propensity-matched analysis of patients with aortic and mitral valve lesions, aortic valve replacement and mitral valve repair improved late survival compared with replacement of both valves.
Gillinov et al.. J. Thorac. Cardiovasc. Surg. 2003.
• In another study of patients with rheumatic heart disease, mitral valve repair plus aortic valve replacement improved event-free survival compared with double-valve replacement.
Talwar, et al Ann. Thorac. Surg. 2007.

• STS database.
• Mitral valve repair - 46%,
• Patients had a 39% reduction in the risk of operative mortality
compared with those undergoing mitral valve replacement,
despite them being of older age, with a lower LVEF, and a
higher incidence of concomitant CABG surgery.
Thourani, et al. Ann. Thorac. Surg. 2014.

Controversy exists, whether repair or replacement of the mitral
valve is preferred in patients who have moderate-to-severe
secondary MR and are undergoing AVR
• In one study, reduced
in-hospital mortality was
reported with mitral valve
repair (11% versus 18% for
replacement), but survival
after discharge from hospital
did not differ significantly
between the two strategies
• In two other studies mitral
valve replacement was
associated with better
freedom from recurrent
secondary ischaemic mitral
regurgitation during
follow-up compared with
mitral valve repair.
Leavitt et al Circulation 2009. Acker et al. N. Engl. J. Med 2014.
Magne, J. et al. Circulation 2009.

• In patients undergoing double-valve replacement, using the same type of prosthesis in both locations (bioprosthesis or mechanical) has been recommended.
• To avoid superimposing the risk of anticoagulation and the risk of bioprosthesis deterioration.
Roberts et al Am. J. Cardiol.1986.
• Tricuspid annuloplasty - tricuspid regurgitation at the time of left-sided valve surgery, as TR (annulus dilatation with ensuing lack of leaflet coaptation).
• Moreover, tricuspid annuloplasty is associated with a lower rate of complications than tricuspid valve replacement.
Arsalan et al Eur. Heart J.2015

PERCUTANEOUS APPROACHES
• Percutaneous treatment of aortic stenosis and mitral
regurgitation is increasingly used in patients at high surgical
risk.
• In selected patients, a staged approach has been proposed —
the valve stenosis is treated first by TAVI, followed by
subsequent implantation of a MitraClip if moderate-to-severe
MR with symptoms persists.
• This strategy has been associated with good procedural
success rates and, at 6 months, acceptable functional outcomes
and survival.
Kische et al.Catheter. Cardiovasc. Interv. 2013.

• In patients with severe AS undergoing TAVI, the concomitant
MS is generally of degenerative aetiology (that is, mitral
annulus calcification) with significant thickening and
calcification of the subvalvular apparatus, and absence of
commissural fusion.
• So not suitable for percutaneous mitral commissurotomy.
Vahanian et al. EuroIntervention 2015.

THE HEART VALVE TEAM
• The numerous diagnostic pitfalls, emergence of innovative
transcatheter therapies, and treatment of elderly high-risk
patients with multiple comorbidities require the expertise of a
multidisciplinary heart valve team.
• Expertise in cardiac surgery, transcatheter interventions, cardiac
imaging, haemodynamics, anaesthesia, and geriatrics is critical to
making the best recommendations and tailoring treatment strategies
to optimize outcomes for individual patients.
Lancellotti et al Eur. Heart J. 2013.

HEART VALVE TEAM CONSIDERATIONS
Life expectancy of the patient
Nature and severity of symptoms
Which valve lesion is dominant
Aetiology and severity of each valve lesion
Size and function of the left and right ventricles
Presence and severity of pulmonary hypertension
Anticipated progression of a secondary valve lesion if left untreated
Transcatheter options
Staged procedures versus all-at-once treatment
Procedural risk
Local experience of the treatment team
Patient wishes

CLINICAL SCENARIOS
• Three main clinical scenarios are encountered in clinical
practice —
1. Patients with two or more severe lesions,
2. Patients with one severe lesion plus at least one nonsevere
lesion,
3. Patients with two or more nonsevere lesions.

RECOMMENDATIONS

INDICATIONS FOR CONCOMITANT VALVE SURGERY
IN PATIENTS UNDERGOING SURGERY ON ANOTHER
VALVE


TWO OR MORE SEVERE LESIONS
• Two or more severely stenotic or regurgitant lesions, and who
are symptomatic or have ventricular dysfunction or dilatation,
should be be surgically corrected concomitantly.
• Patients at high or prohibitive risk of surgery, alternative
treatment pathways have been proposed.
• In such cases, the staged percutaneous approach involving the
MitraClip might be considered.

ONE SEVERE LESION PLUS AT LEAST ONE
NONSEVERE LESION

AHA/ACC AND ESC/EACTS GUIDELINES for performing a second
surgical valve procedure in patients undergoing surgery for another
valve lesion or other cardiac surgery.
CLASS IIA
• Moderate aortic stenosis,
• Moderate aortic regurgitation,
• Moderate primary mitral
regurgitation,
• Moderate primary or
secondary tricuspid
regurgitation (provided that
tricuspid annulus is dilated)
CLASS IIB
• Moderate mitral stenosis,
• Moderate secondary mitral
regurgitation,
• Moderate tricuspid
regurgitation (in the presence
of pulmonary artery
hypertension)

Management of severe aortic stenosis requiring surgery, with concomitant mitral regurgitation.
Mitral regurgitation is highly likely to improve with aortic valve replacement in the absence of
atrial fibrillation, left atrial dilatation, or pulmonary hypertension. *A staged approach is
possible, consisting of TAVI followed by implantation of a MitraClip. if symptomatic mitral
regurgitation persists.

Management of TR in patients undergoing left-sided valve surgery. Indications for surgery on the
tricuspid valve according to the severity and aetiology ( 1º versus 2º ) of TR, and to the presence
of tricuspid annulus dilatation / PH.
Nishimura et al. 2014 AHA/ACC guidelines J. Am. Coll. Cardiol. 2014.

TWO OR MORE NONSEVERE LESIONS
• In patients with nonsevere MVD, determining the global
consequences of all lesions is of the utmost importance.
• Moderate lesions, when combined, can lead to severe functional
intolerance, symptoms, LV dilatation or dysfunction, and pulmonary
hypertension.
• Consequences of the overall haemodynamic burden on the cardiac
chambers, pulmonary circulation, and patient’s functional capacity
should be assessed.
• Surgery - appropriate for selected patients in whom the combination
of moderate lesions has a meaningful effect on the functional
parameters such as maximal exercise capacity and peak oxygen
consumption and pulmonary arterial pressures.

KEY POINTS
MVD is a prevalent form of valvular heart disease;
a. Rheumatic heart disease - developing countries,
b. Degenerative aetiologies - developed countries.
Haemodynamic interactions between valve lesions can
promote, exacerbate, or, by contrast, blunt the clinical
expression of each singular lesion.

Several diagnostic tools used for the assessment of valve
stenosis or regurgitation have been validated in patients with
single-valve disease, but such tools might not be valid for
MVD.
Therapeutic decisions should be made by a heart valve team,
considering the severity of MVD, the patient’s life expectancy
and comorbidities, and the risks of multiple prostheses and
eventual reoperation.
The introduction of transcatheter valve therapies is changing
the therapeutic paradigm, but further studies are needed to
guide therapeutic decision-making.