Embed Size (px)
Citation preview

Diagnostic Radiology of Diagnostic Radiology of Musculoskeletal SystemMusculoskeletal System
Zhang ZhaohuiZhang Zhaohui
Department of RadiologyDepartment of Radiology
The First Affiliated Hospital of Sun Yat-sen UniversityThe First Affiliated Hospital of Sun Yat-sen University

FractureFracture

Definition:Definition: complete or incomplete break in the complete or incomplete break in the continuity of bone or cartilage continuity of bone or cartilage
Clinical presentation:Clinical presentation: traumatic history, local traumatic history, local tenderness, swelling, functionally disorder, deformitytenderness, swelling, functionally disorder, deformity
Radiological appearance:Radiological appearance: fracture line fracture line
General introduction of fractureGeneral introduction of fracture

ClassificationClassification
Complete versus incompleteComplete versus incomplete Complete fractures involves the entire circumference (tubComplete fractures involves the entire circumference (tub
ular bone) or both cortical surfaces (flat bone) of a bone. It ular bone) or both cortical surfaces (flat bone) of a bone. It can be subdivided into several types, such as transverse, obcan be subdivided into several types, such as transverse, oblique, spiral fracture. In incomplete fracture , the break in tlique, spiral fracture. In incomplete fracture , the break in the cortex does not extend completely through the bone.he cortex does not extend completely through the bone.
Comminution fractureComminution fracture Fracture with more than two fragments are comminution Fracture with more than two fragments are comminution
fracture. fracture.

Transverse Transverse fracturefracture

Oblique Oblique fracturefracture

Spiral fractureSpiral fracture

Spiral fractureSpiral fracture

Comminution Comminution fracture fracture

Incomplete fractureIncomplete fracture
The break in the cortex The break in the cortex does not extend completely does not extend completely through the bonethrough the bone

PositionPosition By convention, long bones are divided into thirds, aBy convention, long bones are divided into thirds, a
nd lesions are described as being in the proximal, mind lesions are described as being in the proximal, middle, or distal third or at the junction of the proximal ddle, or distal third or at the junction of the proximal and middle or middle and distal third. and middle or middle and distal third.
If a fracture is located near an articular cortex, it shoIf a fracture is located near an articular cortex, it should be described as either intra- or extra-articular.uld be described as either intra- or extra-articular.

AppositionApposition
The term apposition refers to the state of contact of The term apposition refers to the state of contact of the ends of the fracture fragments. Complete and the ends of the fracture fragments. Complete and normal apposition is termed anatomical apposition.normal apposition is termed anatomical apposition.
Displacement: If fracture fragments are in partial Displacement: If fracture fragments are in partial apposition, the term displacement is used. By apposition, the term displacement is used. By convention, the distal fragment is said to be convention, the distal fragment is said to be displaced in the designated direction with respect displaced in the designated direction with respect to the proximal fragment. to the proximal fragment.

Fracture at the junction Fracture at the junction of the proximal and of the proximal and middle third of femoramiddle third of femora
There is later There is later displacement of distal displacement of distal fragment with respect to fragment with respect to the proximal fragment.the proximal fragment.

Bayonet apposition refers to a fracture in which the Bayonet apposition refers to a fracture in which the fragment ends are not in contact with one another but fragment ends are not in contact with one another but the fragments overlap one another, leaving the shafts the fragments overlap one another, leaving the shafts of the fragments in contact and causing loss of length of the fragments in contact and causing loss of length of involved bone.of involved bone.

Fracture at the junction Fracture at the junction of the middle and distal of the middle and distal third of tibia and fibula third of tibia and fibula with bayonet apposition with bayonet apposition
There is also anterior There is also anterior and later displacement of and later displacement of distal fragment with distal fragment with respect to the proximal respect to the proximal fragment. fragment.

Distraction is complete lDistraction is complete lack of apposition, and mack of apposition, and most commonly secondary ost commonly secondary to either excessive tractioto either excessive traction or interposed tissue. In n or interposed tissue. In a non-acute fracture, the a non-acute fracture, the appearance of distraction appearance of distraction may be due to resorption may be due to resorption of the ends of the fragmeof the ends of the fragments.nts.

AlignmentAlignment
Alignment refers to the relationship of the long axes of the fracturAlignment refers to the relationship of the long axes of the fracture fragments. Loss of normal alignment is angulation. Direction of e fragments. Loss of normal alignment is angulation. Direction of angulation may be correctly described in two ways. The least confangulation may be correctly described in two ways. The least confusing description is the direction of angulation of the apex of the fusing description is the direction of angulation of the apex of the fracture site. Alternatively, angulation of the distal fragment with rracture site. Alternatively, angulation of the distal fragment with respect to the proximal one may be described. These two descriptioespect to the proximal one may be described. These two descriptions are exactly reversed in a given fracture. ns are exactly reversed in a given fracture. For example, a fracture For example, a fracture of the femur pointing anteriorly would be described either as apex of the femur pointing anteriorly would be described either as apex anterior angulation or as posterior angular displacement of the distanterior angulation or as posterior angular displacement of the distal fragment. Either description is correct as long as it is clearly staal fragment. Either description is correct as long as it is clearly stated. ted.

Fracture at the middle tFracture at the middle third of tibia and fibula hird of tibia and fibula with apex anterior anguwith apex anterior angulationlation
There is anterior displaThere is anterior displacement of the distal faccement of the distal facture fragment of tibia wture fragment of tibia with respect to the proxiith respect to the proximal fragment.mal fragment.
The aposition of fractuThe aposition of fracture fragments of fibula ire fragments of fibula is normal. s normal.

RotationRotation Rotation of fracture fragments can be evaluated by cRotation of fracture fragments can be evaluated by comparison of the direction of the joints proximal and omparison of the direction of the joints proximal and distal to the fracture. If this is not possible, malrotatiodistal to the fracture. If this is not possible, malrotation can often be inferred from a radiograph if the antern can often be inferred from a radiograph if the anteroposterior and lateral diameters of a long bone are difoposterior and lateral diameters of a long bone are different and the fracture fragments do not appear congrferent and the fracture fragments do not appear congruent. uent.

Healing of fractureHealing of fracture
Healing of fracture begins with the immediate hemoHealing of fracture begins with the immediate hemorrhage in and around it. This is followed by ingrowtrrhage in and around it. This is followed by ingrowth of granulation tissue, the formation of an osseous h of granulation tissue, the formation of an osseous and sometimes cartilaginous matrix, decalcification and sometimes cartilaginous matrix, decalcification and resorption of the devitalized bone in the opposinand resorption of the devitalized bone in the opposing ends of the fragments, progressive calcification of g ends of the fragments, progressive calcification of the osseous and cartilaginous matrix (callus formatiothe osseous and cartilaginous matrix (callus formation) and finally, shaping of the shaft at the junction of n) and finally, shaping of the shaft at the junction of the fragments.the fragments.

Formation of a small amount of calli arFormation of a small amount of calli around the fracture of clavicleound the fracture of clavicle
Factors that have influence Factors that have influence on the healing of fracture on the healing of fracture include age, fracture type, include age, fracture type, nutrition, treatment, etc.nutrition, treatment, etc.
Callus usually cannot be Callus usually cannot be detected earlier than the 3rd detected earlier than the 3rd week after fracture in older week after fracture in older children or adults but children or adults but becomes visible during the becomes visible during the 2nd week in the new born.2nd week in the new born.

Formation of caFormation of calli around the frlli around the fracture at distal tacture at distal third of radiushird of radius

Development of callus: more opaque, more clearly defined, and Development of callus: more opaque, more clearly defined, and take a fusiform shapetake a fusiform shape

Bony union of the fBony union of the fracture at proximal racture at proximal humerushumerus
Disappearance of fracturDisappearance of fracture line, anatomical apposite line, anatomical apposition, normal alignment, slion, normal alignment, slight irregularity of humeright irregularity of humerus at the fracture site.us at the fracture site.

Complications of fracturesComplications of fractures include: un-union or delaye include: un-union or delayed union; deformity of union; osteoporosis after trauma; id union; deformity of union; osteoporosis after trauma; infection of bone and joint; necrosis of bone; degeneratinfection of bone and joint; necrosis of bone; degeneration of joint; myositis ossificans, etc. on of joint; myositis ossificans, etc.

Un-union fractureUn-union fracture
The opposing ends of The opposing ends of fracture fragments fracture fragments become thin with become thin with increased densityincreased density

Deformity of Deformity of unionunion

Deformity of union Deformity of union with post-traumatic with post-traumatic osteoporosisosteoporosis

Un-union of femoral Un-union of femoral neck fracture with neck fracture with necrosis of femoral head necrosis of femoral head (collapse of femoral (collapse of femoral head with increased head with increased density)density)

Post fracture Post fracture myositis ossimyositis ossificansficans
Radiographs Radiographs show high deshow high density ossificansity ossifications in the stions in the soft tissue oft tissue (())

Greenstick fractureGreenstick fracture
An incomplete fracture in the developing tubular An incomplete fracture in the developing tubular bone caused by bending stress.bone caused by bending stress.
Greenstick fractures are characterized by angling or Greenstick fractures are characterized by angling or buckling of the cortex , and a lucent fracture line buckling of the cortex , and a lucent fracture line often invisible. often invisible.
Common fracturesCommon fractures

Radiographs Radiographs show angling show angling (lateral view) (lateral view) and slight and slight buckling (AP buckling (AP view) of the view) of the cortex of distal cortex of distal third of radius third of radius without a lucent without a lucent fracture line.fracture line.
Green stick Green stick fracturefracture

Epiphyseal separationsEpiphyseal separations
Epiphysis and most of the cellular elements of the Epiphysis and most of the cellular elements of the contiguous growth plate separate from the metaphcontiguous growth plate separate from the metaphysis. In an older child, it may create a metaphyseal ysis. In an older child, it may create a metaphyseal fragment. fragment.

The lateral radiograThe lateral radiograph shows posterior dph shows posterior displacement of epiphisplacement of epiphysis with no radiogrysis with no radiographically visible ossaphically visible osseous fragments.eous fragments.

Epiphyseal separation of Epiphyseal separation of proximal phalange with a proximal phalange with a small metaphyseal osseosmall metaphyseal osseous fragmentus fragment

Epiphyseal separation of medEpiphyseal separation of medial epicondyle of distal humeial epicondyle of distal humerusrus
Normal elbow jointNormal elbow joint

Colles fractureColles fracture
Distal metaphysis of radius Distal metaphysis of radius Within 2cm of articular surfaceWithin 2cm of articular surface Dorsal displacement & apex anterior angulation Dorsal displacement & apex anterior angulation Radial dispacement & shorteningRadial dispacement & shortening ConcomitantConcomitant fracture of styloid process of ulnafracture of styloid process of ulna ConcomitantConcomitant dislocation of distal radioulnardislocation of distal radioulnar joint

Colles fractureColles fracture

Colles fracture with concomitant fracture of styloid process of ulColles fracture with concomitant fracture of styloid process of ulna and dislocation of distal radioulnarna and dislocation of distal radioulnar jointjoint

Supracondylar fractureSupracondylar fracture
A transverse metaphyseal fracture of the distal A transverse metaphyseal fracture of the distal humerushumerus
Commonest elbow fracture in childhood Commonest elbow fracture in childhood Extension type: transcondylar fracture with Extension type: transcondylar fracture with
posterior and proximal displacement and apex posterior and proximal displacement and apex anterior angulation (95%)anterior angulation (95%)
Flexion type: Flexion type: anterior displacementanterior displacement and apex apex posterior angulationposterior angulation
Fat pad displacement indicating a joint effusionFat pad displacement indicating a joint effusion

Supracondylar frSupracondylar fracture with posteacture with posterior displacement rior displacement of distal fragmenof distal fragment and slight t and slight apex apex anterior anterior angulationangulation

Supracondylar Supracondylar fracture with mfracture with minimal displaceinimal displacementment

fat pad fat pad displacmentdisplacment

Compression fractureCompression fracture Wedge-shaped vertebral body with anterior part Wedge-shaped vertebral body with anterior part
being compressedbeing compressed Increased-density line instead of the fracture line Increased-density line instead of the fracture line Adjacent vertebral discs intactAdjacent vertebral discs intact Stable lesion unless more than 30% compressionStable lesion unless more than 30% compression
Vertebral FractureVertebral Fracture

Compression fracture of C6 vertebral bodyCompression fracture of C6 vertebral body

Compresion fracture of T12 vertebral body with kyphosisCompresion fracture of T12 vertebral body with kyphosis

Burst FractureBurst Fracture
Caused by axial compression, which drives Caused by axial compression, which drives the vertebral disc into the vertebral body the vertebral disc into the vertebral body below it, causing it to shatter. below it, causing it to shatter.
It is an unstable lesion. The prognosis depends It is an unstable lesion. The prognosis depends upon the displacement of the posterior aspect upon the displacement of the posterior aspect of the vertebral body and whether the of the vertebral body and whether the vertebral arches are intact. vertebral arches are intact.
Vertebral FractureVertebral Fracture

CT is of considerable value in evaluating the CT is of considerable value in evaluating the posterior elements, classifying injuries, and posterior elements, classifying injuries, and determining the site for vertebral determining the site for vertebral decompression. CT scanning is also able to decompression. CT scanning is also able to identify small cortical breaks. identify small cortical breaks.
MR is valuable in detecting injury of spinal cord MR is valuable in detecting injury of spinal cord and ligament. and ligament.
Vertebral FractureVertebral Fracture

Comminution fracture of vertebral body with posterior diComminution fracture of vertebral body with posterior displacement of fracture fragments. Right posterior elemensplacement of fracture fragments. Right posterior elemen
tsts are also involved.are also involved.

T1WI T2WI
Fracture of L2 Fracture of L2 vertebral body vertebral body with injury of with injury of adjacent spinal adjacent spinal cordcord

Tumor and tumor like lesionsTumor and tumor like lesions

DefinitionDefinition Malignant tumor with ability to produce osteoid Malignant tumor with ability to produce osteoid
or immature bone directly from neoplastic cellsor immature bone directly from neoplastic cells
EtiologyEtiology Of unknown etiology = primary (majority )Of unknown etiology = primary (majority ) Secondary to predisposing factors (Paget disease, Secondary to predisposing factors (Paget disease,
bone infarct, radiation) = secondarybone infarct, radiation) = secondary
Osteosarcoma

DemographicsDemographics Age: second and third decades of life (children and adolescentAge: second and third decades of life (children and adolescent
s)s) Gender: Gender: M:F=2:1M:F=2:1
Skeletal locationSkeletal location
Metaphysis of long tubular boneMetaphysis of long tubular bone
Femur(40%), tibia(16%), and humerus(15%)Femur(40%), tibia(16%), and humerus(15%)

Clinical presentationClinical presentation Soft tissue mass, pain, swelling, warmth, and rSoft tissue mass, pain, swelling, warmth, and r
estriction of motionestriction of motion
Pathological fracturePathological fracture
Increased serum alkaline phosphataseIncreased serum alkaline phosphatase
Early metastasis: lungs , bones and other sitesEarly metastasis: lungs , bones and other sites

Radiographic findingsRadiographic findings
The pattern of osseous involvement depends to a large The pattern of osseous involvement depends to a large extent on the amount of immature bone produced by the extent on the amount of immature bone produced by the tumor. A mixed pattern consisting of both osteolysis and tumor. A mixed pattern consisting of both osteolysis and osteosclerosis is most typical, with purely osteolytic or oosteosclerosis is most typical, with purely osteolytic or osteosclerotic lesions being encountered less frequently.steosclerotic lesions being encountered less frequently.

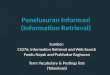
Radiograph shows a lesion witRadiograph shows a lesion with osteosclerosis and osteolysis. h osteosclerosis and osteolysis. Note the Codman triangle( ).Note the Codman triangle( ).
Osteosarcoma on the Osteosarcoma on the upper third of tibia (upper third of tibia (mixed pattern)mixed pattern)

Radiographic findingsRadiographic findings Ill-defined intramedullary, metaphyseal lesionIll-defined intramedullary, metaphyseal lesion Formation of immature bone by tumorFormation of immature bone by tumor Bone destructionBone destruction Soft tissue massSoft tissue mass Aggressive periosteal reaction: Aggressive periosteal reaction:
Codman triangle Codman triangle Sunburst patternSunburst pattern

Osteosarcoma on the loOsteosarcoma on the lo
wer third of femurwer third of femur (oste(osteosclerotic pattern)osclerotic pattern)

Radiograph Radiograph shows shows ivory-like ivory-like appearance.appearance.
Osteosarcoma Osteosarcoma on the femur (on the femur (osteosclerotic osteosclerotic pattern)pattern)

Osteosarcoma of the femur (osteosclerotic pattern) with multiple pulmonary metastases

Osteosarcoma on the Osteosarcoma on the lower third of femur lower third of femur (osteolytic pattern)(osteolytic pattern)
Radiograph shows bone Radiograph shows bone destruction in the distal destruction in the distal metaphysis and diaphysimetaphysis and diaphysis of the femur, with soft s of the femur, with soft tissue mass and Codman tissue mass and Codman triangle( ).triangle( ).

Radiographic findingsRadiographic findings
Conventional radiograph is essential in estabConventional radiograph is essential in establishing the specific diagnosis of osteosarcoma, lishing the specific diagnosis of osteosarcoma, but often cause underestimation of the extent obut often cause underestimation of the extent of the tumor, both within and outside the bone.f the tumor, both within and outside the bone.

Other imaging techniquesOther imaging techniques
CT and MR imaging are more useful in defining CT and MR imaging are more useful in defining the extent of tumor and its relationship to the extent of tumor and its relationship to surrounding neurovascular structures and in surrounding neurovascular structures and in
evaluating the response of the tumor to therapy.evaluating the response of the tumor to therapy.

CTCT Intramedullary and soft tissue extentIntramedullary and soft tissue extent Lesions in complex osseous structures Lesions in complex osseous structures such as such as
pelvis, scapula, or spinepelvis, scapula, or spine
Other imaging techniquesOther imaging techniques

Osteosarcoma on the lower tOsteosarcoma on the lower third of femurhird of femur

MRIMRI Signal: Low on TSignal: Low on T11WI and high on TWI and high on T22WIWI
Evident enhancementEvident enhancement Detecting skip lesionsDetecting skip lesions Superior to CT in defining the intraosseous and Superior to CT in defining the intraosseous and
extraosseous extent of the tumor extraosseous extent of the tumor
Other imaging techniquesOther imaging techniques

Skip lesions Skip lesions
synchronous foci of tumor that are synchronous foci of tumor that are anatomically separate from the primary anatomically separate from the primary lesion and that occur within the same lesion and that occur within the same bone or on the other side of a jointbone or on the other side of a joint

T1WI T1WI
T2WI
+C
Osteosarcoma Osteosarcoma on the upper ton the upper third of tibiahird of tibia

Osteosarcoma with skip lesionsOsteosarcoma with skip lesions

PearlsPearls
• Producing osteoid or immature bone directlyProducing osteoid or immature bone directly• Affects patients in their teens and twenties Affects patients in their teens and twenties • Favors the metaphysis of long tubular boneFavors the metaphysis of long tubular bone• Plain film : essential for diagnosisPlain film : essential for diagnosis
Bone destruction, formation of immature boneBone destruction, formation of immature bone soft tissue mass, aggressive periosteal reactionsoft tissue mass, aggressive periosteal reaction
• Other modalities : determining extent of diseaseOther modalities : determining extent of disease


Definitions Definitions
Locally aggressive neoplasm composed of osteoclast Locally aggressive neoplasm composed of osteoclast like giant cells, usually involving the end of mature llike giant cells, usually involving the end of mature long boneong bone
EtiologyEtiology: Unknown: Unknown
StagingStaging : Latent, Active, Aggressive : Latent, Active, Aggressive
Giant cell tumor of bone

DemographicsDemographics
Age: 20~40 yearsAge: 20~40 years
Gender: F: M=2:1Gender: F: M=2:1
Skeletal locationSkeletal location
Ends of mature long boneEnds of mature long bone
Knee joint and distal end of radiusKnee joint and distal end of radius

Clinical presentationClinical presentation
Pain and swelling at affected areaPain and swelling at affected area
Pathologic fracture in 30%Pathologic fracture in 30%
Limited range of motion of adjacent joint Limited range of motion of adjacent joint
Pulmonary metastases :1-2%Pulmonary metastases :1-2%

GCT of radiusGCT of radius

Radiographic findingsRadiographic findings
Expansile, lytic epiphyseal lesion extending to subchonExpansile, lytic epiphyseal lesion extending to subchondral bone, with well-defined marginsdral bone, with well-defined margins
Periosteal reaction and sclerotic rim: uncommonPeriosteal reaction and sclerotic rim: uncommonWithout calcification or ossificationWithout calcification or ossificationPeripheral trabeculae — multi-locular appearancePeripheral trabeculae — multi-locular appearance

Radiographs show a well defined lytic lesion at upper end of tibia witRadiographs show a well defined lytic lesion at upper end of tibia with pathological fracture ( ). There is no sclerosis, no periosteal reactioh pathological fracture ( ). There is no sclerosis, no periosteal reaction, and no calcificationn, and no calcification
GCT of tibiaGCT of tibia

Pathological fracturePathological fracture
Fracture occurring at a site of previous Fracture occurring at a site of previous abnormality, often by means of a stress that abnormality, often by means of a stress that would not normally causewould not normally cause fracture.fracture.

GCT of tibiaGCT of tibia

Radiographs show expansile and lytic lesion with cortical break Radiographs show expansile and lytic lesion with cortical break through and formation of soft tissue mass ( ).through and formation of soft tissue mass ( ).
GCT of radiusGCT of radius

CT findingsCT findings
Soft tissue attenuation, foci of low attenuationSoft tissue attenuation, foci of low attenuation
Breakthrough of cortex with soft tissue invasionBreakthrough of cortex with soft tissue invasion
MRI findingsMRI findings
Low-intermediate signal intensity on T1WI and T2WILow-intermediate signal intensity on T1WI and T2WI
Strong enhancementStrong enhancement

GCT of femurGCT of femur

T1WI T2WI
T1WI T2WI + C
GCT of tibiaGCT of tibia

PearlsPearls
• Locally aggressive neoplasmLocally aggressive neoplasm• Favoring the Favoring the ends of mature long bonesends of mature long bones• Occurring most frequently in 20-40Occurring most frequently in 20-40• Imaging findings : Imaging findings : expansile, lytic epiphyseexpansile, lytic epiphyse
al lesion extending to subchondral bone, withal lesion extending to subchondral bone, without calcification or ossificationout calcification or ossification

Definition:Definition: Fluid containing lesion of bone, lined by m Fluid containing lesion of bone, lined by mesenchymal cellsesenchymal cells
Etiology:Etiology: tumor like lesion of unknown etiology, attrib tumor like lesion of unknown etiology, attributed to local disturbance of bone growthuted to local disturbance of bone growth
Simple bone cyst

LocationLocation Metaphysis, migration to diaphysis with growthMetaphysis, migration to diaphysis with growth Humerus and femurHumerus and femur
DemographicsDemographics Age: children and adolescentsAge: children and adolescents Gender: M:F=2-3:1Gender: M:F=2-3:1

Clinical presentationClinical presentation
Most lesions asymptomaticMost lesions asymptomatic
Pain, swelling, stiffness at closed jointPain, swelling, stiffness at closed joint
66% of cysts present with pathologic fractures66% of cysts present with pathologic fractures
Inactive, latent after skeletal maturityInactive, latent after skeletal maturity
Spontaneous regression in some casesSpontaneous regression in some cases

Simple bone cyst at upper Simple bone cyst at upper third of humerus with patthird of humerus with pathological fracturehological fracture

Radiographic findingsRadiographic findings
Centrally located, well-defined, expansile, lytic lesionCentrally located, well-defined, expansile, lytic lesion
Long axis parallel to that of host boneLong axis parallel to that of host bone
No periosteal reaction unless fracturedNo periosteal reaction unless fractured
No extension into soft tissuesNo extension into soft tissues
Fallen fragment sign secondary to pathologic fractureFallen fragment sign secondary to pathologic fracture
(a fragment of cortex falls into the fluid within the cavity of a bone cyst)(a fragment of cortex falls into the fluid within the cavity of a bone cyst)

Simple bone cyst at upper Simple bone cyst at upper third of humerus with patthird of humerus with pathological fracturehological fracture

CTCT findingsfindings
Fluid-filled cavityFluid-filled cavity
No enhancementNo enhancement
Helpful in evaluating anatomic complex areas Helpful in evaluating anatomic complex areas
Determination of extentDetermination of extent

Simple bone cyst at up third of femurSimple bone cyst at up third of femur

Bone cyst with fallen fragment signfallen fragment sign

MRI findingsMRI findings
T1WI: low to intermediate signal intensityT1WI: low to intermediate signal intensity
T2WI: high signal intensity;T2WI: high signal intensity;
Heterogeneous signal in case of fracture Heterogeneous signal in case of fracture
No enhancementNo enhancement

Simple bone cyst at up third of femurSimple bone cyst at up third of femur
T1WI T2WIradiograph

PearlsPearls Tumor like lesion of unknown etiologyTumor like lesion of unknown etiology Occurring in children and adolescentsOccurring in children and adolescents Common location: metaphysis, migration to diapCommon location: metaphysis, migration to diap
hysis with growthhysis with growth Imaging findings : Imaging findings : centrally located, well-definecentrally located, well-define
d, expansile, lytic lesion with long axis parallel td, expansile, lytic lesion with long axis parallel to that of host boneo that of host bone

Spread of malignant tumors to osseous strucSpread of malignant tumors to osseous struc
tures (usually through haematogenous dissetures (usually through haematogenous disse
minationmination)
Primary lesions : carcinoma of breast, lung, Primary lesions : carcinoma of breast, lung,
prostate, thyroid, kidney, prostate, thyroid, kidney, neuroblastomaneuroblastoma etc etc
Skeletal MetastasisSkeletal Metastasis

Age: middle-aged and elderly patientsAge: middle-aged and elderly patients
children younger than 5 (neuroblastoma)children younger than 5 (neuroblastoma)Skeletal locationSkeletal location
Spine, pelvis, ribs, skull, femur and humerus, etcSpine, pelvis, ribs, skull, femur and humerus, etc Involvement of bones distal to knee and elbow rareInvolvement of bones distal to knee and elbow rare
Clinical presentationsClinical presentations :: Pain, pathological fracture, etc.Pain, pathological fracture, etc.

Radiographic findingsRadiographic findings
Osteolytic pattern: multiple poorly defined or well Osteolytic pattern: multiple poorly defined or well defined osteolytic bone destruction, perhaps with sdefined osteolytic bone destruction, perhaps with soft tissue mass or pathological fracture, usually witoft tissue mass or pathological fracture, usually without periosteal reaction; destruction of pedicle and hout periosteal reaction; destruction of pedicle and vertebral body with intact intervertebral space.vertebral body with intact intervertebral space.

Osteolytic metastasisOsteolytic metastasisM
Radiograph shows osteolytic Radiograph shows osteolytic bone destruction at upper thibone destruction at upper third of humerus, lateral end of rd of humerus, lateral end of clavicle with formation of soclavicle with formation of soft tissue mass.ft tissue mass.

Multiple Multiple round bone round bone destruction in destruction in the skull the skull without without sclerosissclerosis
Osteolytic metastasisOsteolytic metastasis

Osteolytic destruction Osteolytic destruction of left 5, 6 rib with of left 5, 6 rib with formation of soft formation of soft tissue masstissue mass
Osteolytic metastasisOsteolytic metastasis

Osteolytic Osteolytic metastasismetastasis

Osteoblastic pattern: multiple round or patchy radiOsteoblastic pattern: multiple round or patchy radiodense lesion, or diffuse increased densityodense lesion, or diffuse increased density
Mixed patternMixed pattern :: osteolytic + osteoblasticosteolytic + osteoblastic

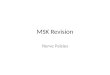
Radiograph shows multiple Radiograph shows multiple round or patchy radiodense round or patchy radiodense lesion in the pelvis and lumlesion in the pelvis and lumbar spine.bar spine.
Osteoblastic Osteoblastic metastasismetastasis

Radiograph shows diffuse increased density in pelvis, vertebral diffuse increased density in pelvis, vertebral body of lumbar spine and upper third of bilateral femursbody of lumbar spine and upper third of bilateral femurs
Osteoblastic Osteoblastic metastasismetastasis

Diffuse increased Diffuse increased density in vertebrdensity in vertebral body of L2, L4, al body of L2, L4, L5 , sacrum and ilL5 , sacrum and ilium.ium.
Osteoblastic Osteoblastic metastasismetastasis

Mixed Mixed pattern of pattern of skeletal skeletal metastasismetastasis

ItemsItems Benign tumorBenign tumor Malignant tumor Malignant tumor
GrowthGrowthSlow, compression and Slow, compression and displacement of adjacent displacement of adjacent tissue, without metastasistissue, without metastasis
Rapid, invasion of Rapid, invasion of adjacent tissue, adjacent tissue, metastasismetastasis
Osseous Osseous changeschanges
Well defined bone Well defined bone destruction, thinning of destruction, thinning of cortex without interruptioncortex without interruption
Ill defined and infiltrative Ill defined and infiltrative bone destruction, break bone destruction, break through of cortex, through of cortex, immature bone produced immature bone produced by tumorby tumor
Periosteal rPeriosteal reactioneaction
Uncommon, secondary to Uncommon, secondary to pathologic fracture, without pathologic fracture, without destruction by tumordestruction by tumor
Various pattern, Various pattern, destruction by tumordestruction by tumor
soft tissue soft tissue massmass
Uncommon, well defined if Uncommon, well defined if present present
Common, ill definedCommon, ill defined
Comparison of benign and malignant bone tumorsComparison of benign and malignant bone tumors

Thank you for Thank you for
your attentionyour attention !!