Embed Size (px)
Citation preview

Morning Report - 2November 3, 2016
Khushboo Gandhi, PGY2Internal Medicine, St. Luke’s Hospital

33 year old CF presents with nausea, vomiting and diarrhea.
HPI: 09/23/2016 4:50 PM
She was in her usual state of health until 2 pm today.
She works as a school bus driver for special needs children and while she was driving the bus, she began to feel very nauseated and had to pull over. She then began to vomit and have diarrhea. 5 times each
She had lunch which consisted of tuna noodle casserole at around noon.

Review of Systems in ED:
Constitutional: Weakness, No fever, No chills, No fatigue, No decreased activity, No loss of appetite, No weight gain. Eye: No recent visual problem, No double vision. Ear/Nose/Mouth/Throat: No decreased hearing, No ear pain, No nasal congestion, No sore throat. Respiratory: no shortness of breath, no cough, no sputum production, No hemoptysis. Cardiovascular: Tachycardia, No palpitations, No peripheral edema, no chest pain Gastrointestinal: Nausea, Vomiting, Diarrhea, No constipation, No abdominal pain. Genitourinary: No dysuria, No change in urine stream. Hematology/Lymphatics: No swollen lymph glands. Endocrine: No excessive thirst. Immunologic: Not immunocompromised. Musculoskeletal: No neck pain, No joint pain, No decreased range of motion. Integumentary: No rash, No pruritus, No petechiae, No skin lesion. Neurologic: Alert and oriented X4, No confusion, No numbness, No tingling, No headache. Psychiatric: Anxiety, Depression.

PMH/PSH: End stage renal disease secondary to heavy NSAID use + Reflux nephropathy (Recurrent UTI with pyelonephritis) (Took 55 tabs of Aleve in one day to relieve abdominal pain secondary to IUD in 2002) --- s/p CAPD since July 2016, Last dialysis at 11 AM today, due to start on cycler tonight first time Asthma/chronic bronchitis -- well controlled with albuterol inhaler as needed. No history of intubations secondary to asthma. Hospitalized once due to asthma , a year ago.Chronic migrainesDepression, AnxietyGout
Cholecystectomy, AV fistula creation x2 (was on HD for 3 weeks prior to PD but discontinued due to work schedule), Kidney stent, Peritoneal dialysis catheter insertion, Tonsillectomy, Mirena IUD insertion
Allergies: Advil- Renal failure.Aleve- Renal failure.Amoxicillin- Stopped breathing.Dilaudid- Itching, breathing problems.
Levaquin- Stopped breathing.Morphine- hives; Vicodin okPenicillin- Stopped breathing.

Family History: Mother - DM - Insulin controlled, Thyroid cancer
Social History: She is divorced and lives alone with her daughter. She works as a bus driver for special needs children. Former smoker, quit in 2004, smoked 10 cigs/day for 2 years, No alcohol intake, no drug abuse.
Meds: Albuterol: 2 puffs, Inhalation, q4hrs, PRN (shortness of breath)Aspirin: 81 mg, 1 tablet, Oral, dailyCholecalciferol: 2,000 units, Oral, dailySertraline: 100 mg, Oral, bid

Physical Examination in ED 8:30 PM:
Vitals: TMax: 36.9; HR: 126 regular; RR: 20; SpO2: 98 % on RA BP: 128/95 mm hg.Height: 152.4 cm Weight: 76.4 kg BMI:32.89
General: Alert and oriented, no acute distress Skin: Normal for ethnicity, No edema, Not pale. HENT: Normocephalic, Oral mucosa is moist, No pharyngeal erythema. Eye: Pupils are equal, round and reactive to light, Normal conjunctiva. Neck: Supple, No carotid bruit, No jugular venous distention, No lymphadenopathy. Respiratory: No chest wall tenderness, lungs are clear to auscultation, respirations are nonlaboredCardiovascular: Regular rhythm, No murmur, Tachycardia, Good pulses equal in all extremities, No edema. Gastrointestinal: Soft, Non-tender, Normal bowel sounds. Lymphatics: No lymphadenopathy neck, axilla, groin. Musculoskeletal: Normal range of motion, Normal strength, No swelling. Integumentary: Warm, Dry, Pink. Neurologic: Alert, Oriented, No focal defects. Psychiatric: Cooperative, Appropriate mood & affect. Genitourinary: No Costovertebral Angle tenderness.

HPI continues…
After arriving on floor, Nurse notifies NP on the floor that patient had become very short of breath and wheezing

Review of Systems on floor at 11:37 PM:
Constitutional: Weakness, No fever, No chills, No fatigue, No decreased activity, No loss of appetite, No weight gain. Eye: No recent visual problem, No double vision. Ear/Nose/Mouth/Throat: No decreased hearing, No ear pain, No nasal congestion, No sore throat. Respiratory: Shortness of breath, Cough, Wheezing, No hemoptysis. Cardiovascular: Tachycardia, No palpitations, No peripheral edema. Chest pain: Midsternal, Anterior. Gastrointestinal: Nausea, Vomiting, Diarrhea, No constipation, No abdominal pain. Genitourinary: No dysuria, No change in urine stream. Hematology/Lymphatics: No swollen lymph glands. Endocrine: No excessive thirst. Immunologic: Not immunocompromised. Musculoskeletal: No neck pain, No joint pain, No decreased range of motion. Integumentary: No rash, No pruritus, No petechiae, No skin lesion. Neurologic: Alert and oriented X4, No confusion, No numbness, No tingling, No headache. Psychiatric: Anxiety, Depression.

Physical Examination on floor at 11:27 PM:
Vitals: TMax: 36.9; HR: 104 regular; RR: 32; SpO2: 94 % on 2 L/m BP: 127/94 mm hg.Height: 152.4 cm Weight: 76.4 kg BMI:32.89
General: Alert and oriented, Severe distress, not able to complete full sentences. Skin: Normal for ethnicity, No edema, Not pale. HENT: Normocephalic, Oral mucosa is moist, No pharyngeal erythema. Eye: Pupils are equal, round and reactive to light, Normal conjunctiva. Neck: Supple, No carotid bruit, No jugular venous distention, No lymphadenopathy. Respiratory: No chest wall tenderness. Respiratory rate: 30 breaths/minute, Tachypneic. Pattern: Regular. Breath sounds: Right, Upper lobe, Lower lobe, Diminished, Expiratory wheezes, No crackles present. Right lower lung dull to percussionCardiovascular: Regular rhythm, No murmur, Tachycardia, Good pulses equal in all extremities, No edema. Gastrointestinal: Soft, Non-tender, Normal bowel sounds. Lymphatics: No lymphadenopathy neck, axilla, groin. Musculoskeletal: Normal range of motion, Normal strength, No swelling. Integumentary: Warm, Dry, Pink. Neurologic: Alert, Oriented, No focal defects. Psychiatric: Cooperative, Appropriate mood & affect. Genitourinary: No Costovertebral Angle tenderness.

CBC 09/23 09/24
WBC 8.7 H 11.4
RBC 4.43 4.21
Hemoglobin 13.1 12.3
Hematocrit 40.4 39.2
MCV 91.2 93.1
MCH 29.6 29.2
MCHC 32.4 L 31.4
RDW 13.3 13.5
MPV 10.8 10.6
Platelets 246 223
Diff 09/23 09/24
Neutro % 0.2 0.4
Lymph % 63 91
Mono % 28 5
Eos % 8 4
Baso % 1 0
Immature Gran % 0 0
Neutro # 5.5 H 10.3
Lymph # 2.4 L 0.5
Mono # 0.7 0.5
Eos # 0.1 0.0
Baso # 0.0 0.0Sed rate 28
General Chemistry 09/23 09/24
Sodium 140 144
Potassium 3.9 f C 2.8
Chloride 102 104
Co2 26 L 17
Anion Gap 12 H 23
BUN H 23 H 20
Creatinine H 5.8 H 5.6
Glucose 95 H 246
Calcium 8.8 8.5
Protein, Total 7.2
Albumin 4.2
Alk Phos 79
Bilirubin, Total 0.7
AST 28
ALT 25
Phosphorus
eGFR L 8 L 9
eCrCl f 0.2 f 0.2
LD 416
Magnesium H 2.6
Labs:

Blood Gases 09/24 09/24
pH 7.40 L 7.33
pCo2 37 33
pO2 L 58 87
HCO3 23 L 17
O2 Sat L 91 97
L/min 2 3
Urine Analysis
UA Color Straw
UA Clarity Clear
UA SG 1.005
UA pH 7.0
UA LE A 1+
UA Nitrite Negative
UA Protein A 2+
UA Protein (Qual) A Trace
UA Glucose (Qual) Negative
UA Ketones Negative
UA Urobilinogen Negative
UA Bilirubin A Trace
UA Blood A 6-10
UA WBC <3
UA RBC A Rare
UA Bacteria A Moderate
Blood Culture Negative
Blood Culture Negative
Urine Culture Negative
Influenza Negative
Res. PCR Negative
Nasal MRSA Negative

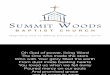
Development of a moderate right pleural effusion with right basilar atelectasis and/or infiltrate.

Overnight patient became extremely short of breath, unable to complete full sentences and was transferred to ICU in the morning following this x-ray finding

Fluid Analysis
Nucleated Cells f <50
RBC 2,000
Glucose f 497
LD f 222
Protein f <2.0
Hospital Course:
Pt was started on peritoneal dialysis cycler on the night of admission and developed acute respiratory distress due to severe right pleural effusion.
Patient was transferred to ICU, peritoneal dialysis was stopped and right thoracentesis was performed, with drainage of 3.2 L of fluid.
Fluid analysis was consistent with 1.5% Dianeal concentration PD solution.
Hydrothorax/Pleural effusion due to peritoneo-pleural leak.
IV antibiotics for possible pneumonia with aztreonam and vancomycin
Did receive Duonebs and steroid for one day due to concern for Asthma exacerbation
CT chest next day showed infiltrate in right upper lobe - Reexpansion edema
Vancomycin was discontinued and continued on aztreonam
She was started on hemodialysis and discharged home on 9/28/2016

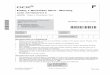
09/25 CT CHEST W/O CONTRAST
● Moderately large right pleural effusion. ● Trace left pleural effusion present. ● Infiltrate in the right upper lobe. ● Partial consolidation and atelectasis noted in
the right middle lobe and right lower lobe. ● Left basilar infiltrate and atelectasis noted. ● 0.2 m noncalcified nodule

“Sweet Hydrothorax”Acute Hydrothorax Complicating
Peritoneal Dialysis

PLEURAL EFFUSION DUE TO PLEUROPERITONEAL LEAK:
Hydrothorax associated with abnormal communications between the pleura and peritoneal cavities was first described by Meigs, who reported the coexistence of pleural effusion and ascites associated with ovarian fibroma
Typically occurs early in the course of PD
Not related to the volume of instilled dialysate
Source of the leak - Congenital or acquired communications between the pleura and the peritoneum
Diaphragmatic hernias allow dissection of fluid through defects around the major vessels and the esophagus or through diaphragmatic foramina
Negative intrathoracic pressure, combined with an increased intra-abdominal pressure caused by dialysate instillation, may open small defects in the diaphragm - promote the flow of dialysate into the pleural space.
Acquired diaphragmatic defects - eight years after starting peritoneal dialysis

Epidemiology:
Incidence is 1.6 to 10 percentlargest study reported to date - 50 of 3195 patients (1.6 percent) developed acute hydrothorax after
starting peritoneal dialysisWomen are affected more commonly than menPatients with polycystic kidney disease are predisposed to develop pleuroperitoneal leaks -
Significantly reduced abdominal capacity
Marked increase in hydrostatic pressure after the infusion of dialysate
Peritonitis increases the incidence of hydrothorax - 6% suffered peritonitis
Clinical characteristics:
Dyspnea and inadequate ultrafiltration abilityAsymptomatic (26 percent)Right side - 50 to 90 percent of casesMost appear early after the initiation of peritoneal dialysis
50% - within 30 days of starting PD
20% - after one year
Reported to occur one day to eight years after beginning PD

Diagnosis:
Dyspneic nonedematous patient Ultrafiltration is consistently inadequate
Modalities for the diagnosis of abdominal and thoracic cavity defects in peritoneal dialysis patients
PERITONEAL SCINTIGRAPHY
Safe, accurate, and rapid way of diagnosing leaks in the peritoneal cavity.3 to 5 millicuries of technetium 99m isotope per 0.5 to 2.0 L of dialysis solution is injected into the
abdominal cavity. Multiple projections (anterior, lateral, posterior, and oblique) are then taken to help diagnose leaks,
hernias, and hydrothorax Although a significant dose of isotope is used, it is not absorbed from the peritoneum, and almost all
of the material drains out of the body after the procedure. The net dose of radiation is therefore only a fraction of the total dose instilled into the peritoneal
cavity



CT SCANS AND CT PERITONEOGRAPHY
Accurate and reliable methods of diagnosing peritoneal defects. CTP Vs CTS - small leaks, adhesions, loculated fluid collections, intra abdominal abscesses, and
pseudocysts The dose of iodinated contrast - 50 mL per liter of dialysis fluid. Oral and intravenous (IV) contrast can be simultaneously given to diagnose any abscesses or tumors CTP is not effective in diagnosing obstruction of the catheter by fibrinous, adhesions or omentumRecommend CTP as the initial diagnostic modality to be utilized. Cumulative radiation exposure may be of concern in pediatric populations.
MRI AND MR PERITONEOGRAPHY
Gadolinium based dyeModerate to advanced renal failure (dialysis dependent or eGFR <30 mL/min) - severe syndrome of
nephrogenic systemic fibrosis.

CLINICAL METHODS:Easy to perform, but not sensitive enough to diagnose these defects
Thoracentesis Especially helpful in patients who are acutely symptomaticDiagnostic as well as therapeutic.Dialysate fluid in the pleura should have a higher concentration of glucose than plasma (50 mg/dl)Concentrations of lactate dehydrogenase (LDH) and protein are consistent with a transudateCell count and cultures (to exclude infection)L and D isomers of lactate - L isomer of lactate is endogenous
Commercial dialysis solutions have both L and D isomers
Methylene blue dye — Instillation of methylene blue dye into the peritoneum - useful in diagnosing leaks. Some case reports of irritation to the abdominal viscera
Clinical observation — An easier, but relatively insensitive method of diagnosing hydrothorax.keep the abdomen dry overnight and to repeat a chest radiograph in the morning to determine if the pleural effusion has decreased

Management:
Depends upon the acuity and severity of the patient's symptoms and desire to continue with peritoneal dialysis as a treatment modality
Acute thoracentesis to remove large pleural effusions is rarely required
Most cases - draining the peritoneal cavity and avoiding overnight (supine) dwells is sufficient
If the leak is small and the patient has adequate residual function to permit intermittent dialysis (eg, nocturnal peritoneal dialysis) - PD can be continued.
Continued - if estimated duration of dialysis is short, such as the patient who will soon undergo a living, related transplant
Some pleuroperitoneal leaks spontaneously resolve (after temporary transfer to hemodialysis) - Cure rate is only 40 percent with conservative therapy

Chemical pleurodesis - Recurrent pleural effusion, unresponsive to conservative measures, who needs and/or desires to continue with peritoneal dialysis
In one review, pleural effusion resolved after pleurodesis in 67 percent of patientsAgents - Autologous blood, talc, and tetracycline
Temporary cessation of CAPD - first-line treatment
Video-assisted thoracoscopic pleurodesis or repair - who failed conservative management
Surgical correction of an identified diaphragmatic defect - Thoracotomy
Most patients with pleuroperitoneal leaks ultimately require permanent transfer to hemodialysis

Noninfectious complications of continuous peritoneal dialysis
Continuous ambulatory peritoneal dialysis [CAPD] and Continuous cycler peritoneal dialysis [CCPD]
Due to increased intra abdominal pressure resulting from instillation of dialysate into the peritoneal cavityHernia formationLeaks (including hydrothorax or pleuroperitoneal leaks)Local edemaBack painGI problems: gastroesophageal reflux, delayed gastric emptying
Not related to increased intra abdominal pressureHemoperitoneumPain on infusion of dialysateElectrolyte imbalancesUltrafiltration failure

GERD - Increased intra abdominal pressure on lower esophageal sphincter
Delayed gastric emptying - mechanical or neurogenic mechanism triggered by the presence of intra abdominal fluid retards gastric emptying - metoclopramide/erythromycin
Back pain - Increased mechanical stress on the lumbar spine - due to the tendency of patients to assume a more lordotic position because of increased intra abdominal pressure
PAIN ON DIALYSATE INFUSION — Abdominal pain often occurs with infusion of dialysate into the peritoneal cavity even in the absence of peritonitis.
Acidic pH (pH 5.2 to 5.5) of conventional lactate dialysate.Poor catheter positionDialysate temperatureHigh glucose concentration of hypertonic dialysis solutions
Rx - May be treated with intraperitoneal infusion of bicarbonate/local anesthetic - Risk of contamination and peritonitis; Slowing the rate of infusion; Catheter replacement
Electrolyte abnormalities:Hypokalemia and hypermagnesemia liberalization of dietary potassium and, often, oral potassium supplementation may be needed.