Embed Size (px)
Citation preview

MITRAL VALVE SURGERY
CHORDAL PRESERVATION
Dr.JYOTINDRA SINGH
MBBS,MS,M.Ch( Cardiac surgery)

PLANINTRODUCTION
ANATOMY & PHYSIOLOGY
HISTORICAL ASPECT
EFFECTS OF CHORDAL PRESERVATION
PHYSIOLOGICAL ALTERATION
TECHNIQUES OF CHORDAL PRESRVATION
RESULTS
TAKE HOME MESSAGE

INTRODUCTION
Aim of mitral valve surgery - to provide a competent,
non-obstructed valve without compromising the left
ventricular (LV) function.
Above aims are met with valve repair .
When repair is not feasible- preservation of LV
function is an important concern.
Awareness of the deleterious effects of the loss of
annulo-ventricular continuity has increased, chordal
preservation has gained popularity

INTRODUCTION
Despite the clear advantages of complete chordal preservation ,many surgeons still
retain only the posterior leaflet because of greater
technical complexity,
longer operating time,
fear of potential interference with mechanical leaflet motion,
need to undersize the mitral prosthesis
possibility of LVOTO.
However, with application of the correct surgical technique tailored to suit the
individual patient, preservation of the entire subvalvular structures is feasible in all
patients with an adequate sized prosthesis.

INTRODUCTION



The left ventricle has been dissected so as to remove its posterior wall, and is viewed from
behind in anatomically appropriate orientation.
Anderson R H , Kanani M MMCTS
2007;2007:mmcts.2006.002147
© 2007 European Association for Cardio-thoracic Surgery

2
ANNULO VENTRICULAR CONTINUITYIn 1922, Wiggers and Katz and later Rushmer et al proposed the concept.
left ventricular geometry and function are a result of a dynamic interaction between the mitral annulus and the LV wall.
The attachments between the mitral annulus and the LV wall
moderate the LV distension during diastole and wall tension during systole.
When the papillary muscles contract during the isometric phase of the cardiac cycle,the closed MV is drawn into the LV cavity thus reducingthe longitudinal axis of the LV and increasing its short axis.
Diastolic recoil.


Annulo ventricular continuity


2
ANATOMY
Figure 42-5. Conventional mitral valve replacement with
complete excision of the leaflets and the entire subvalvular
apparatus, as used in the past and in cases of advanced
rheumatic disease. The mitral prosthesis is implanted using
a series of horizontal mattress sutures

2
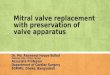
Effects of chordal transection
Hansen demonstrated that transection of chordae to the anterior mitral leaflet (AML) reduced the LV function to a greater degree as compared to the transection of chordae to the posterior mitral leaflet .
improved LV systolic performance by reduction of the LV afterload.
Chordal transection also appeared to shorten the long axis of the LV with an increase in the minor axis and dilatation of the chamber.
Transection of the chordae produced dyskinetic areas at the insertion
of severed papillary muscles
Sarris and colleagues - neo-chordal reconstruction at re-operation

Chordae and papillary muscle

Physiological changes
Chronic MR- LV function gradually declines.
Regurgitant stroke volume added to forward stroke
volume- increase EF in early phase.
Progressive LV dilatation- increase Afterload.
After MVR with chordal transection- EF determined by
contractility,preload ,afterload.


2
Historical aspect
In 1964, Lillehei introduced the concept of chordal preservation during MVR to reduce the problem of post-operative low cardiac output syndrome.
David in 1981 reintroduced the concept- LV function deteriorated if the chordae were transected .
Only those patients in whom the chordae had been spared could increase the LV ejection fraction (EF) and stroke volume index.
Also in the chordal preservationgroup, there was better long-term systolic function and LV performance both at rest and during exercise.

Modified Simpson’s Method
EDV – ESV
LVEF = --------------- X 100
EDV

Colour Doppler Indicators of Mitral
Regurgitation Severity
Mild Moderate Severe
Colour Doppler
Jet area (cm2) <4 >10
Ratio of jet area to
left atrial area (%)
<20 >40
Vena contracta
width (cm)
<0.3 >0.7
PISA radius (cm) a <0.4 >1.0

Indicators of Mitral Regurgitation
Severity
Mild Moderate Severe
Multimodality
Regurgitant
volume (mL/beat)
<30 30-59 >60
Regurgitant
fraction (%)
<30 30-49 >50
Effective
regurgitant orifice
area (cm2)
<0.20 0.20-0.39 >0.40

PML Preservation-Lillehei[Preservation of the posterior mitral valve leaflet
and effect on follow-up results after additional
mitral valve implantation]..
Abstract
As early as 1964, Lillehei et al. published the technique of preservation of the
posterior mitral leaflet (PML) and chordae tendineae in combination with mitral
prosthesis implantation (MPI). In a limited randomized number of 95 patients with
MPI the influence of preservation of PML on hemodynamics and physical capacity at
least 46 months after surgery without (group A) and with preservation of PML (group
B) was investigated. Statistically significant differences in favor of group B were
found for cardiac index, pulmonary artery pressure after stress,
end-diastolic volume index (EDVI), physical capacity and
survival rate after a complication-free course. Basing on these results
at rest and after exertion (30 W), patients with preservation of PML and MPI are long-
term in a better clinical condition.

DAVID’S TECHNIQUE


DAVID’S TECHNIQUE(reduction in tumor blush

2
Feikes et all
Figure 42-5. Conventional mitral valve replacement with
complete excision of the leaflets and the entire subvalvular
apparatus, as used in the past and in cases of advanced
rheumatic disease. The mitral prosthesis is implanted using
a series of horizontal mattress sutures

Feikes et all

2
Khonsari I technique
Figure 42-5. Conventional mitral valve replacement with
complete excision of the leaflets and the entire subvalvular
apparatus, as used in the past and in cases of advanced
rheumatic disease. The mitral prosthesis is implanted using
a series of horizontal mattress sutures


2
Khonsari I & II technique

ROSE & OZ Technique

ROSE & OZ Technique


2
MIKI ET ALL
Figure 42-5. Conventional mitral valve replacement with
complete excision of the leaflets and the entire subvalvular
apparatus, as used in the past and in cases of advanced
rheumatic disease. The mitral prosthesis is implanted using
a series of horizontal mattress sutures

2
Nara technique
Figure 42-5. Conventional mitral valve replacement with
complete excision of the leaflets and the entire subvalvular
apparatus, as used in the past and in cases of advanced
rheumatic disease. The mitral prosthesis is implanted using
a series of horizontal mattress sutures

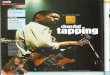
CROSSED PAPILLOPLEXY


(A) Schematic of mitral valve.
© 2003 Elsevier B.V.
detach the strip of anterior leaflet only
from the anterolateral commissure and
preserve the posteromedial commissure
attachment.
This technique does not require any
sutures other than those used for valve
attachment and causes no annular
deformation or leaflet restriction.
Furthermore, because the strip is left
attached at the annulus of posteromedial
commissure, it is easy to begin
attachment of the strip to the annulus.
This modification is simple and effective
in preventing complications associated
with the technique of chordal-sparing
mitral valve replacement.

Intraoperative photograph.
Sasaki H , Ihashi K Eur J Cardiothorac Surg 2003;24:650-
652
© 2003 Elsevier B.V.

Oblique transposition of AML

SINTEK et all




Journals
Postoperative assessment of chordal preservation and changes
in cardiac geometry following mitral valve replacement




Which one to choose

Safeguards-Ideal methodThe factors to be considered are the
simplicity and reproducibility of the technique
prevention of post-operative LVOTO due to systolic
anterior motion of the remaining AML
risk of interference with the prosthetic valve function.
The technique used should allow for implantation of
an adequate size prosthesis to prevent post-operative
patient-prosthesis mismatch..

TAKE HOME MESSAGEComplete chordal preservation advantages.
It preserves LV geometry and function,
reduces the operative mortality,
improves early and long-term survival
reduces the risk of ventricular rupture.
With appropriate surgical technique even large size prosthetic valves can be
implanted and the risk of prosthetic valve dysfunction and LV outflow tract
obstruction can be eliminated.
There is emerging evidence which suggests that RV function may improve
significantly after LV chordal preservation.