Embed Size (px)
Citation preview

Mesenteric Ischaemia
Presented by Lyndon Woytuck, BSc

What is the most common cause of mesenteric ischaemia?A. Acute thrombosisB. Acute embolismC. Chronic atherosclerotic occlusionD. Venous thrombosis

Causes of Impaired Mesenteric Circulation• Atherosclerosis• Arterial embolus• Arterial dissection• Thrombosis• Vasculitis• Mesenteric venous thrombosis• Poor cardiac output leading to low mesenteric flow• Inflammatory or other conditions affecting mesenteric
vessels (e.g., pancreatitis, perforated ulcer, tumor)

The pathophysiology of acute mesenteric ischemia includes all except:
A. Initial Vasospasm.B. Intestinal bacterial translocation.C. Systemic inflammatory response.D. Vasoconstriction.E. Intestinal infarction.

Acute Presentation• “pain out of proportion to examination”• Epigastric bruit• Tenderness on palpation• Hematochezia• Changes in mental status• History of multiple vascular/thromboembolic risk
factors

What is different about mesenteric ischaemia compared to other acute ischaemia?A. More common.B. Less lethal.C. More common in females.D. Easier to diagnose.E. All of the above.

Chronic Presentation• Abdominal pain, postprandial pain• “food fear”• Nausea or vomiting (or both)• Early satiety• Diarrhea or constipation (or both)• Weight loss• History of systemic vascular disease

What is the serum marker that suggests severe acute mesenteric ischemia?
A. Albumin.B. Transferrin.C. Lactate.D. CRP.E. Transthyretin.

Labs• Metabolic or Lactic Acidosis• Left shift and increased absolute WBC indicate full
thickness bowl involvement• albumin, transthyretin, transferrin, CRP to assess
malnutrition

Investigations• Duplex ultrasonography (S/S 85-90%)• CTA (S/S 95-100%) 1-3mm thin slices with contrast• MRA (avoids radiation & contrast, but less precise)• Endoscopy for other diagnoses• Catheter angiography can confirm before open
surgery

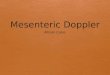
Computed Tomographic Angiography (CTA) in a Patient with Acute Mesenteric Ischemia Caused by an Embolism in the Superior Mesenteric Artery.

Initial Management• Fluid resuscitation with isotonic crystalloids, blood
products if needed• Heparin therapy• Broad spectrum antibiotics• NPO in acute ischaemia

Treatment of Acute Ischaemia• Endovascular• Open surgery• Thrombolysis in combination• Largest study N=70• endovascular success in 87%• in-hospital mortality lower among endovascular
procedures than open surgery (36% vs. 50%)• But patients presenting in profound visceral ischemia
may be assigned open


Treatment of Chronic Ischaemia• Endovascular• Angioplasty alone has poor patency and is associated
with poor long-term symptom relief• Stenting
• Open• improved rates of symptom relief at 5 years and of
primary patency (92%) and lower rates of reintervention
• Hybrid• Consider patient’s state of health, life expectancy


Venous Ischaemia• Heparin Long term anticoagulation• Usually enough, but further compromise in 5%
• Transhepatic / percutaneous mechanical thrombectomy• Thrombolysis• Open intraarterial thrombolysis• Laparotomy


Non-occlusive Ischaemia• Address hemodynamic instability• Anticoagulation• Vasodilation• Catheter-directed infusion of vasodilatory and
antispasmodic agents (papaverine hydrochloride)


Follow-up• Smoking-cessation• blood-pressure control• statin therapy• Lifelong aspirin• endovascular repair – clopidogrel 1-3months• Anticoagulation - AF, venous thrombosis, or
thrombophilia• TPN or nutritional interventions• Duplex US at 6m, 1y, then annually