Embed Size (px)
Citation preview

MENINGITIS
By: Fat in Saud

Outline
Definition Symptoms Signs in newborns Causes Bacterial meningitis Risk factors Complications Lab Diagnosis Treatments and drugs Prevention Immunizations

Definition
Meningitis is an inflammation of the membranes (meninges) surrounding brain and spinal cord.

Symptoms
The signs and symptoms that may occur in anyone older than age of 2 include: Sudden high fever Severe headache that isn't easily confused with other
types of headache Stiff neck Vomiting or nausea with headache Confusion or difficulty concentrating Seizures Sleepiness or difficulty waking up Sensitivity to light Lack of interest in drinking and eating Skin rash in some cases, such as in meningococcal meningitis

Signs in newborns
Newborns and infants may not have the classic signs and symptoms of headache and stiff neck. Instead, signs of meningitis in this age group may include: High fever Constant crying Excessive sleepiness or irritability Inactivity or sluggishness Poor feeding A bulge in the soft spot on top of a baby's head
(fontanel) Stiffness in a baby's body and neck

Causes
Bacterial meningitis Viral meningitis Chronic meningitis Fungal meningitis Other meningitis causes
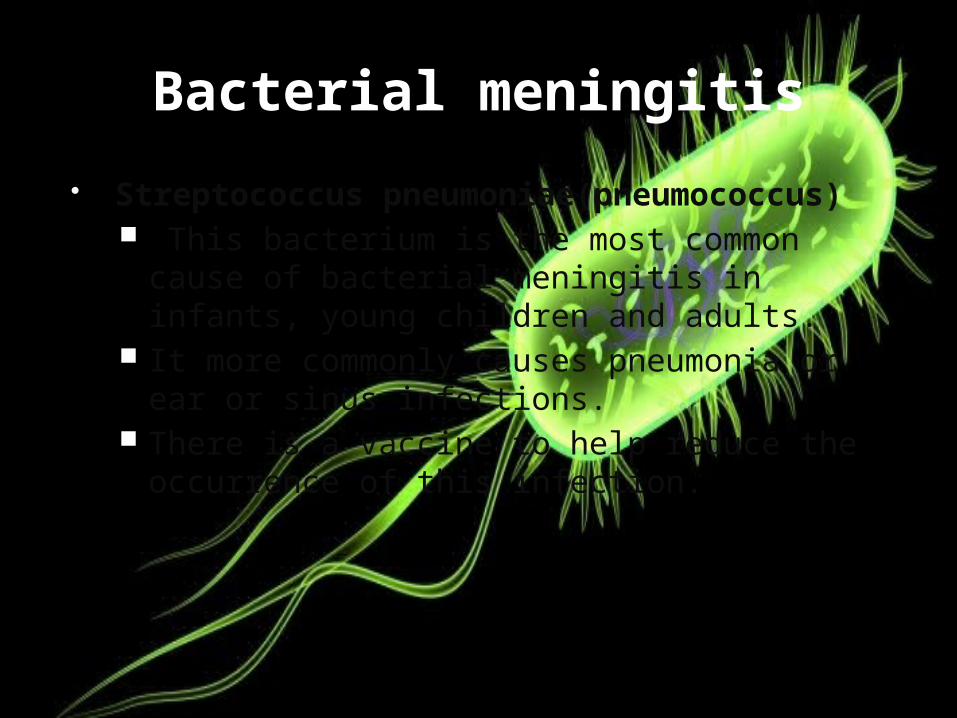
Bacterial meningitis
Streptococcus pneumoniae(pneumococcus) This bacterium is the most common cause of
bacterial meningitis in infants, young children and adults.
It more commonly causes pneumonia or ear or sinus infections.
There is a vaccine to help reduce the occurrence of this infection.

Neisseria meningitidis (meningococcus). This bacterium is another leading cause of bacterial
meningitis. Meningococcal meningitis commonly occurs when
bacteria from an upper respiratory infection enter bloodstream.
This infection is highly contagious. There is a vaccine to help reduce the occurrence of
this infection.

Haemophilus influenzae (haemophilus). Haemophilus influenzae type b (Hib) bacterium used
to be the leading cause of bacterial meningitis in children.
New Hib vaccines — available as part of the routine childhood immunization

Listeria monocytogenes (listeria). These bacteria can be found in soft cheeses, hot
dogs and luncheon meats. Fortunately, most healthy people exposed to listeria
don't become ill, although pregnant women, newborns, older adults and people with weakened immune systems tend to be more susceptible.
Listeria can cross the placental barrier, and infections in late pregnancy may cause a baby to be stillborn or die shortly after birth.
People with weakened immune systems, due to disease or medication effect, are most vulnerable.

Risk factors
Skipping vaccinations. If child hasn't completed the recommended childhood or adult vaccination schedule, the risk of meningitis is higher.
Age. Most cases of viral meningitis occur in children younger than age 5. Bacterial meningitis commonly affects people under 20, especially those living in community settings.
Living in a community setting. College students living in dormitories, personnel on military bases, and children in boarding schools and child care facilities are at increased risk of meningococcal meningitis. This increased risk likely occurs because the bacterium is spread by the respiratory route and tends to spread quickly wherever large groups congregate.

Continue
Pregnancy. If pregnant, at increased risk of contracting listeriosis — an infection caused by listeria bacteria, which also may cause meningitis. If have listeriosis, unborn baby is at risk, too.
Compromised immune system. Factors that may compromise immune system — including AIDS, alcoholism, diabetes and use of immunosuppressant drugs — also make more susceptible to meningitis. Removal of spleen, an important part of immune system, also may increase risk.

Complications
Hearing loss Memory difficulty Learning disabilities Brain damage Gait problems Seizures Kidney failure Shock Death

LAB DIAGNOSIS
CSF EXAMINATION HISTOPATHOLOGY LATEX AGGLUTNATION POLYMERASE CHAIN
REACTION VIRAL CULTURE RAPID DIAGNOSTIC
TESTS (RDT) SEROLOGIC STUDIES OTHER LAB STUDIES

CYTOLOGIC STUDIES OF CSF
Laboratory examination of the CSF is usually the first step to confirm the presence of meningitis.
Cytological examination should precede centrifugation and heating of CSF.

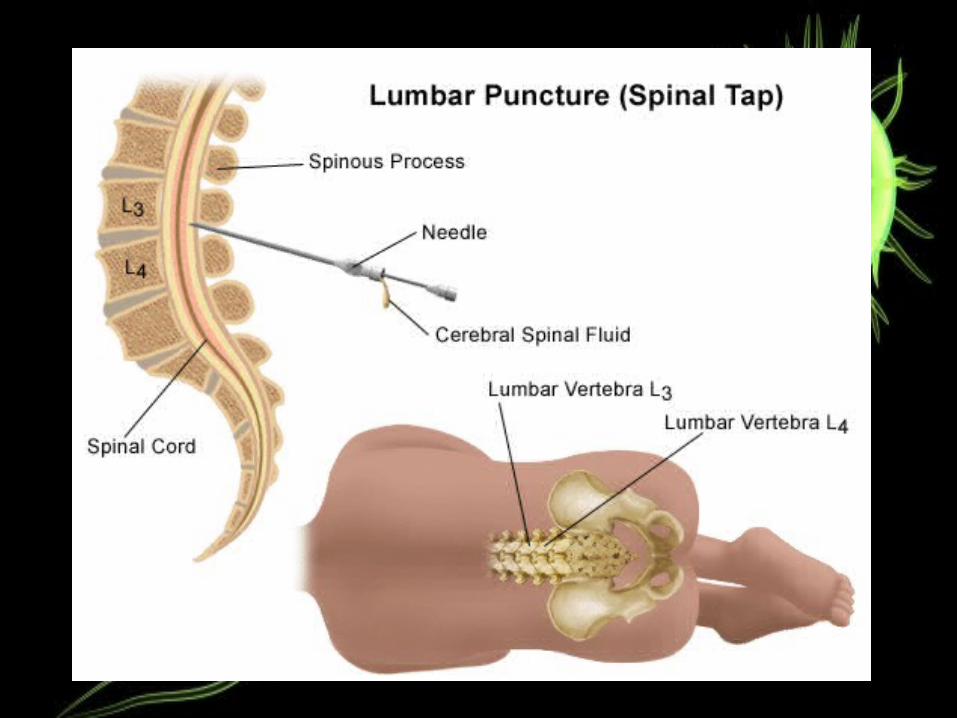
Spinal tap (lumbar puncture). The definitive diagnosis of meningitis requires an analysis of cerebrospinal fluid (CSF), which is collected during a procedure known as a spinal tap. In people with meningitis, the CSF fluid often shows a low sugar (glucose) level along with an increased white blood cell count and increased protein.

CSF EXAMINATION
The typical profile:CSF opening pressure: 50–180 mmH2O
Glucose: 40–85 mg/dL.Protein (total): 15–45 mg/dL.
Leukocytes (WBC): 0–5/µL (adults / children); up to 30/µL (newborns).
Culture: sterile.Gross appearance: Normal CSF is clear and
colorless.Differential: 60–70% lymphocytes; up to 30%
monocytes and macrophages; other cells 2% or less.
VIRAL MENINGITIS
Glucose (mg/dL):Normal (> 40 mg/dL.) Protein (mg/dL) <100 mg/dL (moderate
increase) WBCs (cells/µL) < 100 cells/µL. Cell differential: Early: neutrophils. Late:
lymphocytes. Culture: Negative Opening Pressure Usually normal

BACTERIAL MENINGITIS
Glucose (mg/dL):Normal to marked decrease. <40 mg/dL.
Protein (mg/dL): (Marked increase) > 250 mg/dL.
WBCs (cells/µL): >500 (usually > 1000). Early: May be < 100.
Cell differential: Predominance of Neutrophils (PMNs)
Culture: Positive Opening Pressure: Elevated
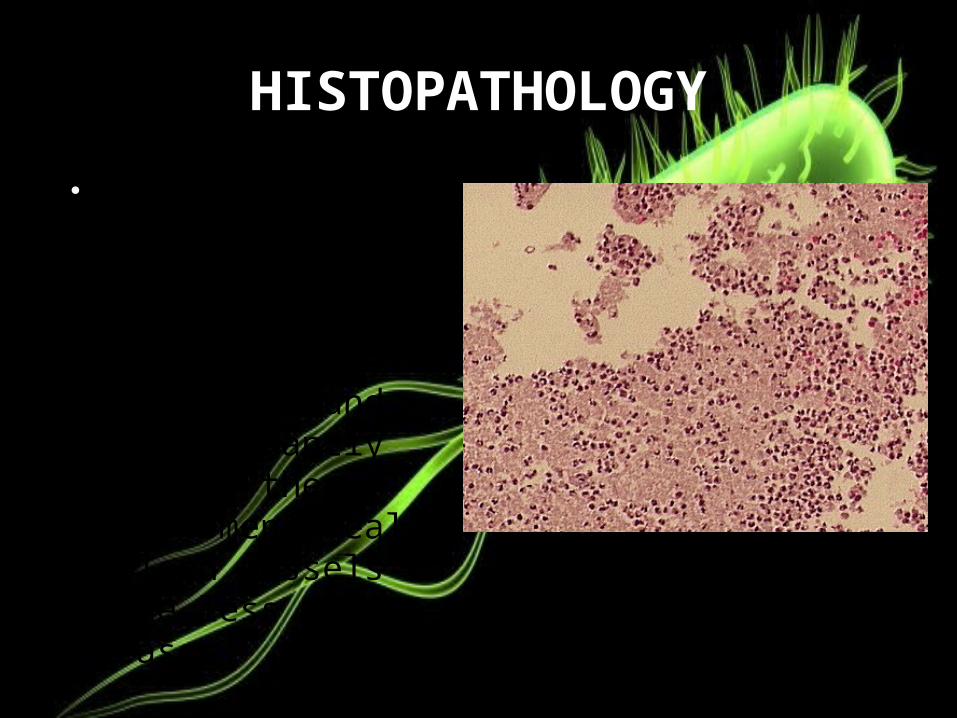
HISTOPATHOLOGY
Neutrophils fill the subarachnoid space in severely affected areas and are found predominantly around the leptomeningeal blood vessels in the less severe cases.
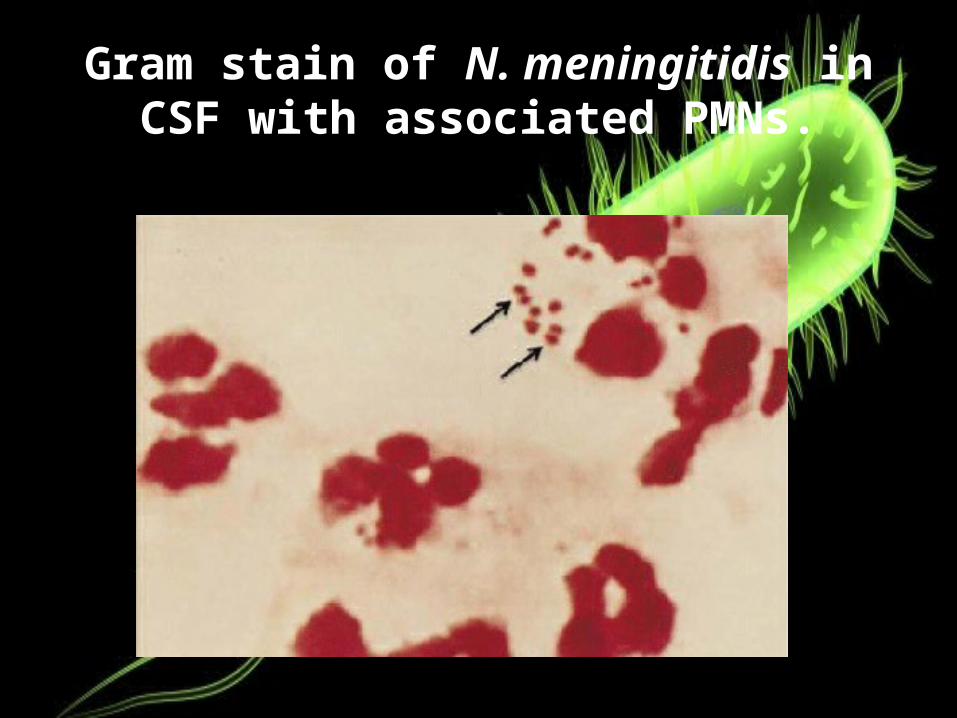
Gram stain of N. meningitidis in CSF with associated PMNs.

STREPTOCOCCUS PNEUMONIAE

LATEX AGGLUTINATION Positive reaction: agglutination (or visible
clumping) of the latex particles and slight clearing of the suspension occurs within 2-10 minutes .
Negative reaction: the suspension remains homogenous and slightly milky in appearance.

POLYMERASE CHAIN REACTION
Amplification of virus specific DNA or RNA from CSF using PCR amplification has become the single most effective method for diagnosing CSF viral infections.
It is a highly sensitive and specific test since only trace amounts of the infecting agent's DNA is required.
It may identify bacteria in bacterial meningitis and may assist in distinguishing the various causes of viral meningitis.
VIRAL CULTURE
The sensitivity of CSF cultures for the diagnosis of viral meningitis is poor in comparison to the detection of bacterial meningitis.
Viruses may also be isolated from throat swabs, blood and urine.
Enterovirus and adenoviruses maybe found in the feces.

Proper streaking and growth of N. meningitidis on a Blood Agar Plate

Proper streaking and growth of S. pneumoniae on a Blood Agar Plate
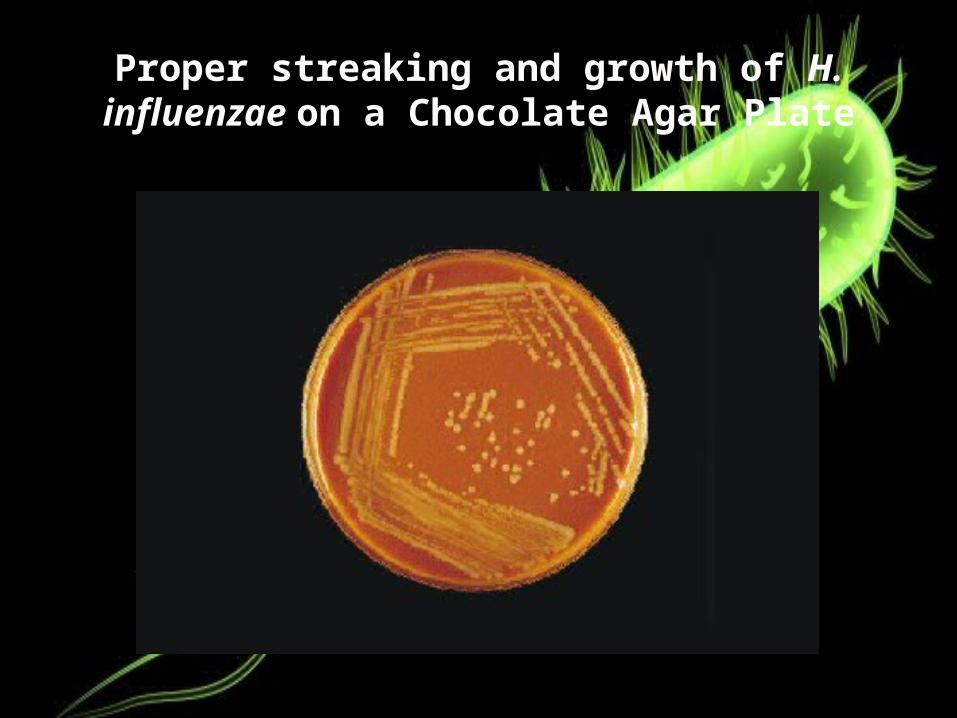
Proper streaking and growth of H. influenzae on a Chocolate Agar Plate

SEROLOGIC STUDIES
Crucial diagnostic tool Serum antibody detection is less useful for viruses with
high prevalence rates in the general population. For viruses with low prevalence rates , diagnosis of
acute viral infection can be made by documenting Seroconversion between acute phase and
convalescent sera. The documentation of synthesis of virus specific
antibodies in CSF is more useful than serum serology alone.

RAPID DIAGNOSTIC TESTS (RDT)
RDTs have been developed for direct testing of CSF specimens without prior heat or centrifugation.
The test is based on the principle of vertical flow immunochromatography.
Gold particles and nitrocellulose membranes are coated with monoclonal antibodies to capture soluble serogroup-specific polysaccharide antigens in the CSF.

READING THE RDT RESULTS
Appearance of red lines on the dipsticks will indicate whether one of the four meningococcal serogroups has been detected in the CSF.
The upper line on the dipstick is the positive control and should always be present.
If the CSF is positive for one of the serogroups, a lower red line will also be present. The position of that red line indicates the specific serogroup based on the RDT that was tested.
A negative result consists of a single upper pink control line only.


OTHER LABORATORY STUDIES
CBC (complete blood count) & DLC (differential leucocyte count)
Liver and Renal function tests ESR (erythrocyte sedimentation rate) C- Reactive protein Electrolytes etc MRI and CT are not necessary in patients with
uncomplicated meningitis. They may be performed in patients with altered
consciousness, seizures etc

Imaging. X-rays and computerized tomography (CT) scans of the head, chest or sinuses may reveal swelling or inflammation. These tests can also help doctor look for infection in other areas of the body that may be associated with meningitis.

Acute bacterial meningitis. This axial nonenhanced CT scan shows mild
ventriculomegaly and sulcal effacement.

Treatments and drugs
Bacterial meningitis Acute bacterial meningitis requires prompt treatment with
intravenous antibiotics and, more recently, cortisone medications, to ensure recovery and reduce the risk of complications, such as brain swelling and seizures. The antibiotic or combination of antibiotics that your doctor may choose depends on the type of bacteria causing the infection. Your doctor may recommend a broad-spectrum antibiotic until he or she can determine the exact cause of the meningitis.
Infected sinuses or mastoids — the bones behind the outer ear that connect to the middle ear — may need to be drained.

Prevention
Wash hands. Practice good hygiene. Stay healthy Cover your mouth. pregnant, take care with food.

Immunizations
Haemophilus influenzae type b (Hib) vaccine. Pneumococcal conjugate vaccine (PCV7). Haemophilus influenzae type b and Neisseria
meningitidis serogroups C and Y vaccine (Hib-MenCY).
Pneumococcal polysaccharide vaccine (PPSV).
Meningococcal conjugate vaccine (MCV4).