Embed Size (px)
DESCRIPTION
MelasmaPostinflammatory hyperpigmentationDrug induced hyperpigmentationSolar lentigosCafé au lait maculesNevus of Ota
Citation preview

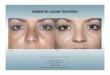
MELASMA Epidemiology, Classification,
Pathophysiology The International School of Vitiligo & Pigmentary Disorders.
Barcelona, Spain - 2-5 November 2011
Prof. Lotti T, Betti S, M.D.
Barcelona, November 2011

Melasma Postinflammatory hyperpigmentation Drug induced hyperpigmentation Solar lentigos Café au lait macules Nevus of Ota

MELASMAMelasma consists of an excessive
production of melanin (hypermelanosis)
which causes the appearance of brownspots on sun-exposed areas
of the face.

Skin color
Melanins:Eumelanin
Pheomelanin
Hemoglobin Stratum corneum Reflectivity of the epidermis
The polymerization is stopped prematurely, and the mixture thus obtained is bound to proteins. Typical of blond e rutile subjects
Extensive polymerization of the monomers of tyrosine oxidized. Tipical in subjects well- pigmented (blacks, brown)
It is yellow and very thick in asian people

MelanocytesDendridic shape with hemispherical body from which depart decreasing calibrum extensions forking several times.
The medium density is around 1000 / mm2 of skin surface.

The numerical density of melanocytes is indipendent of skin color, that depends on the activity of melanocytes and on the persistence of melanin in keratinocytes.
•In people with white skin and those of yellow skin, melanin is limited to the basal layer.
•In people with black skin melanin is found up to thesurface layer.

Melanin
Tyrosin DOPA
Tyrosinase
DQ
Phenolic oxidant Ez containing Copper
cycli
zatio
n
Indole
Eumelanine
Poli
meri
z.ox
Cysteine or
glutathione
residues
Cisteinildope
Feomelanine
oxi
dati
on

Melanin
The mature melanosoms are also known as melanine granules, they migrate into dendrites and are transferred to keratinocytes for posting portions of dendrites or phagocytosis
Tyrosine Melanin
Tyrosinase

Mature melanin granules
Phagocytosed by keratinocytes
Stay in in lysosomes where vengono they are digested(in subjects with little pigmented skin)
Break free in the cytoplasm and persist for some time (in black skin subjects)


Changes in Melanogenesis
Melasma

MELASMA

EPIDEMIOLOGY
Real incidence unknown90% women, 10% menAll races Hispanic, Asian, Indo-Chinese, Africans

ETIOLOGY
Genetic influences Exposure to UV
radiation Pregnancy Oral
contraceptives Cosmetic Phototoxic drugs

GENETIC PREDISPOSITIONthe condition is most widespread among women with skin types III or IV, such as Asian-Americans and people of Mediterranean descent.
EXPOSURE TO UV RADIATIONit is the most important exacerbating factor. Ultraviolet light normally increases melanogenic activity in melanocytes with resulting hyperpigmentation. Once melasma has developed, exposure to sunlight will perpetuate the condition and counteract any other treatment. Use SPF or higher sunscreens that block both UVA and UVB radiation.
PREGNANCY AND CONTRACEPTIVESsome researchers believe it is induced when extrogen stimulates the pigment-producing cells in the skin to secrete more pigment.Melasma it is also known as chloasma or “mask of pregnancy” and it is a very common condition usually seen in women of childbearing age.

LOCALIZATION

CLINICAL PATTNERS: melasma of the face
CentrofacialMalarMandibularCleft lip and chin (chin and upper lip)
centrofacial type: 63% of cases (simmetrycal involvement of the cheeks and nose). malar type: 21% of cases (simmetrycal involvementof the cheeks and nose).
jaw type : 8% of cases (involvement of the maxillary branch of the mast).Lip-chin type: 8% of cases (involvementof the upper lip and chin).

TYPE OF PIGMENTATION
GuttataConfetti likeLinearLarge circular patches

Based on Wood’s lamp examination of the skin, melasma can be classified into four main clinical types and patterns, with correlation in histology , in accordance with the depth of melanin pigment.

EPIDERMAL: light brown, with an enhancement of pigmentation under Wood’s lamp; histologically, it is characterized by a melanin increase in tha basal, suprabasal and stratum corneum layers.
DERMAL: ashen or bluish-grey; no enhancement of pigmentation under Wood’s light; histologically, there is a preponderance of melanophages in the superficial and deep dermis.
MIXED: dark brown; enhancement of pigmentationunder Wood’s lamp in some areas and not in others.
INDETERMINATE: inapparent under Wood’s lamp.
The best terapeutical results are normally achieved in epidermal melasma.

MELASMA SEVERITY
It is scored using the Melasma Area and Severity Index (MASI). In this system, the face is divided into four areas- forehead, right malar, left malar and chin- which correspond, respectively, to 30%, 30%, 30% and 10% of the total facial area.
Torello Lotti: Pigmentary Disorders
Dermatologic Clinics Vol.25, Number 3, July 2007
theclinics.com / Elsevier Saunders

The Melasma in each of there areas is graded according to three variables:
1- Percentage of total area involved
on a scale from o (no involvement) to 6 (90-100% full involvement)
2- Darkness scoring
from 0 to 4 is assessed to a color chart
3- The scale of each patient is graded according to the comparison between the darkness of the melasma and the colour of the chart:
scale 0: no melasma
scale 1: light brown
scale 2: brown
scale 3: dark brown
scale 4: black

The MASI is then calculated using the following equation:
MASI= 0.3(DF+HF)AF+0.3(DMR+HMR)AMR+0.3
(DML+HML)AML+0.1(DC+HC)AC
D= darkness
H= homogeneity
A= area
F= forehead
MR= right malar
ML= left malar
C= chin
0.3,0.3,0.3,0.1= are the respective percentage of total
facial area.

The MASI is measured before treatment as a baseline and after
each session of treatment

Endotelin-1:peptide produced by endothelial cells and by keratinocytes
melanocytes
Recent data also showed that melasma lesions have more vascularizationas compared to the perilesional normal skin. Increased expression of vascular endothelial growth factor (VEGF) in keratinocytes was suggested as the major angiogenic factor for altered vessels in melasma
PATHOGENESIS
UV irradiation is known to increase the synthesis of alpha-MSH and ACTH derived from POMC in keratinocytes. These peptides lead to proliferation of melanocytes as well as increase in melanin synthesis via stimulation of tyrosinase activity and TRP-1.

This is confirmed by:The vascular characteristics of melasma.Kim EH, Kim YC, Lee ES, Kang HY.J Dermatol Sci 2007.
OBJECTIVES: We investigated the vascular characteristics in melasma lesions. The expression of vascular endothelial growth factor (VEGF), a major angiogenic factor of the skin, was also investigated in melasma.METHODS: Erythema intensity was quantified by the increase of the a* parameter using a colorimeter. Skin samples were obtained from lesional and non-lesional facial skin of 50 Korean women with melasma. Immunohistochemistry was performed to determine the expression of factor VIIIa-related antigen and VEGF in melasma.

RESULTS
The values of a* was significantly higher in the melasma lesion than that of perilesional normal skin. Computer-assisted image analyses of factor VIIIa-related antigen-stained sections revealed a significant increase of both the number and the size of dermal blood vessels in the lesional skin. There was significant relationship between the number of vessels and pigmentation in
CONCLUSIONS
These data suggest that increased vascularity is one of the major findings in melasma. VEGF may be a major angiogenic factor for altered vessels in melasma.
Torello Lotti: Pigmentary Disorders
Dermatologic Clinics Vol.25, Number 3, July 2007
theclinics.com / Elsevier Saunders

Torello LottiFull Professor of Dermatology
Vice Chancellor, UniMarconi.it , Roma
Thank you for your attention