Embed Size (px)
DESCRIPTION
Clinically oriented presentation 2014
Citation preview

Megaloblastic Anemias
BY; DOCTOR IMRAN SHAHZAD ANJUM,MD
LATIN AMERICAN SCHOOL OF MEDICINE HAVANA CUBA

Concept
An anemia in which there is a predominant number of megaloblasstic erthyroblasts, and relatively few normoblasts, among the hyperplastic erythroid cells in bone marrow (as in pernicious anemia).

Causes of megaloblastic anemia

Cobalamin (vitamin B12)
In nature mainly in 2-deoxyadenosyl (ado) form that is cofactor for enzyme methylmalonyl coenzyme A mutase and other is methylcobalamin in human plasma and in cell cytoplasm that is a cofactor for methionine synthase.
It is solely synthesized by microorganisms and the only source for humans is food of animal origin like meat, fish and dairy products.
Adult daily losses (mainly in urine and feces) are 1-3 ug and as body doesnot have the ability to degrade body store, so daily requirements are also 1-3 ug.
Body stores are of the order of 2-3 mg, sufficient for 3-4 years if supplies are completely cut off.
Because of appreciable amount undergoing enterohepatic circulation, cobalimin deficiency develop more rapidly in individuals who malabsorb B12 then it does in vegans, in whom reabsorption of biliary cobalamin is intact.


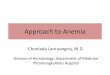
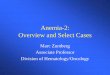
Components and mechanism for cobalamin absorption

Cellular uptake and intracellular reactions involving cobalamin

Sufficiently severe to cause megaloblastic anemia
Malaabsorption of B12, not usually sufficiently severe & prolonged to cause anemia
Causes of cobalamin deficiency

Pernicious anemia of adults
Gastric causes of Cobalamin malabsorption
Severe lack of intrinsic factor due to gastric atophy.
Man and women ratio is 1:1.6 .
Peak age of onset is 60 years and with only 10% patients being < 40 years, blacks indivisuals and latin americans the age of onset generally is lower.
Common in north europens but occur in all countries and ethnic groups.
The disease occur more commenly than by chance in close relatives and in persons with other orgenic specific autoimmune diseases, e.g. Thyroid disease, vitiligo, hypoparathyrodism and addison’s disease.
It also associated with hypogammaglobulinemia, with premature graying or blue eyes and person of blood group A.
The serum gastrin level is raised and serum pepsinogen I level are low.

This usually show atrophy of all layers of the body and fundus with loss of glandular elements, an absence of parietal and chief cells and replacement of mucous cells, a mixed inflammatory cell infiltrate and prehaps intestinal metaplasia. The infiltrate of plasma cells and lymphocyetes contains an excess of CD4 cells.
Gastric biopsy; histological features of stomach in pernicious anemia compared to normal

Juvenile pernicious anemia
This occurs in old children and resembles PA of adults.
Gastric atrophy, achlorhydria and serum IF antibofies are all present, although parietal cell antibodies are usually absent,
About of patients show an associated endocrinopathy such as autoimmune thyroiditis, addison’s disease, or hypoparathyroidism; in some, mucocutaneous candidiasis occurs.

Folate
Folic acid is parent compound of large family of natural folate compounds.
Its highest concentration is found in liver, yeast, spinach, other greens and nuts.
Folate easily destroyed by heating, particularly in large volumes of water.
Total folate in adult is ~10mg with liver containing the largest store.
Daily adult requirements are ~10ug and so stores are sufficient for 3-4 months in normal adult and severe folate deficiency may develop rapidly.


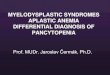
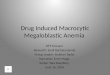
Folates absorption in small intestine & transport
Folate polyglutamate
s
MonoglutamatesLumen-mucosa
5-methyl THFIntestinal-mucosa
Albumin bound 1/3
unbound 2/3 in plasma
Cellular receptors; PCFT/HCPI,
Clathrin-coated pits
Membrane folate
Transporter
Cell cytoplasmPlasma,CSF, milk
and bile have folate
In malabsorption syndrome; due to loss of folate 60-90 ug in bile each day, with folate of sloughed intestinal cells, accelerate speed with which
folate deficiency develop in malabsorption conditions.

Causes of folate deficiency

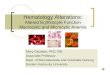
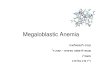
Biochemical basis of megaloblastic anemia
The folate is needed as coenzyme 5,10-methylene THF polyglutame for conversion of dUMP to dTMP.
In deficiencies of folate or cobalamin, there is failure to convert of dUMP to dTMP; precursor of dTTP.
The availablity of 5,10-MTHF is reduced in either cobalamin or folate deficiency.
in cobalamin deficiency due to failure of formation of THF, the substrate on which folate polyglutame are build, MTHF accumulates in plasma and intracsellular concentration fall; termed as THF starvation or methylfolate trap.

The role of folates in DNA synthesis and formation of SAM which is involved in methylation reaction

Bridge to pharmacology
A substance inhibiting cell growth by competing with, or substituting for, a natural substrate in an enzymatic process is called antimetabolities.
Antimetabolite drugs that interfere with either DNA replication or folate metabolism may interfere in replicationa and cause megaloblastic appearance.
The drugs Methotrexate, hydroxyurea, cytosine arabinoside, Pyrimethamine and sulfonamides (mainly in bacteria Trimethoprim) inhibits DHF reductase and so prevent formation of active THF coenzyme from DHF.

Pathogensis
Megaloblastic anemia are group of disorders characterized by distinct morphological pattern in hematpoitic stem cells. A common feature is a defect in DNA synthesis with lesser alterations in RNA and protien synthesis, leading to state of unbalanced cell growth and impaired cell division. Most RBCs are not resting but vainly engaged in attempting to double their DNA,with frequent arrest in S phase and lesser degree of arrest in other phases of cycle. An increased percentage of RBCs have increased DNA content is expressed morphologically as larger than normal “immature nucli” with finely particulate chromatin whereas the relatively unimpaired RNA and protein synthesis results in larger cells with greater “mature” cytoplasm and cell volume. The microscopic appearance of this nuclear-cytoplasmic asynchrony is morphologically discribed as “megaloblastic”.


Clinical features
Many patients are diagnosed through finding of a raised MCV on rotuine CBC.
The main clinical features in more severe cases are those of anemia.
Anorexia is usually marked and there may be weight loss, diarrhea or constipation.
Glossitis, angular cheilosis and mild fever in more severely anemic patients, Juandice(unconjugated) and reversible skin melanin hyperpigmentation also may occur with deficiency of cobalamin or folates.
Thrombocytopenia sometimes leads to bruising and this may be aggrevated by vitamin C deficiency or alcohol in malnourished patients.
Anemia and low leukocyte count may predispose to infections, particularly of respiratory and urinary tract.
Cobalamin deficiency has also been associated with impaired bactericidal function of phagocytes.



Diagnosis of megaloblastic anemia
Hematological findings
1. Peripheral blood
2. Bone marrow
3. Ineffective hematopoiesis
4. Chromosome abnomalities
Diagnosis of cobalamin and folate deficiencies
1. Serum cobalamin
2. Serum folate
3. Red cell folate
4. Serum methylmalonate and homocysteine

How to classify the patient of anemia?




Automated enzyme-linked immunosorbent assay (ELISA)
Serum cobalamin (normal range; 118-148 pmol/L, MA <74 pmol/L) is cost effective and most convient to rule out B12 deficiency in vast majority of patients suspected of having this problem.
Serum folate (normal range; 11-82 nmol/L; also recent recent diet) concentation rises in severe B12 deficinecy because of block in conversion of MTHF to THF inside cells; raised levels has also been reported in intestinal stagnant loop syndrome due to absorption of bacterially synthesized folate.


Red cells folate assay
Normal range 880-3520 umol/L.
Less effected than serum assay for recent diet and traces of hemolysis.
False normal results may occur if a folate-deficient patient may received blood transfusion or a patient has raised reticulocyte count.

Serum methylmalonate and homocysteine
For early diagnosis of B12 deficiency even the absence of hematological abnormalities or subnormal levels of serum cobalamin can be measured by MMA and homocysteine.
Serum homocysteine may be raised in other conditions like chronic renal disease, alcoholism, smoking, pyridoxine deficiency, hypothyroidism and therapy with steroids, cyclosporine and other drugs.

Ineffective hematopoiesis
Accumulation of unconjugated bilirubin in plasma , raised urine urobilinogen, reduced heptaglobin and positive urine hemosiderin, and a raised lactate dehydrogenase due to death of nucleated RBCs in marrow.
A weakly positive direct antiglobulin test due to complement can lead to false diagnose of autoimmune anemia.

Chromosome abnormalities
Bone marrow cells, transformed lymphocytes, and other proliferating cells in the body show a variety of changes, including random breaks, reduced contraction, spreading of centromere and exaggeration of secondary chromosomal contractions and over-prominent satellites.

Treatment of megaloblastic anemia
For out-door patients; establish which of two deficiencies, folate or B12 is the cause and treat only with appropriate vitamin.
For In-door patients; once blood sample and bone marrow biopsy (only if deemed necessary) has been taken for assays, it may be necessary to treat with both vitamins in large doses.

Indications of therapy
A well-documentated megaloblastic anemia or other hematological abnormalities and neuropathy due to B12 deficiency.
Partial or complete gastroectomy or ileal resection and long-term PPI therapy should be screened and if necessary given B12 therapy.
As anemia of B12 deficiency responds to folic acid in large doses before large doses of folic acid are given, Cobalamin deficiency must be excluded, and if present, corrected and otherwise cobalamin neuropathy may develop despite a response of anemia of cobalamin deficiency to folate therapy.

Indications for treatment
Cobalamin(B12) Replenishment therapy 1000-ug
IM injection of hydroxycobalamin given at 3-7 days intervals
Maintenance therapy; 1000 ug IM every 3 months or 1000-2000 ug VO daily
Allergic reactions are rare and require desensitization or antihistamine or glucocorticoid cover.
Folic acid(B9) Replenishment therapy; 5-15 mg
daily continue usually till 04 months when all folate-deficient red cells will have been eliminated and replaced by new folate replete popultation.
Maintenance therapy; daily use of food fortification with folic acid






Hasta la victoria siempre!

Bibliography
Basic Principles & practice of Hematology 2013 by Hoffman
Harrison´s principles of internal medicine
Robbins Basic Pathology
Guyton & Hall Text of Medical Physiology