Embed Size (px)
Citation preview
Margaret Nicholson
Amanda Chapman
When did the attention of monitoring vitals signs change from an important part of a patients management to a task that ‘just needs to be done’?
When did the culture change and how do we get back there?
Our current struggle with reigniting the vitalness of observations
Retrospective note review in Dec 2011 for ◦ Sepsis pathway work in collaboration with Clinical
Excellence Commission
Incidental finding ◦ Inconsistencies with observations post rapid response or
clinical review call
◦ Was this new information, no the MET team identified lack of observations and papers were published (Hillman, Jacques, Buist)
◦ pts requiring close monitoring should be in ICU/HDU- the long held belief by ward staff
0
5
10
15
20
25
0 1 2 3 4 5 6 7 8 9 10 11 14
% o
f p
ati
en
ts
Number of sets of observations
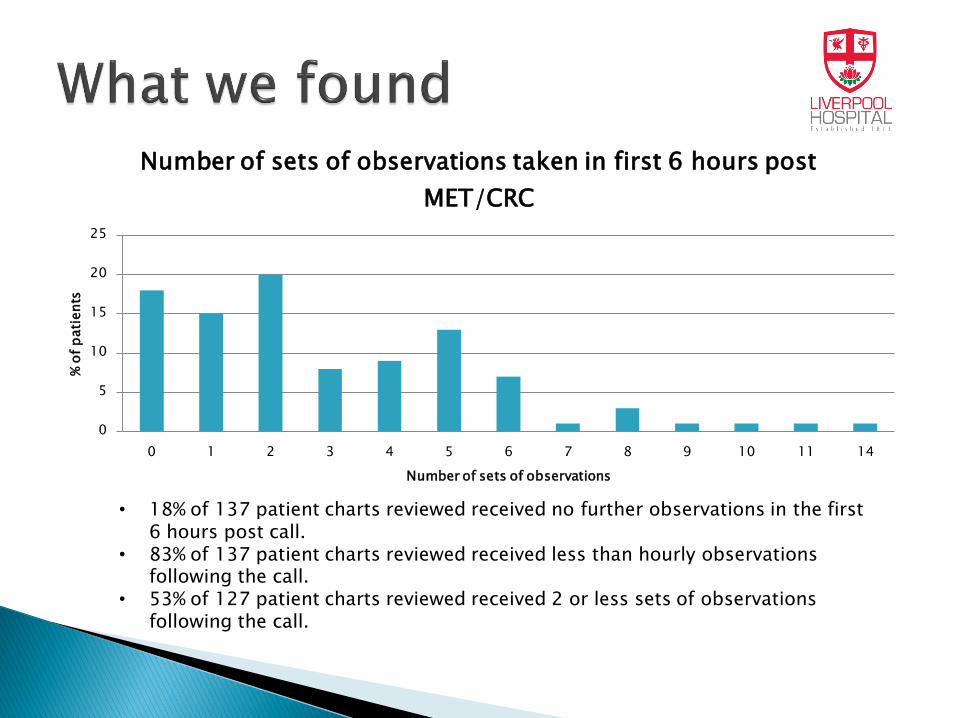
Number of sets of observations taken in first 6 hours post
MET/CRC
• 18% of 137 patient charts reviewed received no further observations in the first 6 hours post call.
• 83% of 137 patient charts reviewed received less than hourly observations following the call.
• 53% of 127 patient charts reviewed received 2 or less sets of observations following the call.
Policies that provided standards in relation to observations ◦ NSW Ministry of Health policy – Recognition and
Management of Patients who are Clinically Deteriorating
Minimum observation frequency
Minimum data set
Increased frequency based on clinical judgement and patient condition
PCA policy
Pathways / guidelines for particular groups of post operative patients
post op observations
Collaborative effort by ◦ Critical care
◦ Policy and Accreditation Manager
◦ Select CNCs
To develop a policy for expectations of observations during and post a rapid response and clinical review call.
Issues ◦ CNC/CNE concerns re: increased workload
◦ Differing options of
What was needed
What was appropriate
◦ Additional observation guidelines added – Where do you stop?
Post operative
Post Emergency Department Transfer
Post transfer from ICU/HDU
◦ Prolonged process of development and approval

Indication
Frequency
Routine
• On transfer or admission to ward.
• Minimum every 4 hours for first 24 hours then if stable every 8 hours e.g., 0600, 1400, 2200.
Clinical Review Call/ Medical Emergency Team Review
• Continuous or 15 minutely observation until stabilised
• Following stabilisation: Half-hourly for 2 hours then hourly for 4 hours then 4 hourly for 24 hours or as ordered by MO for 24 hours.
• For specific MO orders, refer to patient’s SAGO chart - “Variations to Frequency of Observations” or the “Modified Calling Criteria”
• For specific MO orders post MET call, refer to the patient’s “Post MET Management Summary”.
Transfer from ICU
• 2nd hourly for 4 hours then 4th hourly for 8 hours or more frequently if ordered by the MO.
Post Surgery/ Invasive procedure
• On arrival/ transfer
• Hourly for 4 hours then 2nd hourly for 4 hours if stable 4 hourly for 24 hours or as ordered by MO.
Patients who are symptomatic but have not yet breached the CRC calling criteria • Repeat in 30 minutes or as ordered by MO until patient is asymptomatic.
Critical Care Areas / Maternity • As per department/ service based policy.
Night Duty • VISUALLY CHECKED at least hourly overnight (including respiratory effort not
rate). Blood Glucose • prior to administration of insulin or 30 minutes or less before meals and before
supper (approx 2100 hours) 15 minutes after a hypoglycaemic episode and again in one (1) hour if not clinically indicated sooner
• When advised or as clinically indicated Patient Controlled Analgesia
• Hourly for the first six (6) hours then second (2) hourly or more frequently as required until the PCA is ceased.
• 4th hourly Temperature
Minimum Set of vital signs to be recorded every time observations are performed includes: Respiratory Rate; Heart Rate; Blood Pressure; Temperature; Oxygen saturation (SpO2); Neurological - AVPU see Procedure 3.5.1; Pain score. Bowel activity is to be recorded minimum of once per shift. On admission to the hospital/ ward the weight, height and a urinalysis is to be recorded and then weight weekly unless otherwise ordered.
September 2013
Placed on intranet
Email to managers once the policy was available by the Policy and accreditation manager.
No release plan developed
No education plan developed
Change to practice required for compliance
Oct 2013
Audit to show compliance with new policy
CERs co-ordinator attended ◦ MET, CRC, post ED, minimum data set
After hours CNCs ◦ Post ICU
Small sample
0 50 100
Obs 4th hourly for …
Obs 1hrly for 4hrs
Obs 1/2hrly for …
Obs 15min during …
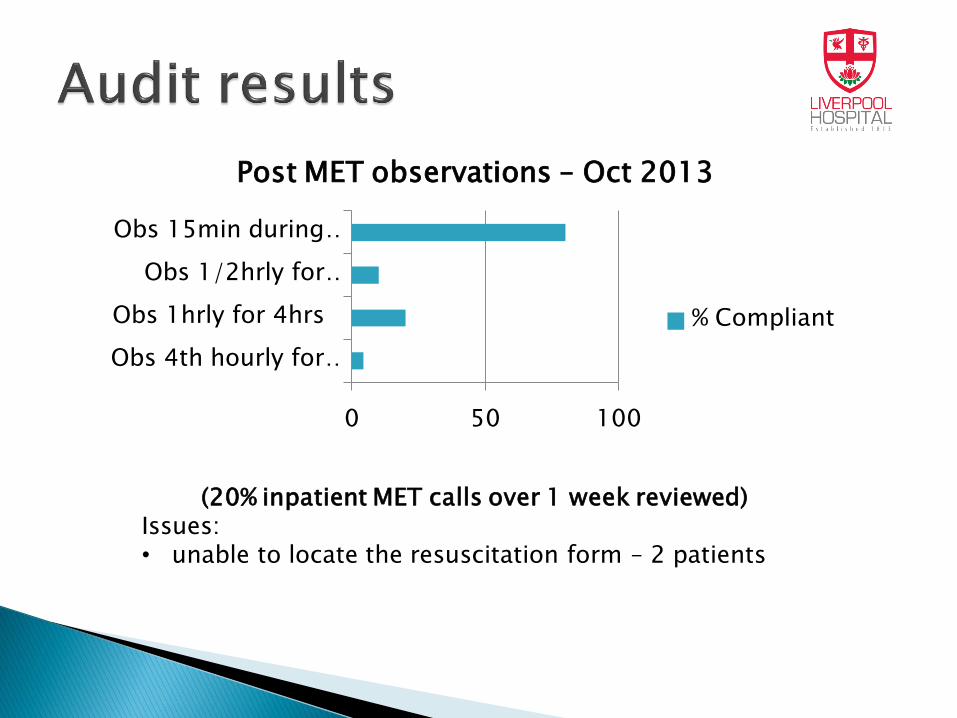
Post MET observations – Oct 2013
% Compliant
(20% inpatient MET calls over 1 week reviewed) Issues: • unable to locate the resuscitation form – 2 patients
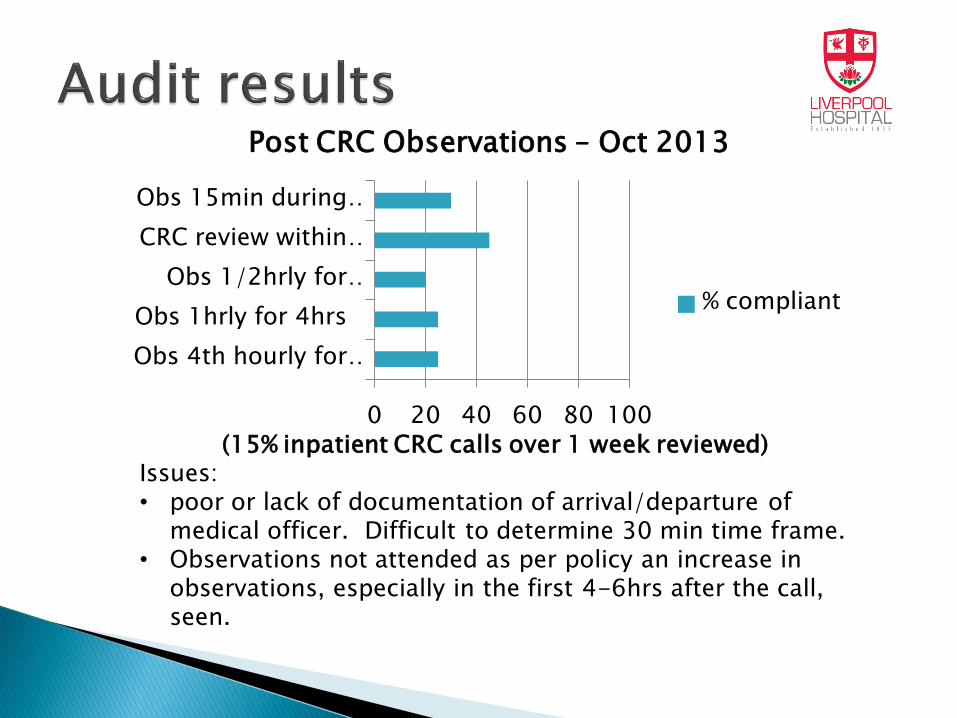
(15% inpatient CRC calls over 1 week reviewed) Issues: • poor or lack of documentation of arrival/departure of
medical officer. Difficult to determine 30 min time frame. • Observations not attended as per policy an increase in
observations, especially in the first 4-6hrs after the call, seen.
0 20 40 60 80 100
Obs 4th hourly for …
Obs 1hrly for 4hrs
Obs 1/2hrly for …
CRC review within …
Obs 15min during …
Post CRC Observations – Oct 2013
% compliant
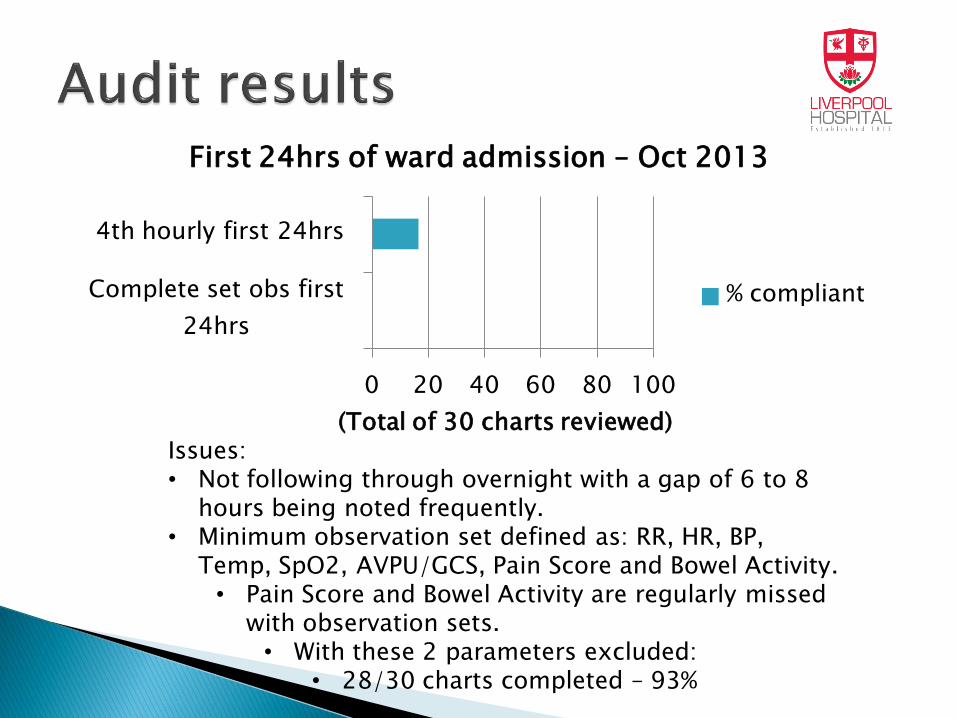
(Total of 30 charts reviewed) Issues: • Not following through overnight with a gap of 6 to 8
hours being noted frequently. • Minimum observation set defined as: RR, HR, BP,
Temp, SpO2, AVPU/GCS, Pain Score and Bowel Activity. • Pain Score and Bowel Activity are regularly missed
with observation sets. • With these 2 parameters excluded:
• 28/30 charts completed – 93%
0 20 40 60 80 100
Complete set obs first
24hrs
4th hourly first 24hrs
First 24hrs of ward admission – Oct 2013
% compliant
0 20 40 60 80 100
2/24 for 4hrs
4/24 for 48hrs
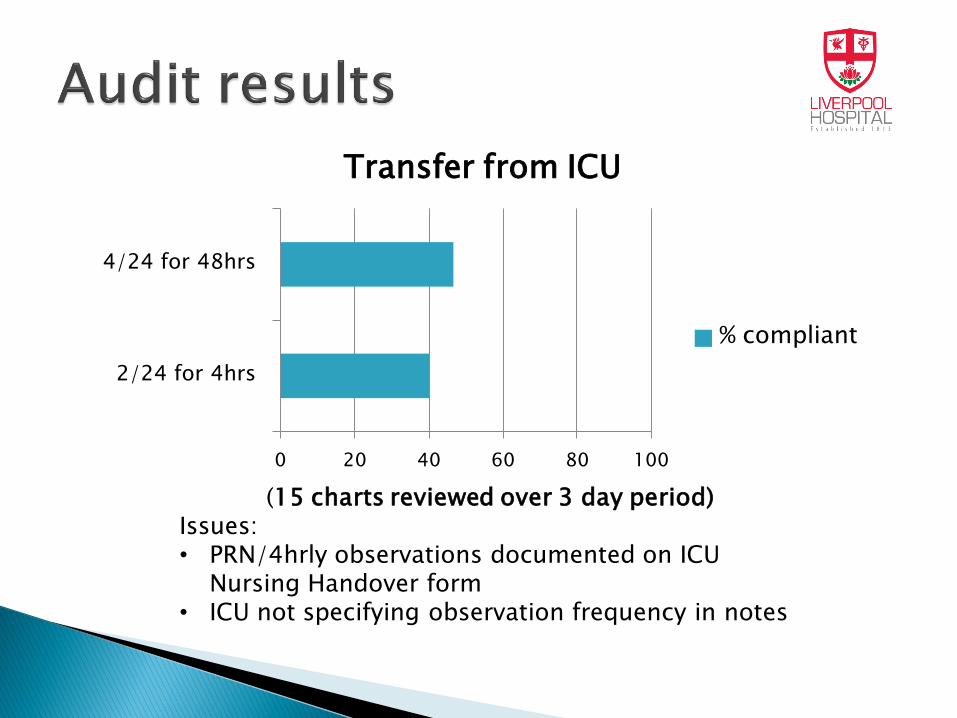
Transfer from ICU
% compliant
(15 charts reviewed over 3 day period) Issues: • PRN/4hrly observations documented on ICU
Nursing Handover form • ICU not specifying observation frequency in notes
Did it reach its intended audience ????
Was there buy in from clinicians
Discussed at hospital meetings
Results disseminated to NUMs and CNEs.
Policy was redistributed
For reauditing in 3 months
0 20 40 60 80 100
Obs 4th hourly for …
Obs 1hrly for 4hrs
Obs 1/2hrly for 2hours
Obs 15min during call
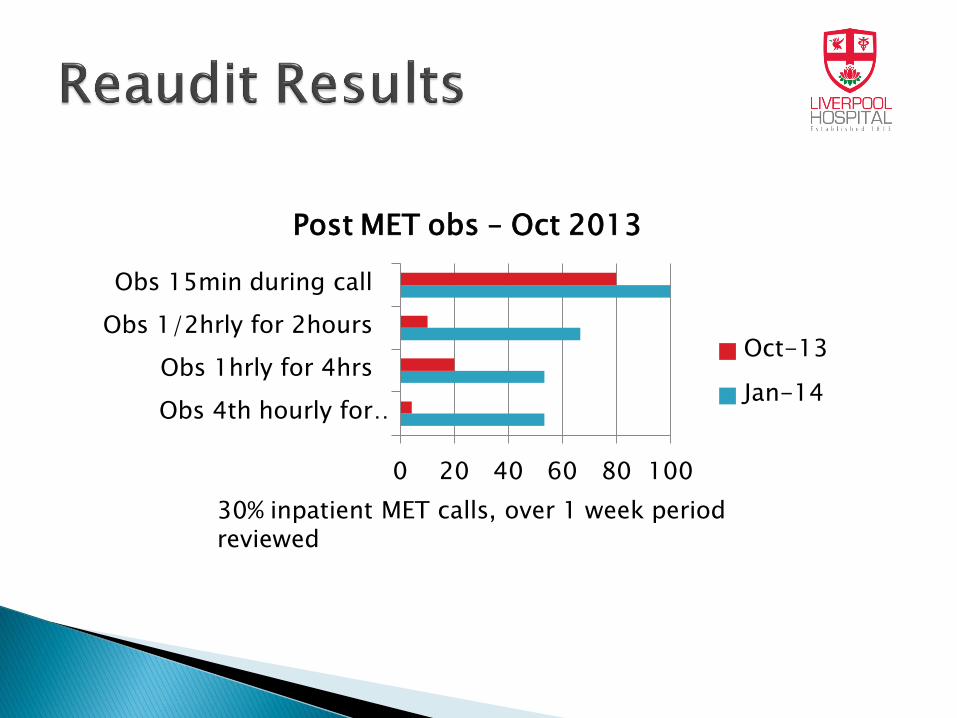
Post MET obs – Oct 2013
Oct-13
Jan-14
30% inpatient MET calls, over 1 week period reviewed
0 20 40 60 80 100
Obs 4th hourly for …
Obs 1hrly for 4hrs
Obs 1/2hrly for 2hours
CRC review within …
Obs 15min during call
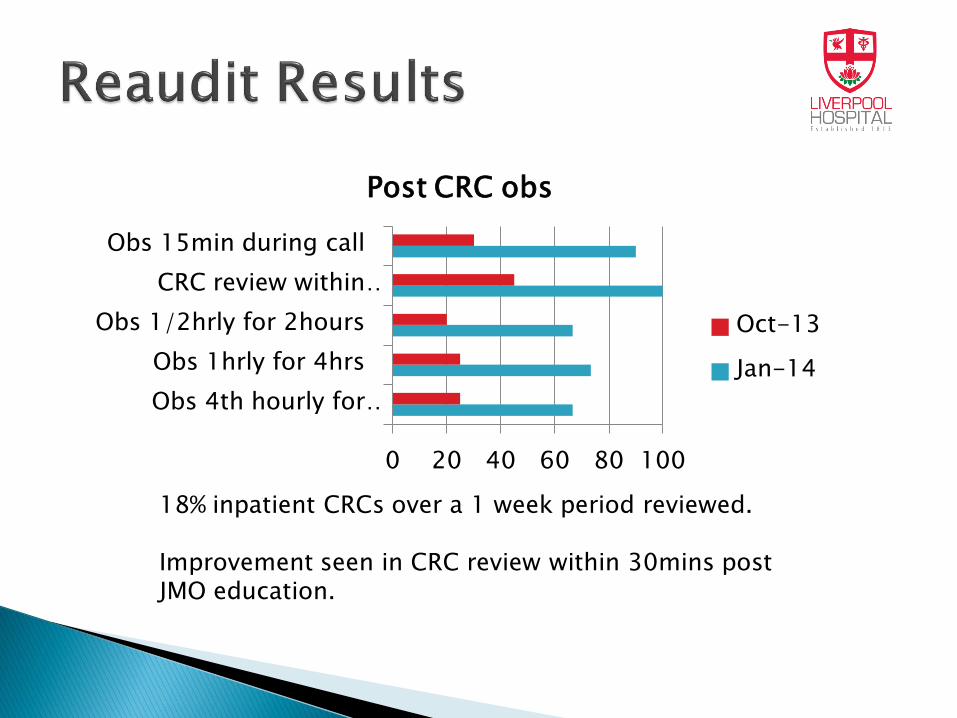
Post CRC obs
Oct-13
Jan-14
18% inpatient CRCs over a 1 week period reviewed. Improvement seen in CRC review within 30mins post JMO education.
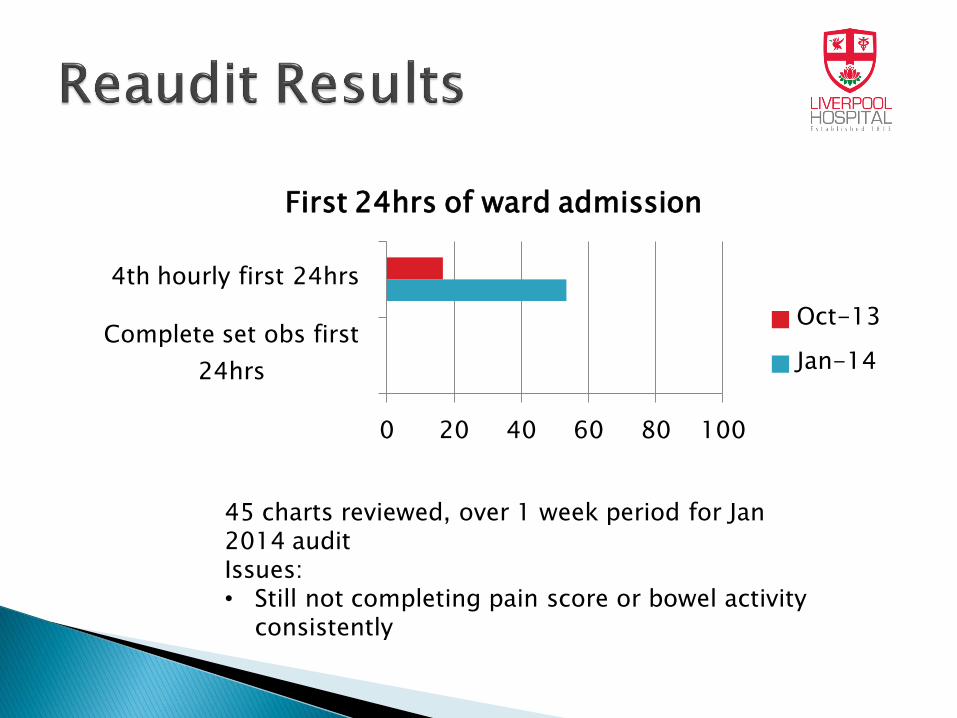
0 20 40 60 80 100
Complete set obs first
24hrs
4th hourly first 24hrs
First 24hrs of ward admission
Oct-13
Jan-14
45 charts reviewed, over 1 week period for Jan 2014 audit Issues: • Still not completing pain score or bowel activity
consistently
Audits conducted by CERs co-ordinator
Small sample
Improved compliance
Determined minimum target goal 85% compliance
ICU discharges not included
Bowel activity as minimum data set unreasonable was to be documented for each set of observations– changed to TDS/once per shift
ICU discharge paperwork states 4th hourly observations, not what policy says ◦ Previously overlooked
Introduction into existing education ◦ Mandatory Education
◦ Nursing orientation
Distribution of laminated summary sheet
Policy based education package ◦ Summary sheet
◦ Questions / answers
• ICU staff education re: policy requirements
• JMO education
Ward education package completed and approval given for release/use.
Request by DONM for wards to complete audits for 1 week of all MET and CRC activations in their ward as baseline. ◦ The results were sent to nursing executive officer
Final overall result presented to meetings
No follow up or improvement plan
Middle of busy winter period
Large audit load already in place on CNE/NUM
CNE relieving for staff deficits eg. Sick relief
Audit tool inappropriate for this application
As correlated by Nursing Executive Officer ◦ 77%
Concern with ongoing low results ◦ CERs co-ordinator and ICU Nurse Practitioner
candidate approached NEO with plan to Review results
Plan education around noted deficits in results
Review audit tool
Educators to commence education package roll out
Re-analysis on available audits ◦ 81%
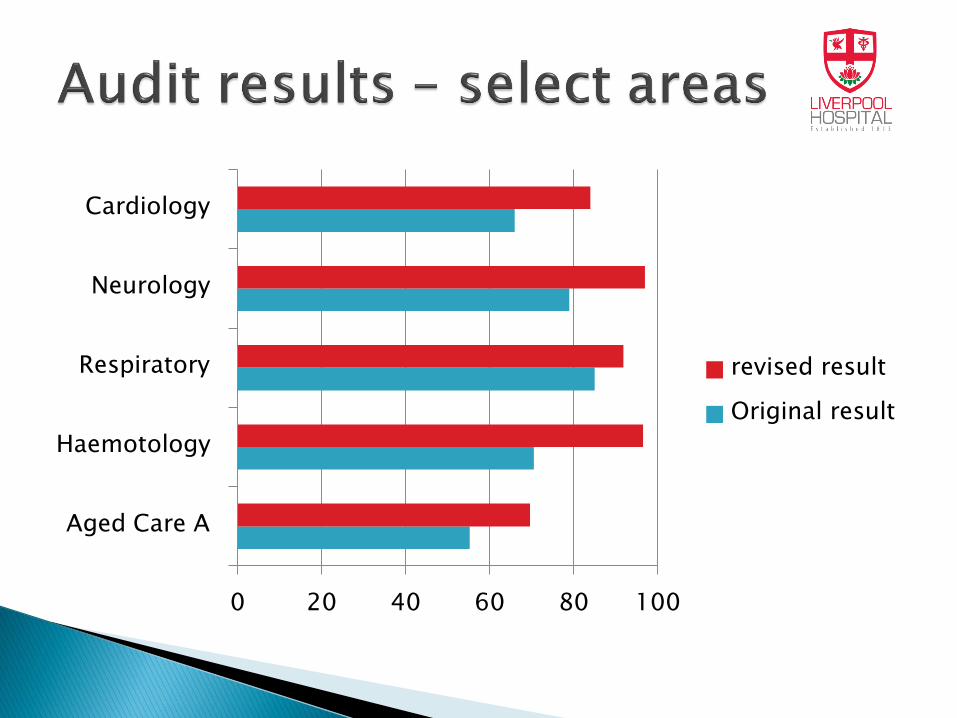
0 20 40 60 80 100
Aged Care A
Haemotology
Respiratory
Neurology
Cardiology
revised result
Original result
◦ Some used 1 form and averaged result
◦ Loss of points for non policy related questions
Calling criteria altered
Observation plan documented
◦ Feedback from users
Difficult to use
Not clear
Time consuming
Simplified
X5 patients audited on 1 A4 page
Audit now included ◦ Minimum data set
◦ Post ED transfer
◦ Post MET / CRC
◦ Post ICU transfer
◦ Post Recovery transfer
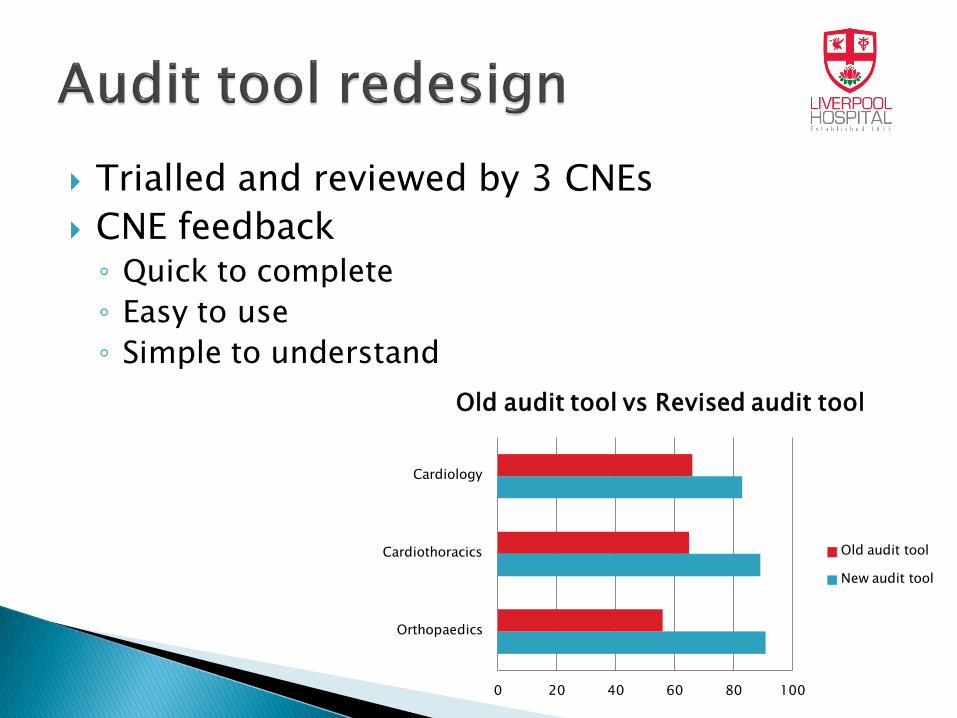
Trialled and reviewed by 3 CNEs
CNE feedback ◦ Quick to complete
◦ Easy to use
◦ Simple to understand
0 20 40 60 80 100
Orthopaedics
Cardiothoracics
Cardiology
Old audit tool vs Revised audit tool
Old audit tool
New audit tool

Education around deficits in audits ◦ Pain score
◦ Bowel score
◦ Overnight observations
◦ Why we need to complete these observations, not just another task!
Presenting at Nursing Ground Rounds ◦ Having presentation / supporting information available
to CNEs
◦ CERs co-ordinator and ICU Nurse Practitioner candidate presenting at ward in-services at CNE request
◦ CNEs able to present to ward staff.
Ward based reaudit ◦ December
to show results from education packages
◦ Ongoing bi-yearly audits
April and November – to avoid busier winter months
Discuss areas of improvements to practice and policy. Is it acceptable not to take obs on patients at night
How do you look at resp effort, without waking pts
Why is resp rate not included
Include clinicians in decision making
Ensure buy in
Ensure information reaches its intended audience
Ask for feedback re policies
The audit tool has to be useful
Feedback to staff- what they are doing well and what we can improve upon

Change our language from passively observing to measuring what is VITAL
VITAL SIGNS