Embed Size (px)
Citation preview

Management of prostate cancer

• Low risk: PSA < 10ng/ml and Gleason < 6 andThe percentage of involved cores is < 50% orIntermediate risk with only 1 positive core
• Intermediate risk: Gleason score of 7 or PSA of 10-20 Low risk with > 50% of positive cores orHigh risk and only 1 positive core
• High risk: Gleason > 8 or PSA > 20 and more than 1 positive core Or intermediate risk and more than 50% positive cores

• Watchful waiting refers to monitoring the patient until he develops metastases that require palliative treatment.
• Active surveillance or expectant management allows delayed primary treatment if there is biochemical or histologic evidence of cancer progression
Dall’Era et al, 2012

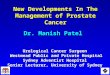
Active surveillance(AS)
• Observed with semiannual PSA determinations and DRE and annual biopsies
• Indicated– Patients with low-risk cancer and a life expectancy
<10 years– Patients with very low-risk cancer and a life
expectancy <20 years• African american and BRCA 2 mutation carriers
are not suitable for AS

• Carter et al. – Cohort of 769 men with very-low-risk prostate
cancer and low PSA density– 41% of patients had been treated at 5 years, and
59% at 10 years – Median time to treatment was 6.5 years. – Cancer control after delayed therapy was excellent
• AS is now widely recommended for most men with low-risk cancer, based on the lack of survival benefit of immediate surgery versus observation at 12 years in the PIVOT trial

• Intervention is recommended – Gleason pattern 4 5 or is present, – More than two biopsy cores are involved, or – More than 50% of a biopsy core is involved. – Progression is more likely in patients who have cancer
present on every biopsy procedure.– The absence of cancer on repeated biopsy significantly
decreases the likelihood of progression (Carter et al, 2007).– Biopsy criteria have been reported to be more accurate
than PSA criteria in predicting progression

• Overdiagnosis often refers to a cancer detected by screening that would not be detected during the patient’s lifetime without screening or would never cause disability or death
• 50% or more of prostate cancer cases are overdiagnosed (Etzioni et al, 2002; Draisma et al, 2003)
• At present, no tumor marker or algorithm can identify indolent tumors with certainty

• Disadvantages– Up to one half of patients are upgraded on the basis of the
radical prostatectomy specimen– Repeated biopsies are always subject to sampling errors
(Harnden et al, 2008) and – May induce fibrosis in and around the prostate gland that could
compromise subsequent nerve-sparing surgery, rendering it impossible to perform in more than half of patients (Barzell and Melamed, 2007)
– Trigger inflammation leading to PSA fluctuations that are difficult to interpret
– Patients undergoing active surveillance and radical prostatectomy have a similar quality of life in most domains at 5 years of follow-up
– 6 to 8 years, active surveillance groups have more anxiety and depression

Radical Prostatectomy
• Gold standard• Hormone therapy and chemotherapy are never
curative• Not all cancer cells can be eradicated consistently by
radiation or other physical forms of energy, even if the tumor is contained within the prostate capsule
• If the prostate gland remains in situ, it is possible for new prostate cancers to develop in the retained prostatic epithelium

• Advantage of radical prostatectomy– Possibility of cure with minimal collateral damage to surrounding
tissues if it is skillfully performed – Provides more accurate tumor staging by pathologic examination
of the surgical specimen.– Treatment failure is more readily identified, – Tumor recurrence after radical prostatectomy can be successfully
treated with potentially curative postoperative radiotherapy – Postoperative course is much smoother than in the past.
• Few patients require nonautologous blood transfusions. • The hospital stay is usually 1 to 3 days, and operative
mortality is rare in the modern era– Radical prostatectomy significantly reduces local tumor
progression and distant metastases and improves cancerspecific and overall survival rates compared with watchful waiting

• Disadvantages of radical prostatectomy– Necessary hospitalization and recovery period; a – Possibility of incomplete tumor resection, – If the operation is not performed properly or if the tumor is
not contained within the prostate gland– Risk for erectile dysfunction and urinary incontinence.
• Erectile dysfunction and rectal complications are less likely with nerve-sparing surgery than with radiotherapy, and
• Good treatment options are available to treat both urinary incontinence and erectile dysfunction.
– Results reported from high-volume centers are more favorable than those from national surveys

• Surgical Approaches to Radical Prostatectomy– Open• Perineal• Retropubic
– Minimal invasive• Laparoscopic–Transe peritoneal–Retroperitoneal
• Robotic

• The principal objective of radical prostatectomy is to completely excise the cancer
• Other objectives are remain continent and preserve potency• The key to preserving urinary continence is to perform a meticulous
dissection, avoiding injury to the external urinary sphincter.• Meticulous dissection is also required to preserve the neurovascular
bundles• Hemostatic sutures or clips may be used to control bleeding from the
neurovascular bundles. Use of electrocautery or a harmonic scalpel risks irreversible thermal injury to the neurovascular bundles
• The prostatic pedicles are suture ligated or hemoclipped and divided close to the gland, avoiding incision into the prostatic capsule.
• In performing the seminal vesicle dissection, care must be taken to avoid injury to the neurovascular bundles situated immediately lateral and posterior to thems

• Perineal– Less blood loss– Short operative time– Disadvantages• Does not provide access to lymph nodes• High rates of rectal injury• Occasional post operative fecal incontinence• Difficulty to spare cavernous nerves

• Retropubic– Familiarity with surgical anatomy– Low risk of rectal injury and fecal incontinence– Wide exposure– Ready access to pelvic lymph nodes– Low risk of cancer at surgical margin– Preservation of neurovascular bundle

• Laparoscopic RP– Associated with less bleeding, better visualization, less postoperative
pain, and shorter convalescence than the standard open approach– Hemostasis in the neurovascular bundles is difficult to achieve without
applying – Thermal injury to the neurovascular bundles
• Relative difficulty in rapidly placing hemostatic sutures or applying hemostatic clips laparoscopically.
• Heat from a harmonic scalpel or electrocautery can irreversibly damage the cavernous nerves
– Rectal, ureteral, and vascular injuries and anastomotic leaks have also been more common with laparoscopic prostatectomy in some studies

• The early reported rates of positive surgical margins have been higher with laparoscopic prostatectomy, and the adequacy of cancer control is as yet uncertain because of lack of long-term results
Touijer et al, 2009

• Robotic RP– Greater technical ease for the surgeon, especially for tying
sutures and performing the vesicourethral anastomosis– Lower blood loss three-dimensional (3D) visualization– Enhanced dexterity– No superiority was seen between robotic and open radical
prostatectomy for functional or oncologic outcomes • Pierorazio et al, 2013a; Silberstein et al, 2013
– Robotic prostatectomy was associated with a trend toward more urinary incontinence and no difference in sexual function compared with open radical prostatectomy• Barry et al, 201
– Significantly lower transfusion rate and shorter hospital stays compared with open radical prostatectomy (Tewari et al, 2012; Sammon et al, 2013) but a
– higher rate of incisional hernias (Carlsson et al, 2013).


• The importance of the surgeon’s experience in reducing complications is well documented (Vickers et al, 2007, 2009; Klein et al, 2008; Abboudi et al, 2014; Thompson et al, 2014; Vickers, 2014)
• Patients considering surgical treatment of their prostate cancer should be not to choose a technique but to choose an expert in a given technique

• Patient selection– Healthy and free of comorbidities– Life expectancy of at least 10 years– Generally accepted upper age limit for radical
prostatectomy is about 76 years– Neoadjuvant hormone therapy does not enhance
the resectability of prostate cancer and often increases the difficulty of performing nerve-sparing surgery
– Neoadjuvant chemotherapy rarely produces pathologic complete responses

– Nerve-sparing surgery is questionable• Extensive cancer in the biopsy specimens• Palpable extraprostatic tumor extension• Serum PSA level above 10 ng/mL• Biopsy Gleason score higher than 7 • Poor-quality erections preoperatively • Current and future lack of a sexual relationship• Medical conditions that may adversely affect erections
(e.g., diabetes mellitus, hypertension, psychiatric diseases, neurologic diseases, or medications that produce erectile dysfunction)

• Surgical Technique
1. Pelvic lymphadenectomy2. Opening of the endopelvic fascia and limited incision of the
puboprostatic ligaments3. Suture ligation and transection of Santorini dorsal venous complex4. Dissection of the urethra at the apex of the prostate and transection
of the urethra (sometimes the anastomotic sutures are placed at this point in the operation)
5. Dissection of the prostate from the neurovascular bundles6. Securing and transection of the prostatic pedicles7. Transection and reconstruction of the bladder neck8. Dissection of the seminal vesicles and ampullary portions of the
vasa deferentia9. Performance of the vesicourethral anastomosis

• Failure after RP was defined as a rising serum PSA >0.2 ng/ml, clinical evidence of local or distant recurrence, or the initiation of adjuvant radiotherapy or hormonal treatment
• At 5 years 84% of patients, at 10 years 78%, and at 15 years 73% were free of progression

• The hazard of prostate cancer–specific recurrence continues to increase for at least 15 years after radical prostatectomy, and the risks for mortality may increase for 25 years or more (Shikanov and Eggener, 2011; Bill-Axelson et al, 2014)
• It is important to continue to monitor patients long after surgery

• Pelvic Lymph Node Dissection– Restrict PLND at the time of RP to men with a ≥2% risk of positive
nodes according to a contemporary nomogram• Limited Versus Extended Pelvic Lymph Node Dissection
– No prospective studies have demonstrated the optimal anatomic limits of a PLND for prostate cancer
– PLND that includes the external iliac, hypogastric, and obturator node packets is feasible in both open and minimally invasive RP, and carries no greater risk than a PLND limited to the external iliac nodes alone
– The more extensive the PLND, the greater the number of LN removed, and the greater the number of positive nodes.

• Therapeutic Benefit of Pelvic Lymph Node Dissection– Potential therapeutic benefit of extended PLND,
particularly in men with only one or two positive nodes and Gleason score ≤7 in cancer identified in the RP specimen
– In a series of patients with positive LN treated at Johns Hopkins Hospital, men who had an extended PLND were less likely to develop BCR at 5 years, compared with men who underwent a limited PLND


• Complications– Early complications include hemorrhage; rectal,
vascular, ureteral, and nerve injury; urinary leak or fistula; thromboembolic and cardiovascular events; urinary tract infection; lymphocele; and wound problems
– Late complications of radical prostatectomy are erectile dysfunction, urinary incontinence, inguinal hernia, incisional hernia with laparoscopic and robotic prostatectomy, and urethral stricture

• Urinary Continence– High-volume radical prostatectomy surgeons, more
than 90% of men recover complete urinary continence. – The return of urinary continence is associated with the
patient’s age:• Approximately 95% of men younger than 60 years can attain
pad free urinary continence after surgery; 85% of men older than 70 years regain continence.
– Relatively few require implantation of an artificial urinary sphincter or a sling procedure for stress urinary incontinence.

• Erectile Function– The return of erectile function after radical prostatectomy
correlates with the age of the patient, preoperative potency status, extent of nerve-sparing surgery, and era of surgery
– Erections usually begin to return as partial erections 3 to 6 months after surgery and may continue to improve for up to 3 years or more
– Patients should be encouraged to use erectile aids postoperatively, including PDE5 inhibitors, intraurethral suppositories, intracavernosal injections, or vacuum erection devices

• Scandinavian randomized trial (SPCG-4)– 695 unscreened men with clinically localized prostate
cancer– Over 23 years of follow-up, – RP compared with watchful waiting• Reduced the risk of death from any cause by 29%• Risk of death from prostate cancer by 44% (an absolute
difference of 11%).• The need for subsequent ADT was reduced by 51%, • Clinical local recurrence was reduced by 66%.

• Prostate Cancer Intervention Versus Observation Trial (PIVOT)– United States and randomly assigned 731 men with clinically
localized prostate cancer to RP or observation– mean age was 67, the median PSA level was 7.8 ng/ml, and
approximately three-quarters of the men had a biopsy as a consequence of an elevated PSA, half had no palpable tumor (cT1c) and 70% had low-grade (Gleason ≤6) cancer on biopsy
– Median of 10 years of follow-up, – 48% of the patients had died, but only 7% had died from prostate
cancer. – There were no differences in overall or cancer-specific mortality
between the two arms of the trial. – But there were clear indications that RP reduced the risk of dying of
cancer in the subset of men who had aggressive cancers, including• Those whose PSA was >10.0 ng/ml and • Those with high-risk cancers

• two trials indicate that most men with cancers detected without screening and those with screen-detected intermediate- and high-risk cancers have less risk of metastases and of death from prostate cancer when treated with early RP than with observation alone
• Men with screen-detected low-risk cancer can be managed safely with AS and do not need immediate surgery or radiotherapy.

• Management of Postoperative Biochemical Recurrence– Biochemical recurrence afterRP
• 50% of recurrences appear within 3 years • 80% within 5 years• 99% within 10 years
– Rarely, recurrences appear more than 15 years after RP – The PSA velocity or doubling time, the interval from
surgery to biochemical recurrence, and the Gleason score usually reflect how rapidly the tumor is likely to progress

• Adjuvant radiotherapy VS salvage radiotherapy– Radiotherapy administered proactively shortly
after surgery (after urinary continence has been attained) in patients with undetectable PSA levels is called adjuvant radiotherapy.
– In contrast, radiotherapy given selectively to men with detectable postoperative PSA levels is called salvage radiotherapy

• Adjuvant therapy should be strongly considered for patients with Multiple or very high-risk tumor features—that is, extensive extracapsular tumor extension, multiple or broad-based positive surgical margins, seminal vesicle invasion, and lymph node metastases.
• For patients with focally positive margins or minimal extracapsular tumor extension, monitoring PSA every 4 months with early salvage therapy being initiated when the PSA reaches 0.2 ng/ mL and is verified to be rising may be more appropriate.
• In patients with a limited life expectancy, and especially those with Gleason grade 6 or 7 tumors, PSA levels may be monitored to measure the PSA velocity to help determine whether salvage radiotherapy is necessary
Cotter et al, 2011; Karlin et al, 2013

Radiotherapy for Localized Prostate Cancer
• External beam or brachytherapy techniques is a second treatment option for men with clinically localized prostate cancers
• Intensity-modulated external beam radiotherapy (IMRT) has become a standard mode of treatment delivery
• Brachytherapy using permanent or temporary radioactive implants within the prostate alone or combined with IMRT

• High-dose IMRT alone (in the range of 80 Gy) or brachytherapy alone are excellent treatment options– Patients with low-risk disease in whom AS may not be
considered—owing to PSA velocity, the presence of a dominant lesion on imaging studies, or a larger volume of disease determined by biopsy
• Larger prostate volumes, the presence of urinary obstructive symptoms, and medical co morbidities – brachytherapy is contraindicated

• For patients with intermediate- and higher-risk disease, combined modality treatments including brachytherapy and supplemental IMRT are preferred to allow for the delivery of a high and concentrated dose of radiation to the prostate

• Intensity-Modulated Radiotherapy and Image-Guided Techniques– Clinical target volume (CTV) includes the entire prostate
gland and immediate periprostatic tissues, as well as the seminal vesicles, as visualized on CT
– Low-risk disease with unremarkable imaging studies, the CTV may exclude the seminal vesicles
– Use of image-guided approaches, the margin can be safely reduced to 5 mm to 6 mm around the CTV, except at the prostate-rectal interface, where an even tighter margin (3 mm to 5 mm) is used

– 10% to 20% improvement in 5- to 10-year PSA survival outcomes when higher doses of 78 Gy to 80 Gy are applied, compared with dose levels of 70 Gy, and such benefits have been observed for low-, intermediate-, and high-risk cohorts
– For patients with intermediate- and especially high-risk disease, doses beyond 80 Gy may be required to achieve optimal tumor control outcomes
– Complication rates after EBRT• Acute symptoms typically appear during the
third week of treatment–Acute intestinal symptoms–Internal and external hemorrhoids–Acute urinary symptoms

• Late rectal toxicities– 12 months to 18 months after completion of treatment– Rectal bleeding, mucous discharge, and mild incontinence of stool– More-severe toxicities, including ulcer development and fistula
formation, are observed in ≤1% of patients• Late urinary toxicities include chronic urethritis, which
occurs in approximately 10% to 15% of patients, and urethral strictures, which occur in 2% to 3%. Hemorrhagic cystitis
• Rates of impotence at 3 years or longer after EBRT ranges widely from 36% to 68%,

• Hypofractionated External Beam Radiotherapy– A pooled analysis of 1,100 patients treated from 2003 to 2011
at eight institutions – The median dose delivered for these patients was 36.25 Gy in
five fractions. – The median follow-up was 3 years;– the 5-year PSA-relapse-free survival rates were 95%, 84%, and
81% for low-, intermediate-, and high-risk patients, repsectively. – Stereotactic radiosurgery appears promising, but this form of
treatment cannot be considered an established form of radiotherapy delivery, and ongoing studies will define its role better in the years ahead.

• Role of Proton Therapy for Localized Prostate Cancer• Bragg peak—by which the majority of the energy of
the beam is deposited at the end of its track, creating a rapid falloff of dose beyond the target
• Proton therapy was associated with a lower risk of erectile dysfunction
• No established evidence that proton therapy provides superior tumor control outcomes, compared with well-delivered high-dose IMRT or image-guided radiotherapy, for the treatment of prostate cancer

• Prostate Brachytherapy– Transperineal ultrasound-guided approaches– Most commonly used radioisotopes for permanent seed
brachytherapy are iodine-125 (125I) and palladium-103 (103Pd)– The half-life of 125I is 60 days, with a mean photon energy of 27
KeV and an initial dose rate of 0.07 Gy/h– Half-life of 103Pd is 17 days, with a mean photon energy of 21
KeV and an initial dose rate of 0.19 cGy/h. – The active periods for 125I and 103Pd are 10 months and 3
months, respectively. – 125I is used, the typical prescription dose is 144 Gy; 125 Gy is
routinely used for 103Pd.

Prostate Brachytherapy
• The size of the prostate gland should preferably be <60 cm3 and optimally <50 cm3
• The size of the prostate can be effectively addressed with combined androgen-blockade therapy
• More suitable intervention for patients with – Bilateral hip replacements– Patients with small bowel in close proximity to the prostate
volume are also better suited to brachytherapy, owing to the lower doses to the bowel expected with brachytherapy
– History of inflammatory bowel disease

• Brachytherapy is seldom used for the treatment of high-volume, high-risk prostate cancers, because IMRT is the preferred method for treatment of aggressive tumors
• Proctitis and rectal injury are less common with brachytherapy than with external beam therapy, but erectile dysfunction occurs more commonly with brachytherapy than with external beam radiation.
• Other complications associated with brachytherapy include seed migration and rectourethral fistula

• Combined Brachytherapy and External Beam Radiotherapy– Increased dose of radiation that has been estimated to
have a biologic equivalent that well exceeds a 100-Gy dose of EBRT
– Brachytherapy combined with IMRT boost was associated with better PSA-relapse-free survival (hazard ratio [HR] = 0.40; 95% CI = 0.24 to 0.66; p <0.001) and better distant metastases–free survival (HR = 0.41 [0.18 to 0.92]; p = 0.03)
– Late toxicity outcomes were 4.6% versus 4.1% for grade 2 GI toxicity (p = 0.89), 0.4% versus 1.4% for grade 3 GI toxicity (p = 0.36), 19.4% versus 21.2% for grade 2 genitourinary toxicity (p = 0.14), and 3.1% versus 1.4% for grade 3 genitourinary toxicity (p = 0.74) for the IMRT versus the combination RT groups, respectively

• High-Dose-Rate Brachytherapy– Ultrasound-guided transperineal placement of afterloading
catheters in the prostate– High-dose fractions, ranging from 4 Gy to 6 Gy each, are
administered during an interval of 24 hours to 36 hours using 192Ir– Advantage of an afterloading approach, the
• Radiation oncologist and physicist can more easily optimize the delivery of radiotherapy
• Reduces radiation exposure to the radiation oncologist and others involved in the procedure
• Reduces radiation exposure to the radiation oncologist and others involved in the procedure

• Optimal Radiotherapeutic Approach for Localized Disease– Low-risk disease - brachytherapy as monotherapy or IMRT at
dose levels of 80 Gy would be appropriate and associated with biochemical outcomes of approximately 90% at 10 years• Patients with enlarged prostate glands of 60 ml to 90 ml are best
treated with ADT to reduce the size of the gland before brachytherapy– intermediate- or high-risk disease, doses higher than 80 Gy may
be necessary• Recommend for these patients brachytherapy in combination with
image-guided EBRT
• .

• ADT is used as adjuvant therapy– Improve local eradication of locally advanced tumors by
reducing tumor size, – Eliminate tumor clonogens inherently resistant to
radiotherapy by impairing DNA repair pathways, and/or – Reducing prostate volumes by 30% to 40%, which improves
the ability to deliver maximal radiation dose levels without exceeding the tolerance for the surrounding normal tissue.
– Hormone therapy also has a favorable effect on micrometastatic disease that may be present at the time of diagnosis in men with high-risk tumors

• EORTC 22863– Node-negative patients with clinical stage T3 disease
or T1–T2 patients with high-grade disease received adjuvant ADT on the first day of radiotherapy (prescribed dose of 70 Gy) and continued for 3 years
– 10-year overall survival was 58% versus 40% for patients treated with ADT plus EBRT and EBRT alone, respectively (p = 0.0004)
– 10-year PCSM rates for these respective cohorts of patients were 10% and 30% (p <0.0001)

• Duration of ADT was addressed in RTOG 92-02– Neoadjuvant and concurrent ADT for a total of 4 months
or the same therapy plus an additional 24 months of adjuvant ADT for a total of 28 months
– At a median follow-up of 5.8 years, the results showed that all outcomes were improved for patients who received 28 months with the exception of overall survival
– subset analysis, however, showed a 10% overall survival advantage for patients with Gleason scores of 8 to 10 who were treated with the longer course of ADT

• RTOG 94-13 evaluated two sequencing regimens of adjuvant ADT– Patients were randomized to receive either 4 months of
ADT before and during radiotherapy or 4 months of ADT as adjuvant therapy following the completion of EBRT
– Neoadjuvant and concurrent ADT in conjunction with whole-pelvic radiotherapy was associated with a trend for an improved progressionfree survival (PFS) compared to the other study arms (48% PFS for neoadjuvant ADT and whole-pelvic radiotherapy versus 40% for prostate only radiotherapy and adjuvant ADT; p = 0.065)





• Management of the Patient with Rising Prostate-Specific Antigen After Definitive Local Therapy– Biochemical failure after surgery is a detectable or rising PSA
level >0.2 ng/ml, with a second confirmatory increase >0.2 ng/m
– Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference.• Prostate specific antigen (PSA) failure as occurring after
three consecutive PSA rises after a nadir with the date of failure as the point halfway between the nadir date and the first rise or any rise great enough to provoke initiation of therapy• Rise by 2 ng/mL or more above the nadir PSA be
considered the standard definition for biochemical failure after EBRT with or without HT

• Salvage Radiotherapy for the Patient with Rising Prostate-Specific Antigen After Prostatectomy– Improved outcomes are achieved with salvage radiotherapy when
preradiotherapy PSA values are ≤0.5 ng/ml– MSKCC, 285 patients with increasing PSA levels after prostatectomy
- treated with either salvage three-dimensional CRT or IMRT• The 7-year (median follow-up, 5 years) PSA-relapse-free survival
and distant metastases–free survival rates were 37% and 77%, respectively
• Patients treated without any adverse prognostic features had a 5- year PSA-relapse-free survival of 70%, compared with 30% for those with any adverse feature
– Efficacy of salvage EBRT alone for clinically palpable local disease or imaging evidence of disease within the prostatic bed is suboptimal
– ADT can be used to improve local tumor eradication by reducing the size of a mass, by the concurrent elimination of tumor clonogens inherently resistant to radiotherapy, or both.

• Salvage Therapy for Locally Recurrent Disease After Radiation– Salvage RP, brachytherapy, or cryosurgery– Patient selection requires a performance status of 80 or more,
histologic confirmation of disease in the gland, and no evidence of metastatic disease by imaging
– Salvage Cryotherapy• With the development of second- and third-generation probes,
real-time TRUS for intraoperative monitoring, thermocouplers, and urethral warmers, cryotherapy is potentially less toxic
• Case selection criteria include a prostate volume between 20 g to 30 g
• Biochemical disease-free survival rates range from 34% to 98%• Reported long-term complications include erectile dysfunction
(77% to 100%), rectal pain (10% to 40%), urinary incontinence (4% to 20%), urinary retention (0% to 7%), and urethral sloughing (0% to 5%).302–307 Rectourethral fistulas, the most serious complication following cryotherapy, are relatively uncommon (0% to 4%)




Advanced Prostate Cancer
• Principle of treatment of advanced prostate cancer is to deplete androgens or inhibit signaling through the androgen receptor (AR)
• 1940s by Huggins and Hodges showed that surgical removal of the testes or the administration of exogenous estrogen could induce tumor regressions, reduce the level of acid phosphatase in the blood, and palliate symptoms of the disease



• Noncastrate Prostate Cancer (Rising Prostate-Specific Antigen and Noncastrate Metastases)– Bilateral orchiectomy is an inexpensive standard
treatment that reliably reduces testosterone levels to the “castrate” range (<50 ng/dl)
– Estrogens inhibit the production of LHRH, which decreases the release of follicle-stimulating hormone and LH, and reduces androgen levels in a dose-dependent manner. A dose of diethylstilbesterol (DES), 3 mg/d, generally achieves castrate testosterone levels.

• LHRH agonists produce an initial rise in LH that increases testosterone levels, followed 1 to 2 weeks later by downregulation of LH receptors that results in a medical castration– The initial rise in testosterone can flare the disease,
precipitating or exacerbating symptoms such as pain, obstructive uropathies, and spinal cord compromise
• LHRH antagonists produce castrate levels of testosterone in 48 hours without the initial rise– Initial treatment of patients with symptoms

• Antiandrogens– Block the binding of testosterone to the AR– Steroidal type I agents - cyproterone acetate have
progestational properties that suppress LH levels and lower serum testosterone; these are not widely used.
– The nonsteroidal type II agents bind to the AR and act as competitive antagonists for ligands.
– The three first-generation type II agents approved are • Flutamide - short half-life requiring multiple daily doses,
and • Bicalutamide and nilutamide - weekly half-lives and are
administered once daily.

– All three were approved initially in combination with a LHRH analog: – Flutamide to prevent the flare that can result from the initial rise in
testosterone that occurs with LHRH analogs, bicalutamide (50 mg daily) on the basis of an improved safety profile relative to flutamide
– Nilutamide in combination with surgical orchiectomy based on greater efficacy relative to orchiectomy alone
– Type II agents given as monotherapy do not inhibit LH synthesis in the hypothalamus or pituitary, and circulating testosterone levels rise.
– None of these antiandrogens are approved as monotherapy in the United States, although bicalutamide 150 mg is approved in the European Union

• Enzymatic Inhibitors of Androgen Synthesis– Ketoconazole
• Nonspecific P450 inhibitor that• Dose of 1,200 mg/d, • Produces castrate levels of testosterone in 24 hours through
inhibition of adrenal and testicular steroidogenesis• The effect is not durable, limiting the drug’s use as first-line
treatment. • It was useful for patients who presented with acute spinal cord
compression or disseminated intravascular coagulation, when LHRH analogs are contraindicated and the risk of hemorrhage from surgery is significant

• In a meta-analysis of 10 randomized controlled trials that included LHRH agonists/antagonists, orchiectomy, DES, or choice of DES or orchiectomy, outcomes were similar.
• 27 randomized trials with 8,275 patients, showed a 2% difference in mortality at 5 years: 72.4% for monotherapy versus 70.4% for the combined approach; a second meta-analysis limited to trials of a nonsteroidal antiandrogen showed a 2.9% difference: 75.3% versus 72.4% at 5 years. None proved meaningfully superior

• The Veterans Administration Research Service Cooperative Urological Research Group trials enrolled 1,900 patients staged primarily by DRE– DES or orchiectomy could delay the development of
metastatic disease in patients with locally advanced tumors, although overall survival was worse due to cardiovascular complications.
– There was also no overall survival benefit for patients with metastatic disease

• MRC PR03 trial randomized 998 patients– Patients treated with early therapy were less likely
to require a TURP or develop ureteral obstruction, progress from M0 to M1 disease (P <0.001, two-tailed), to develop pain (P <0.001), or to die of prostate cancer relative to those in whom therapy was “deferred.” Even so, survival times were similar between the two groups

• Toxicities of Androgen Deprivation Therapy– Androgen deprivation syndrome include hot flashes, a
decrease in libido, erectile dysfunction, impotence, fatigue, anemia, weight gain and alterations in fat metabolism, loss of muscle mass and weakness, bone loss, a decrease in mental acuity, mood swings, personality changes, memory loss, depression, and insomnia
– Many of the adverse effects of ADT can be relieved by exercise– Hot flashes
• Occur in more than 80% of patients at any time, even during sleep, and may last for several seconds or an hour or more.
• They are bothersome in about 25% of cases• If significant, can be reduced in frequency and intensity with
estrogens at doses as low as 0.3 mg/d by patch or progestins (e.g., megestrol acetate or medroxyprogesterone acetate)


• Androgen deprivation is one of the most effective therapies against any solid tumor; unfortunately, with time almost all prostate cancers will become androgen refractory.
• All current forms of androgen deprivation therapy (ADT) function by either lowering levels of circulating androgens or blocking the binding of androgen to the androgen receptor.
• Almost all castration-resistant prostate cancer remains sensitive to androgen; therefore ADT should continue in castration-resistant disease.
• Relative to testosterone and dihydrotestosterone, the adrenal androgens are weak.• There are four general forms of ADT: (1) ablation of androgen sources, (2)
antiandrogens, (3) inhibition of LHRH and/or LH, and (4) inhibition of androgen synthesis.
• Bilateral orchiectomy reduces testosterone by 90% within 24 hours of surgery.• Nonsteroidal antiandrogens cause LH and testosterone levels to increase.• Serious liver toxicity is a possible side effect of all antiandrogens.• Antiandrogens can act as agonists on some tumors; antiandrogen withdrawal
results in PSA declines in 15% to 30% of patients.• Bicalutamide 150 mg monotherapy appears to have equivalent efficacy to medical
or surgical castration for locally advanced or metastatic prostate cancer.• Enzalutamide improves overall survival in metastatic, castration-resistant prostate
cancer after treatment with chemotherapy

Abiraterone improves overall survival in metastatic, castrationresistant prostate cancer both before and after treatment with chemotherapy.
• All LHRH agonists induce a testosterone increase upon initial exposure. Coadministration of an antiandrogen functionally blocks the effects of testosterone.
• The magnitude and rapidity of the initial response to ADT are strong predictors of the durability of that response.
• The side effects of ADT include osteoporosis, hot flashes, sexual dysfunction, cognitive function alterations, changes in body habitus, gynecomastia, and anemia. These side effects can be
progressive but are responsive to other treatments.• There is no evidence that 3 months of neoadjuvant ADT prior to radical prostatectomy
improves biochemical outcomes.• There is considerable evidence that ADT combined with external beam radiation therapy
improves overall survival, cancerspecific survival, and freedom from disease progression. The optimal timing and duration of ADT in this combination remains undefined.

• Based on a large meta-analysis of many clinical trials, combined androgen blockade with nonsteroidal antiandrogens provides about a 3% survival benefit at 5 years compared to standard ADT.
• The natural history of prostate cancer progression is protracted. Many men with evidence of disease will never require ADT.
• The use of ADT in low-risk, localized prostate cancer increases overall (non–prostate cancer) mortality.
• In lymph node metastatic prostate cancer, ADT improves overall survival if the primary tumor is removed but has no significant effect if the primary tumor is not removed

• Follow-up after hormonal therapy• Patients should first be evaluated at 3 and 6
mo after the initiation of treatment• As a minimum, tests should include serum PSA
measurement, DRE, serum testosterone, and careful evaluation of symptoms to assess treatment response and side effects.


Castration-Resistant Prostate Cancer
• Castrate serum levels of testosterone (testosterone <50 ng/dl or <1.7 nmol/l).
• Three consecutive rises of prostate-specific antigen (PSA), 1 wk apart, resulting in two 50% increases over the nadir with PSA >2.0 ng/ml.
• Antiandrogen withdrawal for at least 4 wk for flutamide and for at least 6 wk for bicalutamide.
• PSA progression, despite consecutive hormonal manipulations. • Progression of osseous lesions: progression or appearance of two
or more lesions on bone scan or soft tissue lesions using Response Evaluation Criteria in Solid Tumours and with nodes >2cm in diameter.


• Nonmetastatic Castration-Resistant Prostate Cancer– At present there is no consensus regarding the
most appropriate management for patients with nonmetastatic CRPC
– Sequential endocrine approach (using second-generation agents, e.g., ketoconazole) is the most commonly used therapeutic modality.

Metastatic Castration-Resistant Prostate Cancer
• Cytotoxic Chemotherapy– Docetaxel is the standard first-line chemotherapy for
mCRPC. It prolongs progression-free and overall survival, ameliorates pain, and improves quality of life.
– Toxicity of docetaxel includes myelosuppression, fatigue, peripheral edema, neurotoxicity, hyperlacrimation, and nail dystrophy.

• TAX 327– From March 2000 through June 2002, – 1006 men with metastatic hormone-refractory prostate
cancer received 5 mg of prednisone twice daily and were randomly assigned to receive • 12 mg of mitoxantrone per square meter of body-surface area every
three weeks, • 75 mg of docetaxel per square meter every three weeks, or • 30 mg of docetaxel per square meter weekly for five of every six
weeks– The median survival was 16.5 months in the mitoxantrone
group, 18.9 months in the group given docetaxel every 3 weeks, and 17.4 months in the group given weekly docetaxel
– When given with prednisone, treatment with docetaxel every three weeks led to superior survival and improved rates of response in terms of pain, serum PSA level, and quality of life, as compared with mitoxantrone plus prednisone.

– Cabazitaxel has emerged as a second-line chemotherapy option for patients with mCRPC who have had progressive disease during or after docetaxel treatment.
– Novel tubulin-binding taxane– Poor affinity for P-glycoprotein, the adenosine
triphosphate–dependent drug efflux pump– Toxicity of cabazitaxel includes neutropenia
(including febrile neutropenia) and diarrhea

• Pivotal randomized phase III (TROPIC) trial– Conducted in 146 institutions across 26 countries, which
recruited 755 men with mCRPC who had progressed after docetaxel-based chemotherapy
– 377 patients were randomized to receive mitoxantrone 12 mg/m2 intravenously every 3 weeks (with oral prednisone 10 mg daily), and 378 patients were assigned to receive cabazitaxel 25 mg/m2 intravenously every 3 weeks (plus prednisone)
– After a median follow-up of 12.8 months, overall survival in men receiving cabazitaxel was 15.1 months compared to 12.7 months in men receiving mitoxantrone (HR 0.70, P < .0001)

• Although it does not prolong survival, mitoxantrone has been approved to palliate symptoms associated with metastatic disease, and it is often used in patients who have previously received docetaxel and/or cabazitaxel, or in those who would not tolerate these agents.

• ANDROGEN RECEPTOR– DIRECTED APPROACHES– There is mounting evidence that CRPC is not androgenindependent
and continues to rely on androgen/AR signaling.– Abiraterone is a CYP17 inhibitor that depletes adrenal and
intratumoral androgens. It is approved for the treatment of mCRPC, both before and after chemotherapy.
– Enzalutamide is a novel AR signaling inhibitor that blocks the AR and prevents nuclear translocation and DNA binding. It was shown to improve survival in men with mCRPC both in the prechemotherapy and postchemotherapy settings.
– Additional CYP17-targeting agents (e.g., orteronel) and AR-targeting agents (e.g., ARN-509) are in clinical development.

• IMMUNOTHERAPY– Sipuleucel-T is the first therapeutic vaccine to be approved by the FDA
for the treatment of any cancer, and it is indicated for men with asymptomatic or minimally symptomatic mCRPC without visceral metastases or cancer-related pain requiring narcotics.
– ProstVac-VF is a poxviral-based PSA-directed prostate cancer vaccine that is administered by subcutaneous injection. It is currently in phase III testing for men with asymptomatic or minimally symptomatic mCRPC.
– Ipilimumab shows promising clinical activity in men with mCRPC, although a large trial in docetaxel-pretreated patients narrowly missed its primary survival end point. Although ipilimumab is not currently FDA-approved for prostate cancer, an ongoing trial is evaluating ipilimumab in men with mCRPC who have not yet received chemotherapy.
– The future of prostate cancer immunotherapies is likely to involve their use in the early-disease setting, or in combination with other standard prostate cancer therapeutics (hormone therapy and radiotherapy).

• NOVEL TARGETED TREATMENTS– Despite negative studies with bevacizumab and aflibercept,
angiogenesis remains a valid therapeutic target in prostate cancer, as exemplified by the novel agent tasquinimod.
– Because of the reciprocal interactions between the PI3K/Akt/ mTOR pathway and the AR signaling pathway, dual inhibition of both pathways concurrently will likely represent the most fruitful therapeutic strategy.
– Cabozantinib is a novel small molecule inhibitor of c-Met and VEGFR2, with profound activity on CRPC bone metastases.
– Custirsen is an antisense oligonucleotide against clusterin mRNA, which may play a role in reversing resistance to taxane chemotherapies


• PALLIATIVE MANAGEMENT– Patients with back pain and a history of bone metastases should be
evaluated for epidural cord compression. The clinical syndrome often includes at least one of the following signs and symptoms: back pain, focal neurologic deficit (leg weakness, sensory levels), or changes in bladder or bowel control.
– Initial management of suspected cord compression includes immediate MRI of the spine and initiation of high-dose intravenous corticosteroid therapy. Definitive treatment should include radiation therapy, surgical decompression, or both.
– Zoledronic acid and denosumab are both reasonable treatment options for the prevention of skeletal-related events in patients with castration-resistant bone metastases. Denosumab may include the advantage of not requiring renal dosing. Both agents can (rarely) cause ONJ.
– Radium-223 is a novel alpha-emitting radiopharmaceutical that the FDA has approved for the treatment of symptomatic bone metastases in CRPC patients without visceral metastases or bulky lymph node disease. The recommended dose is 50 kBq/kg intravenously every 4 weeks for a total of 6 cycles.

THE NEUROENDOCRINE/ANAPLASTIC PHENOTYPE

• These tumors are invariably unresponsive to hormonal manipulations but are transiently sensitive to radiation therapy and chemotherapy including platinum-etoposide combinations (or platinum-docetaxel combinations).