Embed Size (px)
Citation preview

Facial fractures
Conor DalbyACCS ST2

Contents• History
• Clinical features
• Investigations in facial trauma
• Analysis of mid-face injury
• Orbital blow-out fracture
• Injuries to the mandible
• Le Fort
• Management

History Once the ABCs have been stabilised and a basic history of the event and PMH has been obtained, seek to answer the following questions:
1. Can you breathe out your nose on both sides?
2. Are you having any trouble speaking?
3. Any new visual disturbance?
4. Is your hearing normal?
5. Are you experiencing any numbness of your face?
6. Do your teeth come together as they normal would?
7. Any painful or loose teeth?

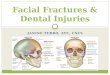
Clinical signs of facial fractures
sublingual haematoma
Clinical Sign Underlying pathologyFlattened cheek Depressed zygomatic fracture‘Dish face’ deformity, or elongated face Mid-face fracturesSaddle deformity of the nose Naso-ethmoidal fractureUneven pupils/diplopia Orbital floor fractureCSF rhinorrhoea Base of skull fractureSubconjunctival haemorrhage without posterior border Orbital wall fractureHypothesia: • Numbness of the cheek, side of nose, and upper
lip/teeth
• Numbness of the lower teeth and lip
Orbital floor fracture damaging the infraorbital nerve
Mandibular fracture damaging the inferior dental nerve
Subcutaneous emphysema Facial fracture into sinusDental malocclusion Maxillary or mandibular fractureSublingual haematoma or gum laceration Mandibular fractures

‘Dish face’ deformity: mid-face fracturesFlattened cheek: depressed zygomatic fracture
Subconjunctival haemorrhage without posterior border:Orbital wall fracture

Investigations for facial trauma• ‘Facial views’ -
Occipitomental views are required in two planes
• Mandibular AP view and orthopantomogram (OPG) are required for mandibular injuries. OPG alone may miss Symphysis menti fracture.
• Nasal X-rays are not indicated
• CT scanning may be required to plan surgical intervention but is best organised by the maxillofacial team.

Analysis of a mid-face injuryThink of the zygoma as a mid face stool with 4
legs.
Concentrate on the stool’s legs. For each leg, compared the injured side to the other (normal) side. Look for any asymmetry or any difference between the appearance of the matching legs. Check as follows:
•Leg 1: zygomatic arch•Leg 2: frontal process of the zygoma•Leg 3: orbital floor/rim•Leg 4: lateral wall of the maxillary antrum•Look for fractures and look for:
• a fluid level in the maxillary antrum• sinus air in the soft tissues or in the orbit
NOTE: If any one leg is fractured, always double check that the other legs are intact (looking for ‘tripod’ fracture)

Isolated fracture of the zygomatic arch. This is a common injury (arrow)
Fracture of the inferior orbital margin.
This may occur in isolation or as part of a tripod
fracture

‘Tripod fracture’. In this combination injury the cheekbone (zygoma) is detached from its four points of attachment to the rest of the facial skeleton

Orbital blow-out fracture
Following blunt trauma, this injury may be isolated, or accompany any other major or minor facial injury. It results from a direct compressive force to the globe. A squash ball or a thrown egg are easy ways to do this.
The blow causes a sudden increase in the intraorbital pressure behind the eyeball. resulting in fracture(s) of the thin and delicate plates of bone that form the floor an medial wall of the orbit.

Injuries to the mandible

Le Fort (mid-face fractures)We can’t discuss facial fractures without mentioning le fort. He subjected cadaveric skulls to a
variety of blunt trauma and found 3 predominant patterns of fracture:
1.Le Fort I: fracture involving the tooth bearing portion of the maxilla. There may be an associated split in the hard palate, a haematoma of the soft palate, and malocclusion.
2.Le Fort II: fracture involving the maxilla, nasal bones and medial aspect of the orbit. The maxilla may be floating and cause potential airway obstruction.
3.Le Fort III: fracture involving the maxilla, zygoma, nasal bones, ethmoid and base of skull.
This is a useful classification for the maxillofacial surgeon when planning treatment. However, the Le Fort patterns are not particularly helpful when carrying out step-by-step assessment of the plain radiographs in the emergency department. As the Le Fort patterns involve the pterygoid plates, the only reliable detail would be found on a CT scan, not a plain film.

Other facial injuriesNasal fractures:
The most common facial fracture. The diagnosis is clinical and an Xray is not required.
A septal haematoma should always be assessed for, and if present, the patient should be urgently referred for incision and drainage to avoid septal necrosis.
ENT follow-up at 5-7 days allows assessment of the nose once the swelling has subsided.
Temporomandibular joint dislocation:
TMJ dislocation is usually sustained by a direct blow to an open jaw or following yawning/eating in patients with lax joint capsules/ligaments. Anterior dislocation is the most common, however they can occur in any direction when occurs with fractures of the mandible or base of skull.
Reduction of anterior dislocations can usually be achieved in the ED with the aid of analgesia and sedation. Following reduction, the patient should have a soft diet, and be advised not to open their mouth widely for 2 weeks.
Refer for outpatient maxillofacial follow-up.

Management of facial fractures
1. Resuscitate and establish a clear airway (ATLS)
2. Treat any epistaxis
3. Analgesia
4. Ensure appropriate tetanus prophylaxis
5. Avoid nose blowing (risk of surgical emphysema)
6. Prophylactic antibiotics may be indicated
7. Clean and cover facial lacerations, but do not close if associated with fractures, because they can provide access for surgical reduction.
8. Head injury assessment and advice
9. Refer to maxillofacial surgery

References• Stacey V. Revision notes for MCEM part B. Oxford University Press. 2012
• Raby N, Berman L, Morley S, de Lacey G. Accident and Emergency Radiology a survival guide. Third edition. Saunders Elsevier. 2015.
• Sublingual haematoma: http://www.studydroid.com/printerFriendlyViewPack.php?packId=419447
• Depressed zygomatic fracture: http://www.slideshare.net/adorabledrakheel/maxillofacial-trauma-19339123
• Dish face deformity: http://medical-gal.tumblr.com/post/93113045135/emt-monster-facial-fractures-le-fort-i
• http://www.rcemlearning.co.uk/modules/zygomatic-complex-and-nasal-injury/clinical-assessment-and-risk-stratification/general-examination/