Embed Size (px)
DESCRIPTION
case base discussion
Citation preview

Case Based Discussion
Management of Diabetes Mellitus
Dr. PMA.Ahamed
Registrar in Paediatrics
TH Kurunegala

Case History
Ama, a 10 year old schooling child was admitted with the
history of sudden onset of dizziness, fainting attack and
chest pain.
She was diagnosed with DM one year back. Had put on
MIXTARD insulin with diet control and attends regular
clinic follow-up.
Her main complaints were dizziness, abdominal pain and
vomiting. Also had severe headache.
No history of losing consciousness, had neither fever nor
urinary symptoms.
No history of recent weight loss.
Mother checks her early morning CBS REGULARLY
which usually remains above 200 mg/dl.
13-Aug-14 2

Case History Cont’d…..
No history of hypoglycemic episodes.
Does not miss her breakfast.
Takes three main meals and 2 snacks with sugar and
carbohydrate restriction.
Child’s activities compromised due to the illness but she
attends to school regularly.
Her vision and renal function were checked initially and
were normal.
She has no asthma and was not on prolonged steroid.
No family history of DM or Hypothyroidism.
Development is normal
Vaccination is up to date.
13-Aug-14 3

Case History Cont’d…..
Father runs a coconut business that generates a reasonable
income.
Mother, a house wife has a fairly good understanding of the
disease. she is aware about hypoglycemic symptoms but her
knowledge on dietary modification for insulin dose
adjustment [carbohydrate count or glycemic index] seems to
be poor.
Insulin is injecting by mother using insulin pen. she is aware
of rotating injection sites, taking correct dose and
subcutaneous administration.
School teachers and class mates are informed about her
illness.
13-Aug-14 4

Examination
Average built. Weight 30.5Kg just below 50th centile, height
140cm on 75th centile.
Looks ill, active and mildly dyspneic but no fruity odour.
Mild dehydration ++, she is not febrile.
No cataract and fundus normal.
No finger clubbing, no LJM (prayer sign)
No obvious goiter, no features of Thalassemia or Cushioned
No areas of lipodystrophy.
HR 96 and good volume, BP 100/70mmHg, No postural drop.
RR 36 lungs clear, no recession.
Abdomen soft non tender no hepatosplenomegaly,
no visible scars.
CNS GCS 15/15. peripheral sensation for touch normal.
5

Investigation
CBS 660 mg/dl
Urine
SE - Na 138, K 3.8 mmol/dL
Renal function - normal
Urine micro albumin 6mg/dL
Urine albumin/creatinin ratio - normal
UFR
U.CULTURE
FBC NAD
HbA1C 16%
13-Aug-14 6
NORMAL
ketone bodies - positive
ward test - brick red

Diagnosis DM/DKA
Diagnosis is straight forward
RBS > 200mg/dl or 11.1mmol/L
With typical symptoms
+/- ketonuria
DIFFERENTIAL DIAGNOSIS
type 2 DM in obese child
Transient hyperglycemia due to physical stress (rare)
13-Aug-14 7

13-Aug-14 8

DKA Management Goals
Correct dehydration and electrolyte imbalance
Correct hyperglycemia by insulin administration
Prevent of treatment complication
These goals are achieved by adhering to the evidence
base protocols.
13-Aug-14 9

DKA Protocol / MILUWAUKEE Protocol
Has been used for more than 20yrs in a large clinical setting
with no death no neurological sequale
A standard water deficit 85ml/kg
Mild – moderate DKA - 10- 24hrs correction
Sever DKA 30-36 hrs
Transition to oral intake and SC insulin
when DKA resolved
pCO2 >15mEq/L and pH>7.30
Normal SE
A flow sheet is mandatory for close observation.
13-Aug-14 10

Flow Sheet
13-Aug-14 11

Approach Consideration 1st hour
10-20 mL/kg IV bolus(A) 0.9% N.Saline or LR (C) *
Insulin drip(A) IV at 0.05 to 0.10 U/kg/hr(A)
NBM(E)
Monitor -In/Out put, neurologic status(E)
Mannitol at bedside[1g/kg IV for cerebral edema](C)
2nd hour until DKA resolution
0.45%NS + continue insulin drip + added K 40mmoL/l(A)
IV rate =[ SWD + maintenance – bolus ]/23hours
5% glucose if blood sugar < 250 mg/dL(14 mmol/L) (B)
If K <3 mEq/L, give 0.5 to 1.0 mmol/kg as oral K
solution OR increase IV K to 80 mmol/L(E) .
After DKA resolution
Oral intake with subcutaneous insulin(C)
12

Sample Calculation for a 30kg Child
IV rate =[SWD+ Maintenance – Bolus ]/23hours
Standard Water Deficit (SWD)
85ml/kg = 2550ml
Maintenance (24 hr)
1st 10 kg 100 mL/kg
2nd 10 kg 50 mL/kg
for all remaining kg 25 mL/kg =1750ml
1st hr = 10ml/kg IV bolus N.Saline =300mL
Then 2550+1750-300/23hrs = 175ml/hr
13-Aug-14 13

Discussion
Long Term Management - Goals Of Treatment
Control BSL [ Insulin therapy, Diet and activity]
Prevent of acute complication [hypoglycemia, DKA]
Ensuring optimum growth and development
Maintaining normal life style
Adequate education for the patient and parents
Early detection and Rx of associated disease
Reducing long term complication by maintaining good
metabolic control
Regular screening and early intervention
Provide psychological support
13-Aug-14 14

Control BSL
Insulin Therapy
Type of insulin
Dosage schedule
Monitoring
Education
Any thing new ?
13-Aug-14 15

Insulin Therapy Cont’d……
Insulin has 4 basic formulations:
Ultra ̶ short-acting ( lispro, aspart, glulisine)
Traditional short-acting ( regular, soluble)
Medium or intermediate-acting ( isophane, lente, detemir),
Long-acting ( ultralente, glargine)
13-Aug-14 16

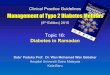
Diagrammatic Representation of Insulin Activity
13-Aug-14 17

Meals vs BSL vs Insulin level
13-Aug-14 18

Exogenous Insulin effect with time
13-Aug-14 19

Injection Regimens
Twice daily combinations of short and intermediate acting
insulin.
Multiple injection regimens using once-daily or twice-daily
injections of long-acting or intermediate-acting insulin and
short-acting insulin given at each meal
A combination of the above 2 regimens, with a morning
injection of mixed insulin, an afternoon premeal injection of
short-acting insulin and an evening injection of intermediate-
or long-acting insulin
Continuous subcutaneous insulin infusion (CSII) using an
insulin pump
CSII with close loop monitoring (external pancreas)
13-Aug-14 20

13-Aug-14 21

Dose Depending on the pubertal stage;
0.7 u/kg/day in pre pubertal
1.0 u/kg/day at mid puberty
1.2 u/kg/day by the end of puberty
Newly diagnosed; 60-70% of above values due to residual β
cell function (honey moon period)
1/3 long acting of total insulin
2/3 short acting ( 3 divided dose for each meals)
Insulin schedule should be adjusted to optimal BS control
Frequent self monitoring of BS and dose adjustment
paramount
Storage and supply of insulin should be discuss properly
13-Aug-14 22

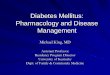
Continuous subcutaneous insulin infusion (CSII) –
Rapid-acting insulin infused continuously 24 hours a day
through an insulin pump at 1 or more basal rates, with
additional boluses given before each meal and correction
doses administered if blood glucose levels exceed target
levels
Bionic pancreas or CSII with close loop monitoring
Pancreas and islet cell transplantation
Technically demanding and rejection are limiting factors
Regeneration of islet cells
1.In vitro by using embryonic stem cells
2.Ex vivo by using bone marrow stem cells differentiate to β cell
in vitro
3.In vivo regeneration therapy
23

13-Aug-14 24
CSII
BIONIC
PANCREAS

Injection Phobia
Alternatives to injecting insulin have been constantly
sought
Oral insulin research: expensive but promising
Many major pharmaceutical companies are at the
research and development stage of following
Pre meal oral insulin (oralin)
Delayed-absorption capsules
Oral sprays
Inhaled form of insulin (Exubera)
Sublingual lozenges
13-Aug-14 25

Diet
Dietary management is an essential component.
Aim of dietary management
No strict diet restriction.
Dietary recommendations should take into account the
patient’s eating habits and lifestyle.
A daily caloric intake prescription should balance the
child's food intake with insulin dose and activity.
Keep blood glucose concentrations as close as possible
Avoiding extremes of hyperglycemia and hypoglycemia
Recommendations for amounts of dietary carbohydrate,
fat, and protein.
13-Aug-14 26

Diet Cont’d……
Carbohydrates - 50-55% of daily energy intake; no more
than 10% of carbohydrates should be from sucrose or other
refined carbohydrates
Fat - Should provide 30-35% of daily energy intake
Protein - Should provide 10-15% of daily energy intake
Instructions on how to divide calories between meals and
snacks
20% for breakfast
35% for lunch
30% for dinner
15% for snack
13-Aug-14 27

Dietary Freedom
Carbohydrate counting
The ability to estimate the carbohydrate content of food
The dietitian should develop a diet plan for each child to suit
individual needs and circumstances.
The number of carbohydrates in a food can be determined
by reading the nutrition label, consulting a reference book
or website, carrying a database on a personal digital
assistant (PDA)
Exchange planning
All foods are categorized as either a carbohydrate, meat or
meat substitute, or fat.
In this system, one serving of a carbohydrate (eg, one small
apple can be exchanged for any other carbohydrate
(eg, 1/3 cup cooked pasta) 28

Activity
No restrictions on activity
Exercise has real benefits
Educate the patients about the effects of exercise on the
blood glucose level.
Should check blood sugar level before and after exercising
Adjusting insulin dose for exercise
Make sure to maintain their hydration status during
exercise
Avoiding excessive weight gain or weight loss
Early detection of hypoglycemic symptoms
13-Aug-14 29

Monitoring
self-monitoring of blood glucose levels(SMBG)
A minimum of 4 daily BS should be measured for Optimal
diabetic control
requires frequent Monitoring when hypoglycemia
inter current illness, dietary changes and unusual
physical activity
Availability of glucometer /strips and cost are limiting
factors
Continuous glucose monitors (CGMs) /RT-CGM
contain subcutaneous sensors that measure interstitial
glucose levels every 1-5 minutes, providing alarms when
glucose levels are too high or too low or are rapidly rising
or falling.
HbA1c level
30

Target BSL and HbA1C
Age (year)
Pre meal BSL
( mg/dL)
HbA1C(%)
<5
100 -200
7.5 - 9
5 - 11
80 - 150
6.5 - 8
12 - 15
80 - 130
6 - 7.5
18 <
70 - 120
5.5 - 7
13-Aug-14 31

Somagi Phenomenon
Rebound hyperglycemia in early morning after an incident
of hypoglycemia this rebound is secondary to the release
of counter regulatory hormones
Commonly reported more frequently at night due to
unrecognized and untreated hypoglycemia when as sleep
So evening dose of insulin should be reduced
Dawn phenomenon Rise in blood sugar in the early morning hours due to low
insulin level
So the dose of insulin should be increased or change to
long acting
13-Aug-14 32

Parent and Patient Education
About disease and importance of follow-up
Recognition of hypoglycemia and initial management
Blood glucose monitoring
Insulin therapy
Healthy eating habits
Physical activity
Dealing with ups and downs of illness
Keeping communication and getting information
Coping styles and support groups 33

Where to find reliable health information?
National Library of Medicine
(www.nlm.nih.gov/medlineplus/healthtopics.html)
National Institute of Diabetes & Digestive & Kidney Diseases
(www.niddk.nih.gov)
American Diabetes Association (ADA)
(www.diabetes.org)
The Endocrine Society
(www.endo-society.org)
Hormone Health Network
(www.hormone.org/diseases-and-conditions/diabetes)
Local Diabetic Clinics
13-Aug-14 34

Long Term Monitoring and Follow-up
Growth assessment
Injection site examination
Evaluation for signs of associated autoimmune disease
Blood pressure
Retinal screening, Retinoscopy or Fundal photography
Urine examination for microalbuminuria and nephropathy
Neuropathy screening and foot care
Macro vascular complication
35

Screening Guidelines
When Frequency Preferred Screening Method
Retinopathy After 5yr PPC
After 2yr PC 1-2 yearly Fundal photography
Nephropathy After 5yr PPC
After 2yr PC annually Overnight timed urine albumin
Neuropathy - - Physical exam
Macrovasc. After 2yr Every 5 yr lipids
Thyroid At diagnosis Every 2-3yr TSH
Celiac At diagnosis Every2-3yr Tissu transglutaminase, endomysial ab

Can We Prevent Type I Diabetes ???
13-Aug-14 37
Viral Infection
CRS
?mumps
Early exposure to gluten
Cows milk/formula
Hygienic hypothesis
Breast feeding
Psychological stress
Omega3, Vit C/D/E, Zn
(TEDDY study)
MHC/HLA Types
CTLA 4
Interleukin receptor

Summary
Pathophysiolgy of type 1 DM
Treatment of DKA
Long term management of DM
Advances in the management
Monitoring and follow-up
13-Aug-14 38

0
5
10
15
20
25
30
35 01-05-02
01-06-02
01-07-02 01-08-02
01-09-02
Series 1
Series 2
Any ?
13-Aug-14 39

13-Aug-14 40