Embed Size (px)
Citation preview

Management of Ankle Injuries
Dr Umar M AminuOrthopaedics Unit
Surgery DepartmentATBUTH
Outline• Introduction• Epidemiology• Anatomy• Assessment of Ankle Injury• Differential Diagnoses• Initial Management• Ankle Sprains
» Classification» Treatment» Prevention
• Ankle Fractures» Classification» Treatment
• Ankle Arthrodesis• Prognosis• Conclusion

Introduction
• An important cause of morbidity in primary care emergency medicine and sports medicine
• Range from ligamentous sprain to severe fracture dislocation with disruption of the joint
• Obvious clinical deformity or injuries with neurovascular compromise of the foot are orthopaedic emergencies

Epidemiology• Ankle fractures are the most common of all fractures treated
in hospitals (Yang et al, 2011)) • in the US with an incidence of ankle,tibial and fibular
fractures 492,000 per year(Praemeret al., 1992; Weening and Bhandari, 2005)
• RTA accounts for 46.3% in Nigeria (Ifesanya and Alonge, (2012)) and 71.5% in Rwanda (Twagirayezu et al., 2008)
• 30.2% of injuries among squash players in Nigeria (Owoeye OBA et al, 2013)
• 24.1% of injuries among professional Nigerian Basket ball players (Talabi, A E,)
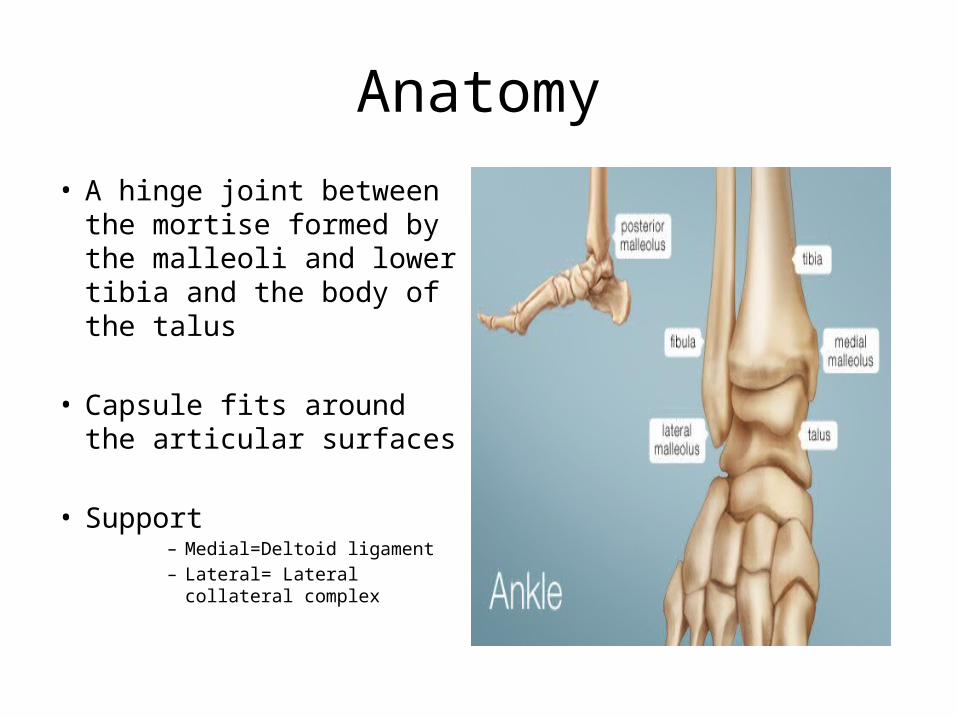
Anatomy• A hinge joint between the
mortise formed by the malleoli and lower tibia and the body of the talus
• Capsule fits around the articular surfaces
• Support– Medial=Deltoid ligament– Lateral= Lateral collateral
complex

Anatomy(cont’d)

Assessment of Ankle Injuries
History• Duration of injury• Mechanism of injury• Site of Pain• Ability to bear weight, walk or continue playing• Previous ankle injury• Past medical history• Drug history

Assessment of Ankle Injury(cont’d)
• Examination• Inspection
» Ability to bear weight» Deformity» Swelling/bruising» Effusion» Open wounds
• Palpation» Crepitus and tenderness
Assessment of Ankle Injury(cont’d)
• Examination (cont’d)• Examination for Neurovascular Injury
» Sensation» Capillary refill» Distal pulses
• Movement /power-• Coexisting injuries
» Ipsilateral knee and foot» Proximat tibial #
Assessment of Ankle Injury(cont’d)
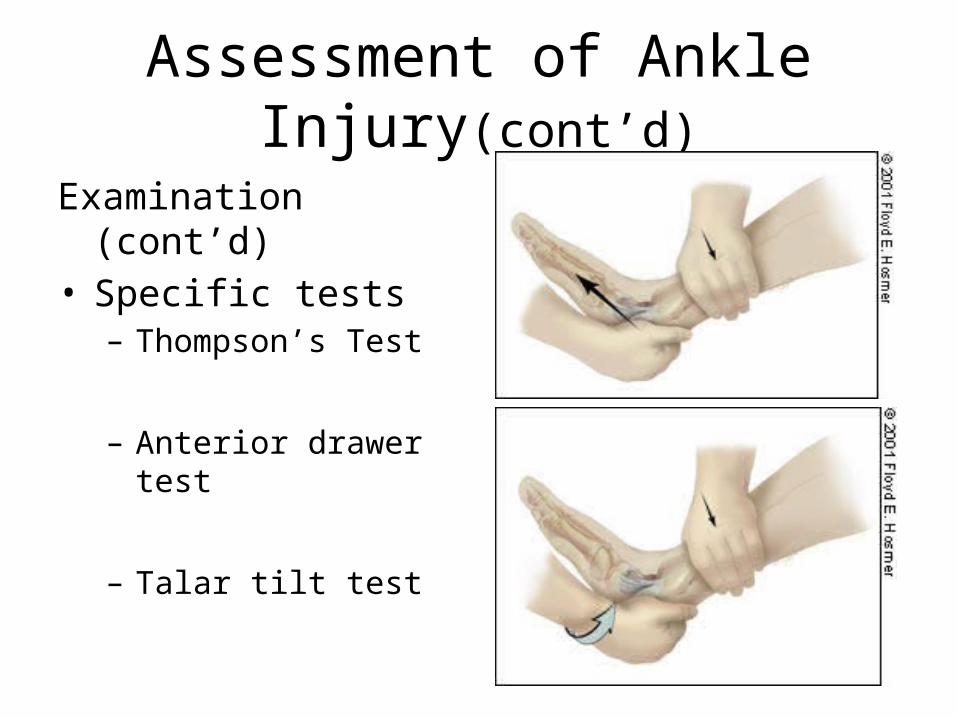
Examination (cont’d)• Specific tests– Thompson’s Test
– Anterior drawer test
– Talar tilt test
Assessment of Ankle Injury(cont’d)
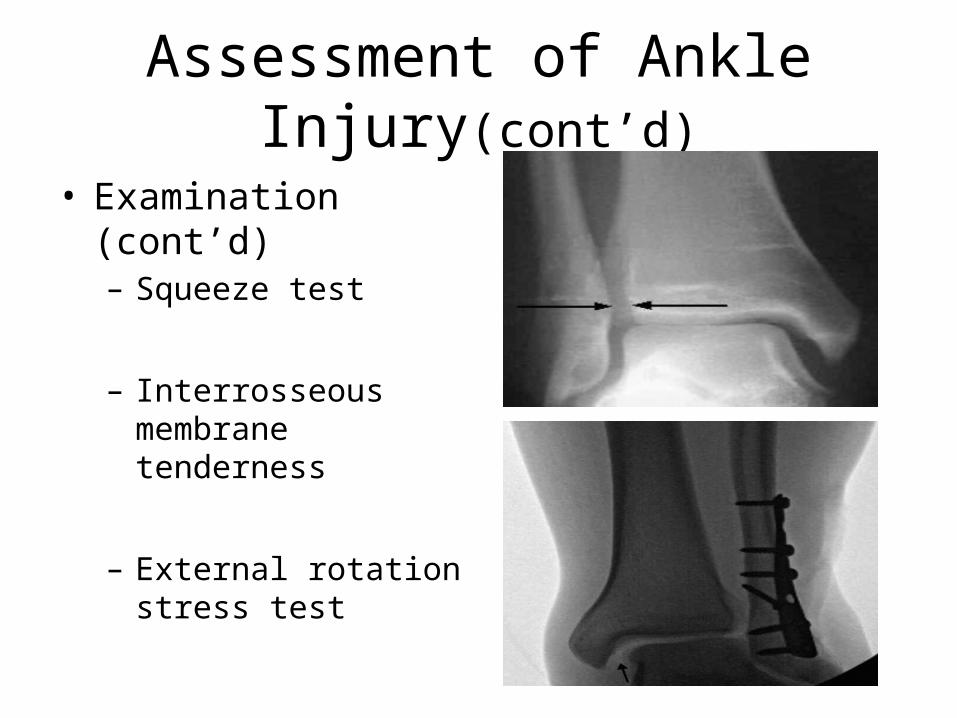
• Examination (cont’d)– Squeeze test
– Interrosseous membrane tenderness
– External rotation stress test

Assessment of Ankle Injury(cont’d)
Investigations• Imaging
• X-ray –• AP• Lateral• Mortise view
• CT and MRI•Guided by Ottawa rule
Assessment of Ankle Injury(cont’d)
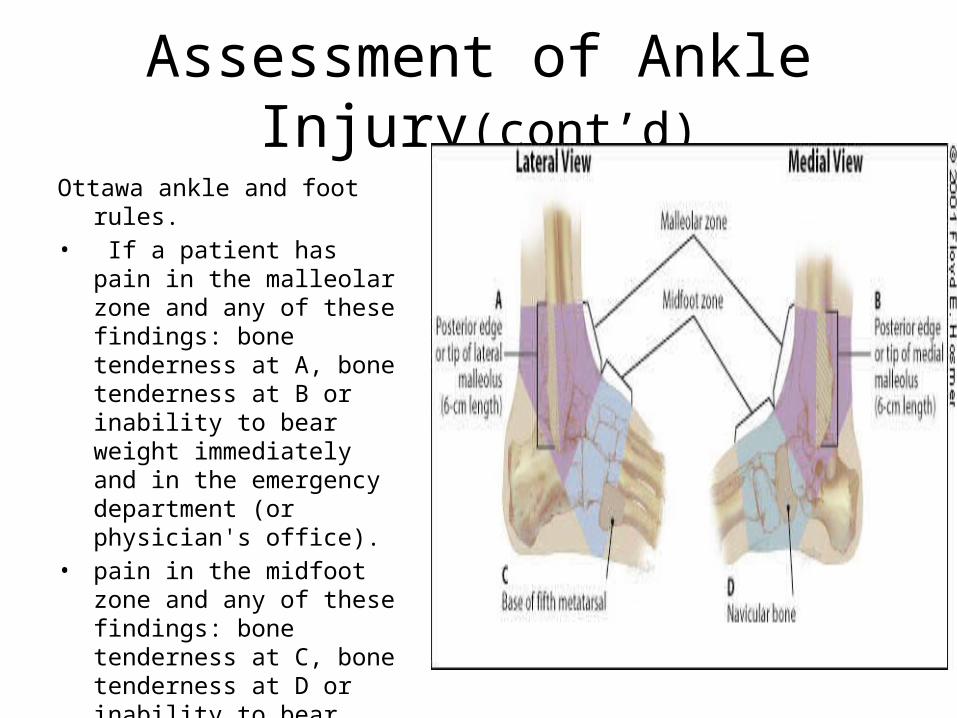
Ottawa ankle and foot rules.• If a patient has pain in the
malleolar zone and any of these findings: bone tenderness at A, bone tenderness at B or inability to bear weight immediately and in the emergency department (or physician's office).
• pain in the midfoot zone and any of these findings: bone tenderness at C, bone tenderness at D or inability to bear weight immediately and in the emergency department (or physician's office).

Differential Diagnoses
• Ligamentous injury-Sprain
• Bony injury- Fracture
• Tendinous injury- Strain
• Others- gout,

Initial Management
• Resuscitation
• Neurovascular compromise obvious deformity or # should be reduced –before x-ray under analgesia and sedation

Ankle Sprains
• The most common musculoskeletal injuries
• Lateral collateral complex most commonly affected
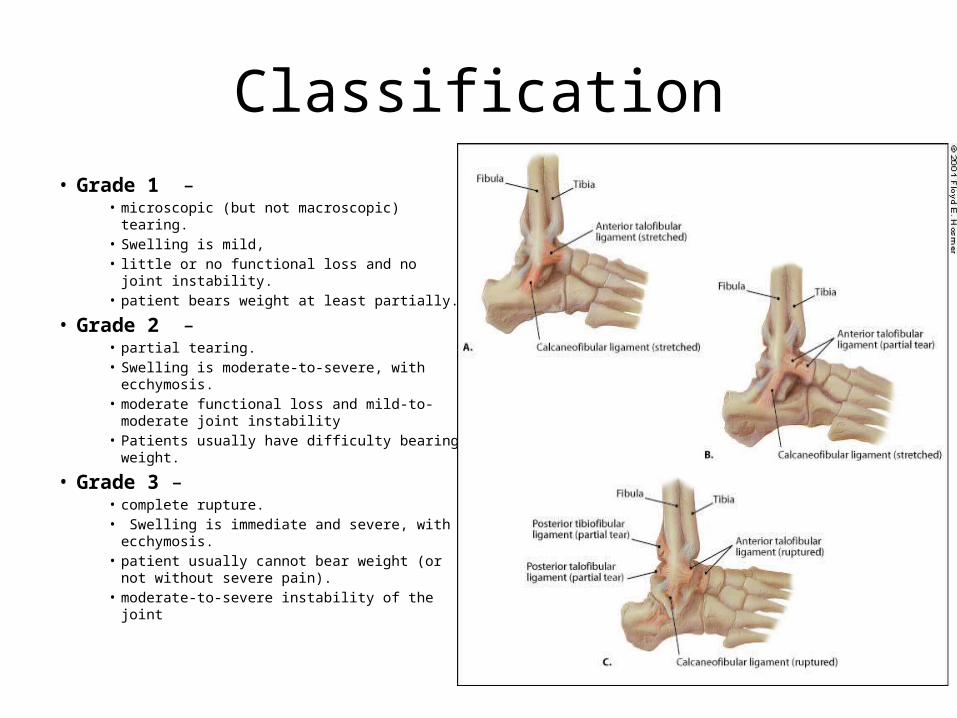
Classification• Grade 1 –
• microscopic (but not macroscopic) tearing. • Swelling is mild, • little or no functional loss and no joint
instability. • patient bears weight at least partially.
• Grade 2 –• partial tearing. • Swelling is moderate-to-severe, with
ecchymosis.• moderate functional loss and mild-to-
moderate joint instability• Patients usually have difficulty bearing weight.
• Grade 3 –• complete rupture.• Swelling is immediate and severe, with
ecchymosis. • patient usually cannot bear weight (or not
without severe pain). • moderate-to-severe instability of the joint
Treatment
• Protection – • protect the injured area from further injury)
• Rest –• stop the activity that caused the injury • rest for the first 48 to 72
• Ice –• for the first 48 to 72 hours after the injury, • apply ice wrapped in a damp towel to the injured area for 15 to 20
minutes every two to three hours during the day.• Do not leave the ice on while you are asleep, and do not allow the
ice to touch your skin directly, because it could cause a cold burn.
Treatment(cont’d)
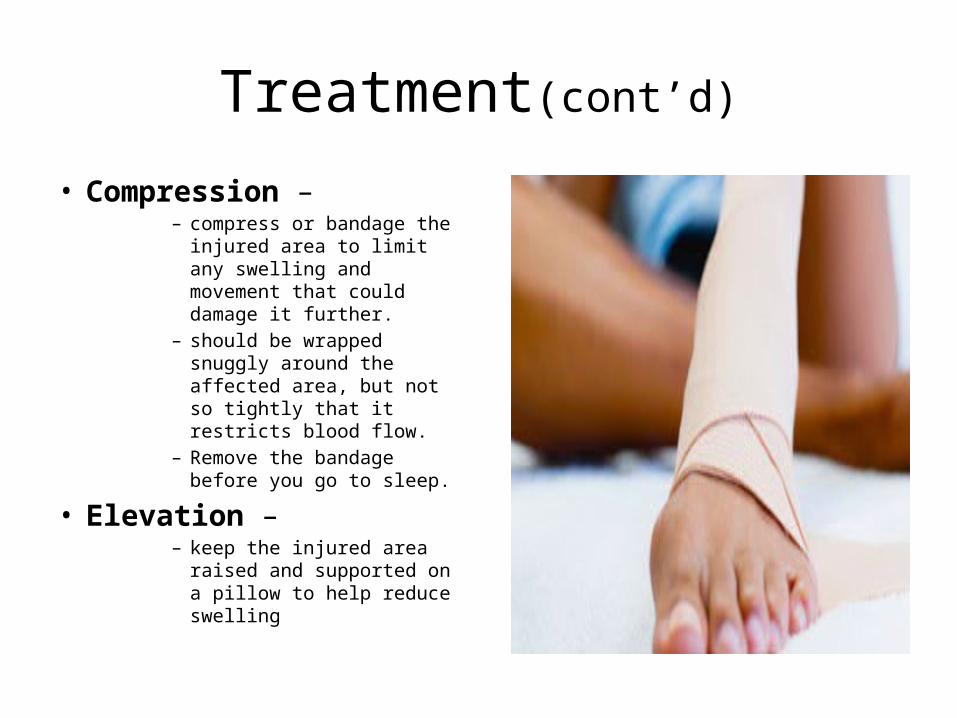
• Compression – – compress or bandage the
injured area to limit any swelling and movement that could damage it further.
– should be wrapped snuggly around the affected area, but not so tightly that it restricts blood flow.
– Remove the bandage before you go to sleep.
• Elevation – – keep the injured area raised
and supported on a pillow to help reduce swelling
Treatment (cont’d)
Avoid HARM in 1st 24hrs-• Heat – such as hot baths, saunas or heat packs. • Alcohol – drinking alcohol will increase bleeding
and swelling, and slow healing. • Running – or any other form of exercise that
could cause more damage. • Massage – which may increase bleeding and
swelling.
Treatment (cont’d)
Treat Pain• Systemic/topicalRehabilitation• Important to build up
muscle around ankle• Supervised exercises may
provide some benefit for recovery
• Athlete with severe sprains may need orthosis for several months after injury
Treatment (cont’d)
Surgery-• usually only required for severe muscle strains,
particularly those in professional sports people. • For non-sports professionals and those with
more minor strains, the loss of muscle strength is usually too mild, or the risk of repeated injuries too low, to justify the risks of surgery.
Prevention
• Appropriate foot wear for hiking over hills or uneven ground of for manual labour

Ankle Fractures
• May involve:• distal tibia, • distal fibular , • talus or• calcaneous
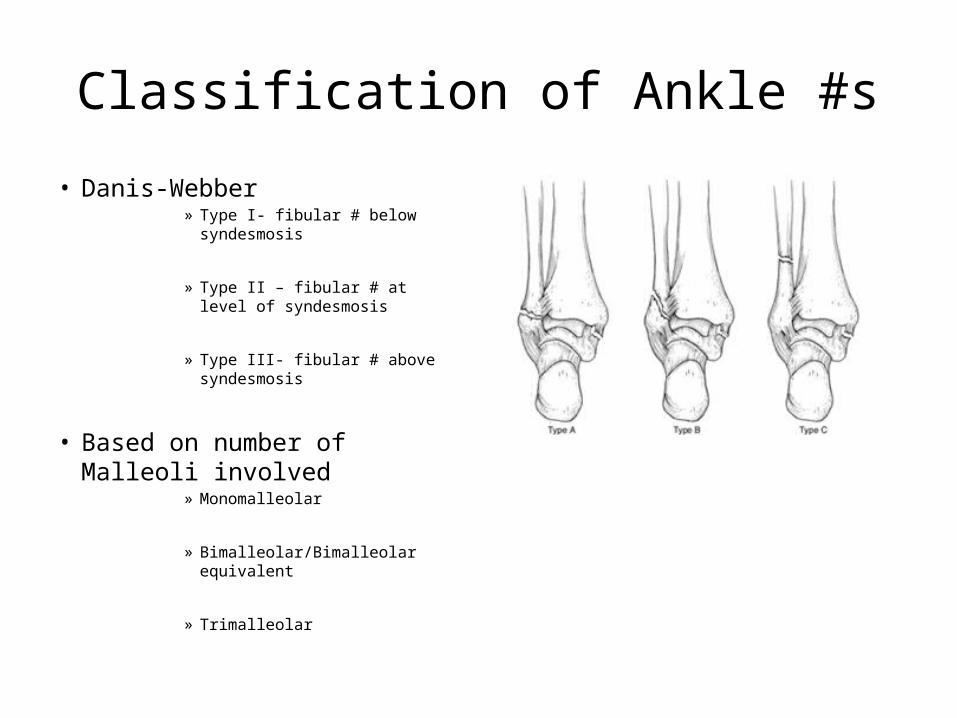
Classification of Ankle #s• Danis-Webber
» Type I- fibular # below syndesmosis
» Type II – fibular # at level of syndesmosis
» Type III- fibular # above syndesmosis
• Based on number of Malleoli involved
» Monomalleolar
» Bimalleolar/Bimalleolar equivalent
» Trimalleolar

Classification of Ankle #s (cont’d)

Classification of Ankle #s (cont’d)Named Fractures
• Snowboarded’s # • Maisonneuve #
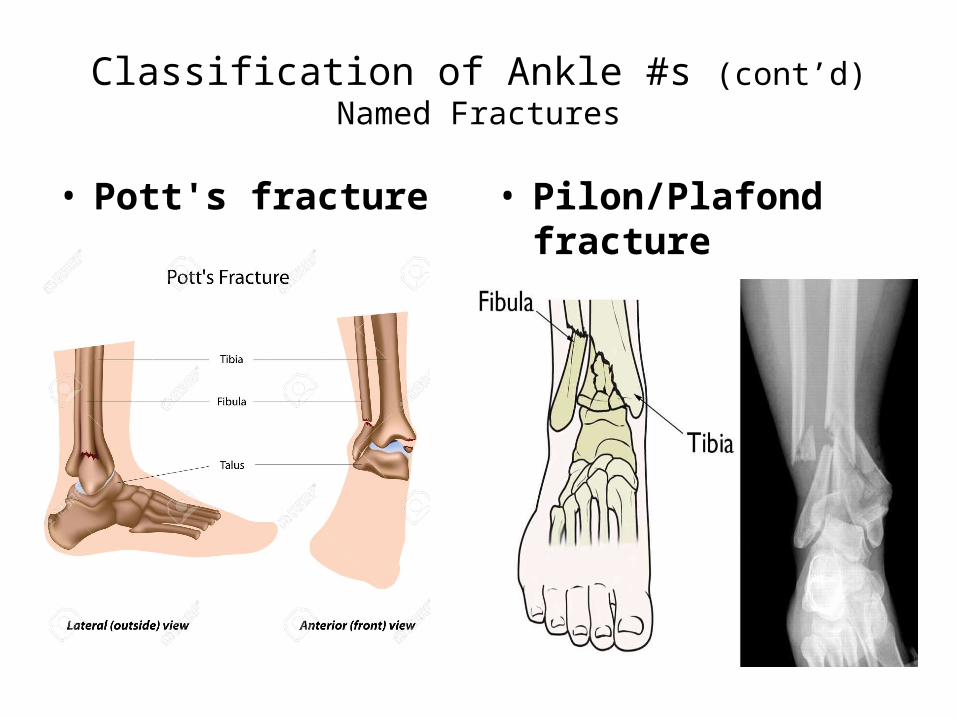
Classification of Ankle #s (cont’d)Named Fractures
• Pott's fracture • Pilon/Plafond fracture
Treatment
• Initial Treatment• Resusitation
» ‘ABCDE’ principles of Trauma
• Neurovascular compromise or dislocation immediately reduced
• Open fractures covered with wet, sterile dressing secured with looosely wraped dry sterile gauze
• Analgesia
Treatment(cont’d)
• Secondary survey
• Stablise # with backslab
• Elavate limb

Treatment(cont’d)
Definitive Treatment• Consider whether the fracture is stable or unstable.
Unstable ankle fractures include:» Fracture dislocation.» Bimalleolar or trimalleolar fractures.» Any lateral malleolar fracture with substantial talar shift.
• aim to reduce the fracture, maintain reduction, promote healing and restore function.
• can be achieved both conservatively and operatively.

Treatment(cont’d)
Conservative treatment• For:– Non-displaced fractures or anatomically reduced
fractures - although functional outcome may be better if treated operatively.
– Patients with serious comorbidities who are not fit for surgery.
Treatment-Conservative (cont’d)
• cast for 4-6 weeks - following this, weight-bearing can be resumed.
• Serial radiographs to ensure the reduction, joint congruity and healing are maintained
• Consider operative treatment if the fracture fails to heal or displaces.

Treatment(cont’d)
Operative treatment• For:– Displaced unstable fractures.– Talar subluxation.– Joint incongruity.– Bimalleolar or trimalleolar fractures - >25-30%
involvement of the plafond or >2 mm step off.– Syndesmotic disruption:
» Weber C fractures; some Weber B fractures.» Tibiofibular clear space of ≥6 mm on anteroposterior radiography.
Complications
Early• Infection.• Compartment
symdrome.• Vascular compromise
and foot ischemia
Late• DVT(secondary to immobilisation).• Fracture non-union and malunion.• Poor wound healing• Osteoarthritis (especially talus
fractures).• Reduced movement at the ankle
(calcaneal fractures can compromise inversion and eversion).
• Ankle fractures involving the growth plate in children can lead to deformity and growth disturbance.

Ankle Arthrodesis
• for treatment of tibiotalar arthrosis
• results in freedom from pain and nearly normal walking ability
• other options, such as total ankle replacement, have been less viable

Ankle Arthrodesis(cont’d)
• The indications -– degenerative arthrosis,– rheumatoid arthritis– posttraumatic arthritis,– avascular necrosis of the talus– neurologic disease resulting in an unstable ankle,– neuropathic ankle joint.
• The relative contraindications include degenerative joint disease in the subtalar and midtarsal joints.
Ankle Arthrodesis(cont’d)
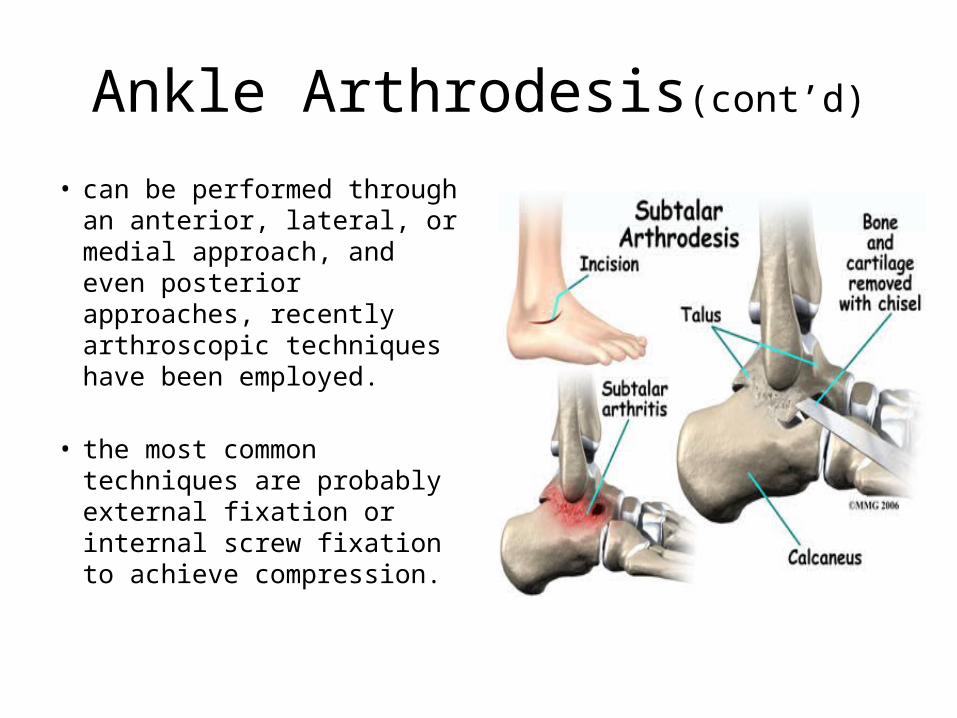
• can be performed through an anterior, lateral, or medial approach, and even posterior approaches, recently arthroscopic techniques have been employed.
• the most common techniques are probably external fixation or internal screw fixation to achieve compression.
Conclusion
• Ankle injuries very in cause, and complexity and so does their management and a proper understanding of this is necessary for their proper management .

THANK YOU FOR LISTENING