Embed Size (px)
Citation preview
MALARIAOp. Dr. Kivanc KAYHAN
Obs & Gyn


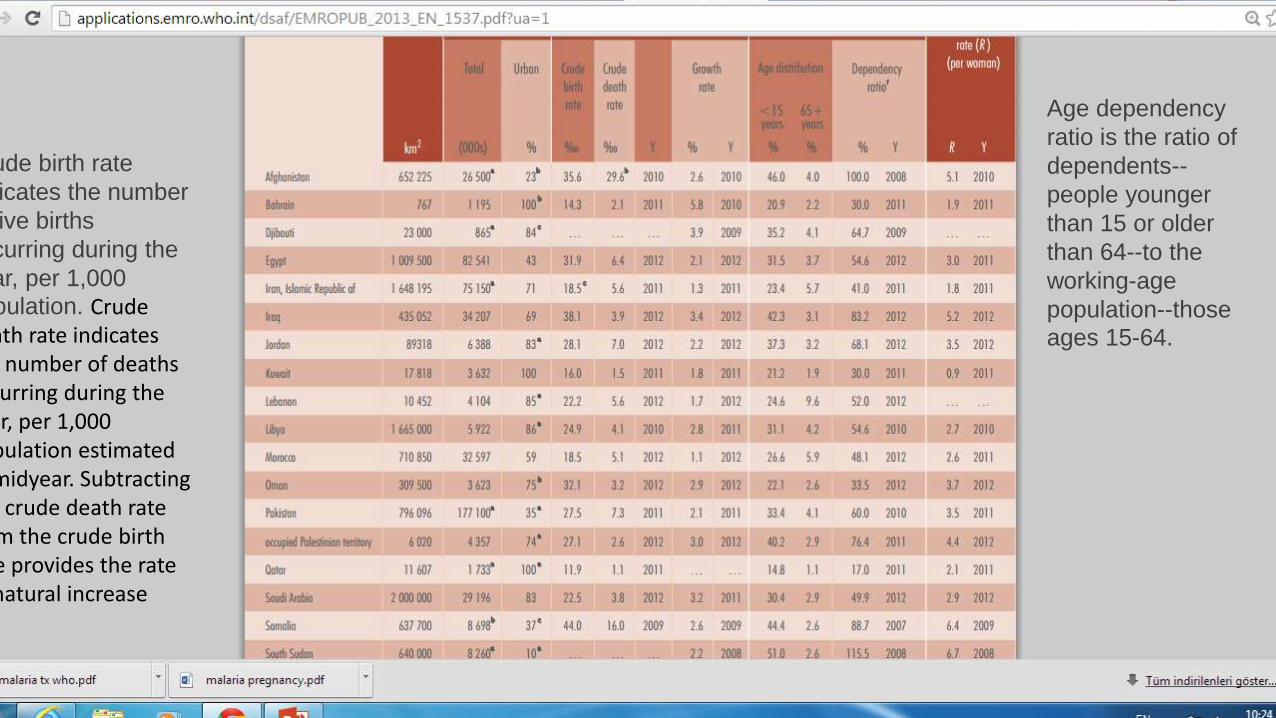
Crude birth rate
indicates the number
of live births
occurring during the
year, per 1,000
population. Crude death rate indicates the number of deaths occurring during the year, per 1,000 population estimated at midyear. Subtracting the crude death rate from the crude birth rate provides the rate of natural increase
Age dependency
ratio is the ratio of
dependents--
people younger
than 15 or older
than 64--to the
working-age
population--those
ages 15-64.
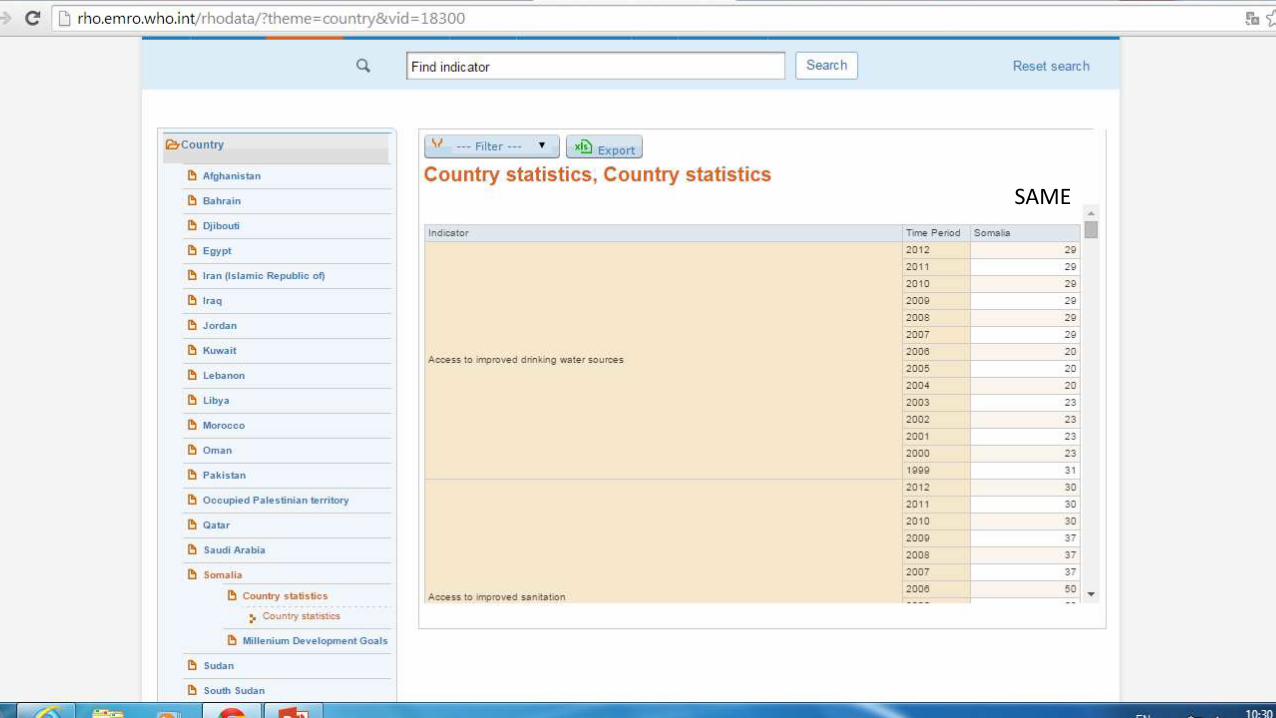
SAME
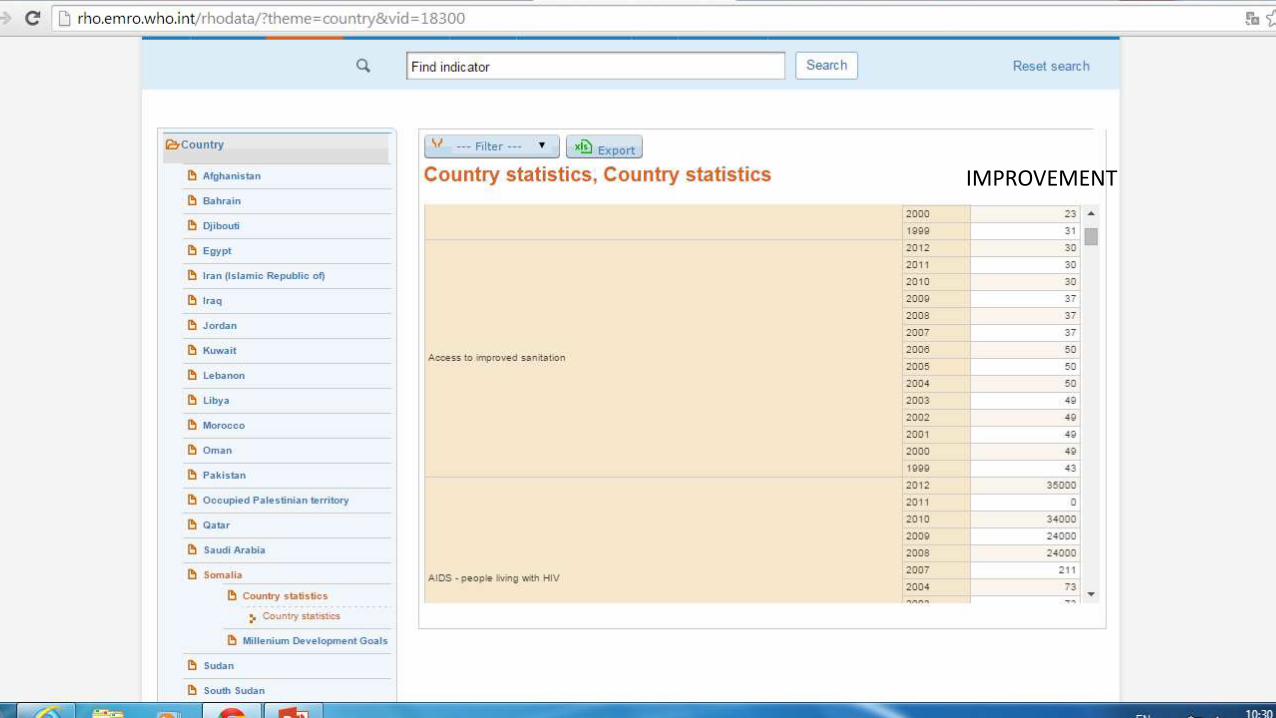
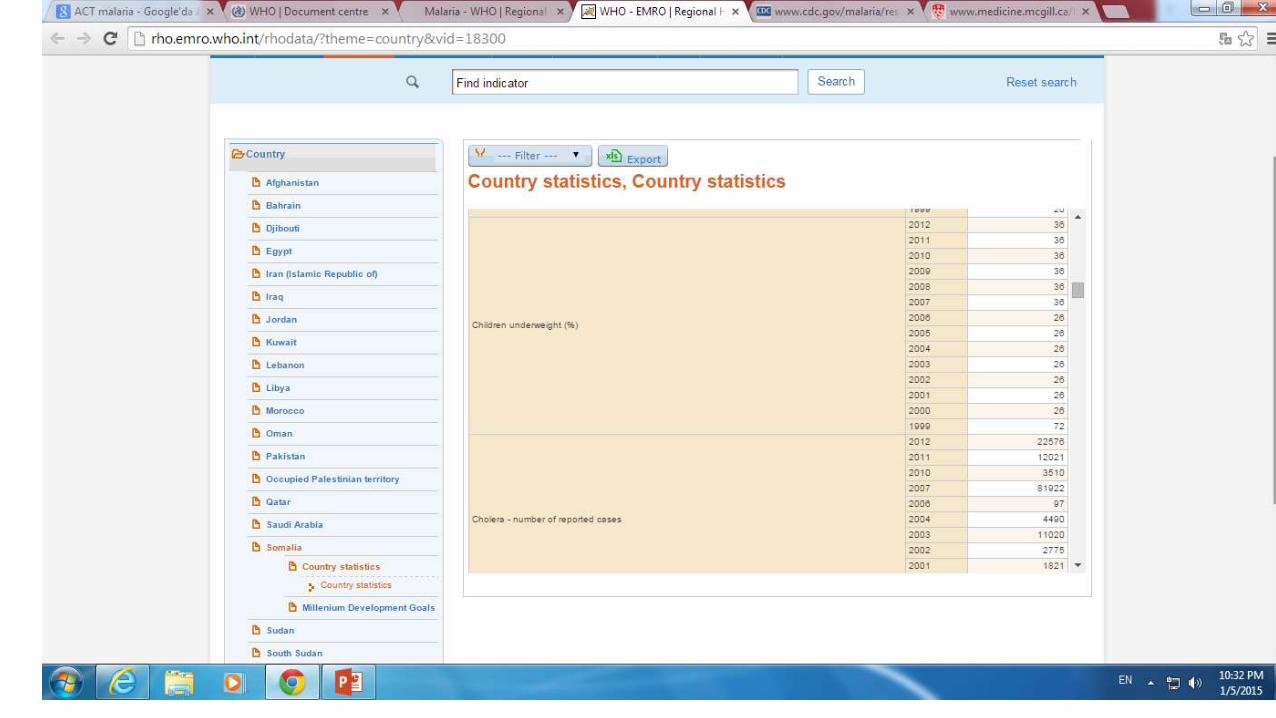
IMPROVEMENT
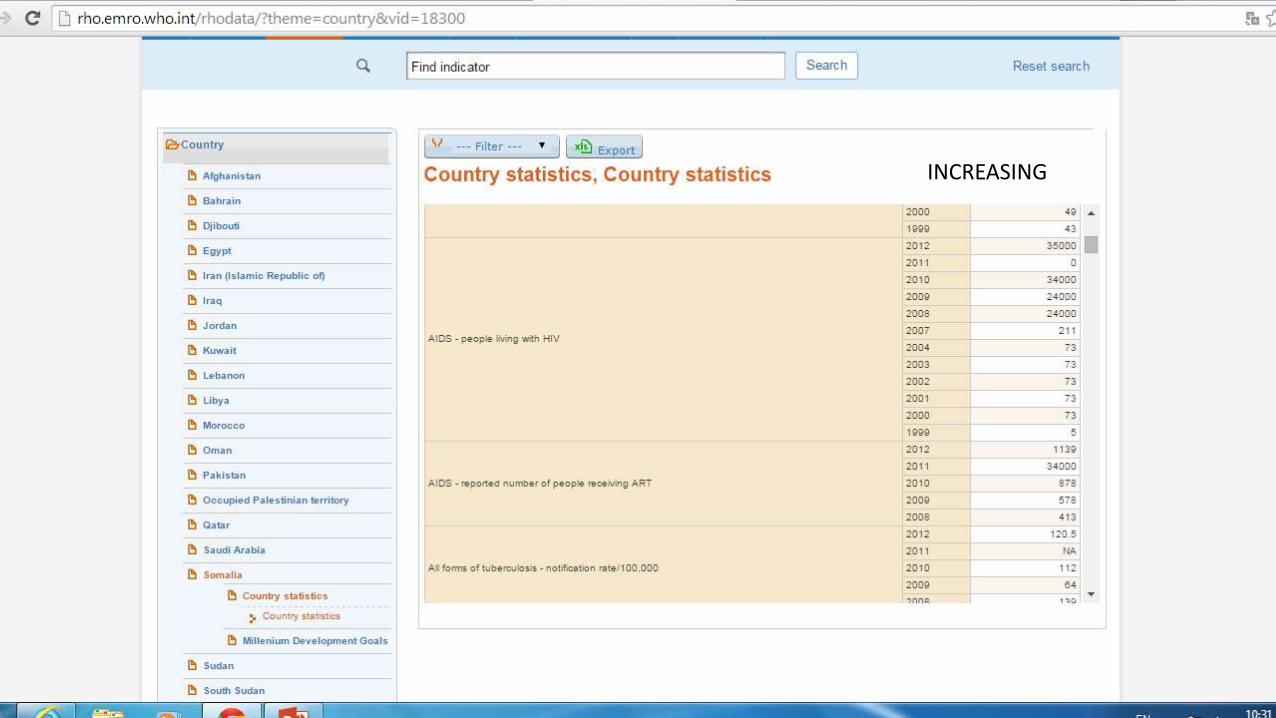
INCREASING
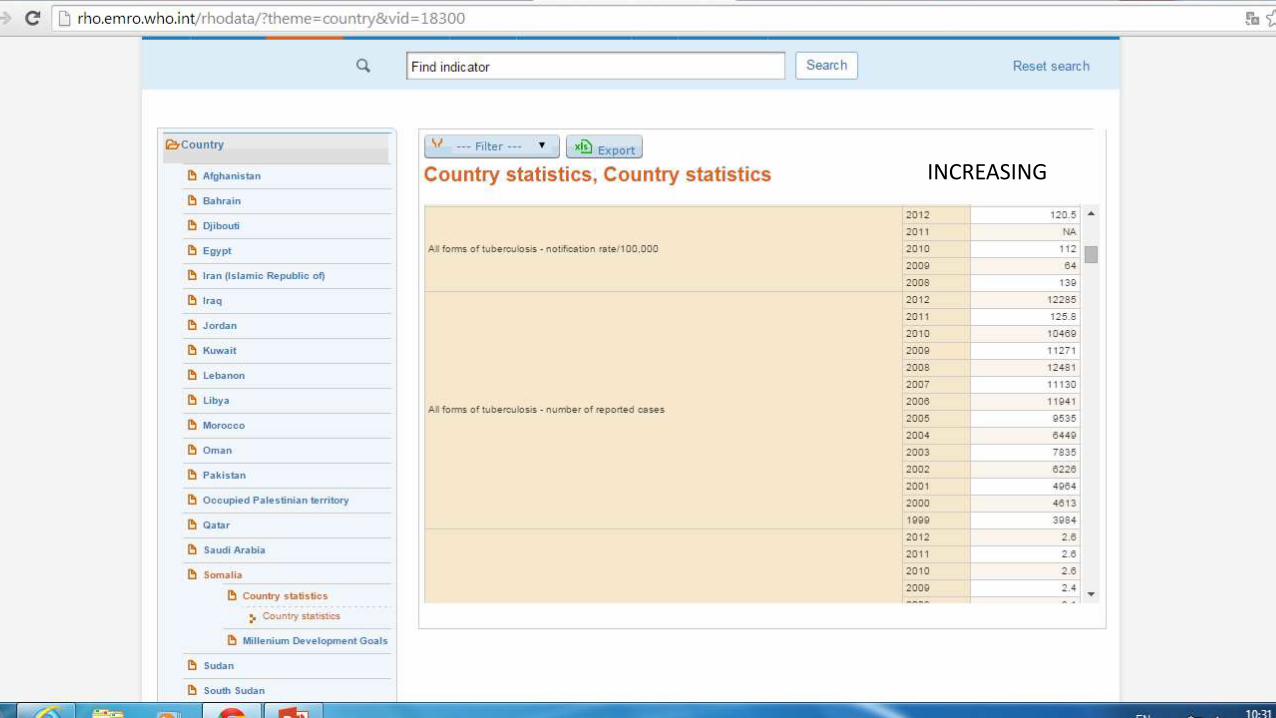
INCREASING

SAME
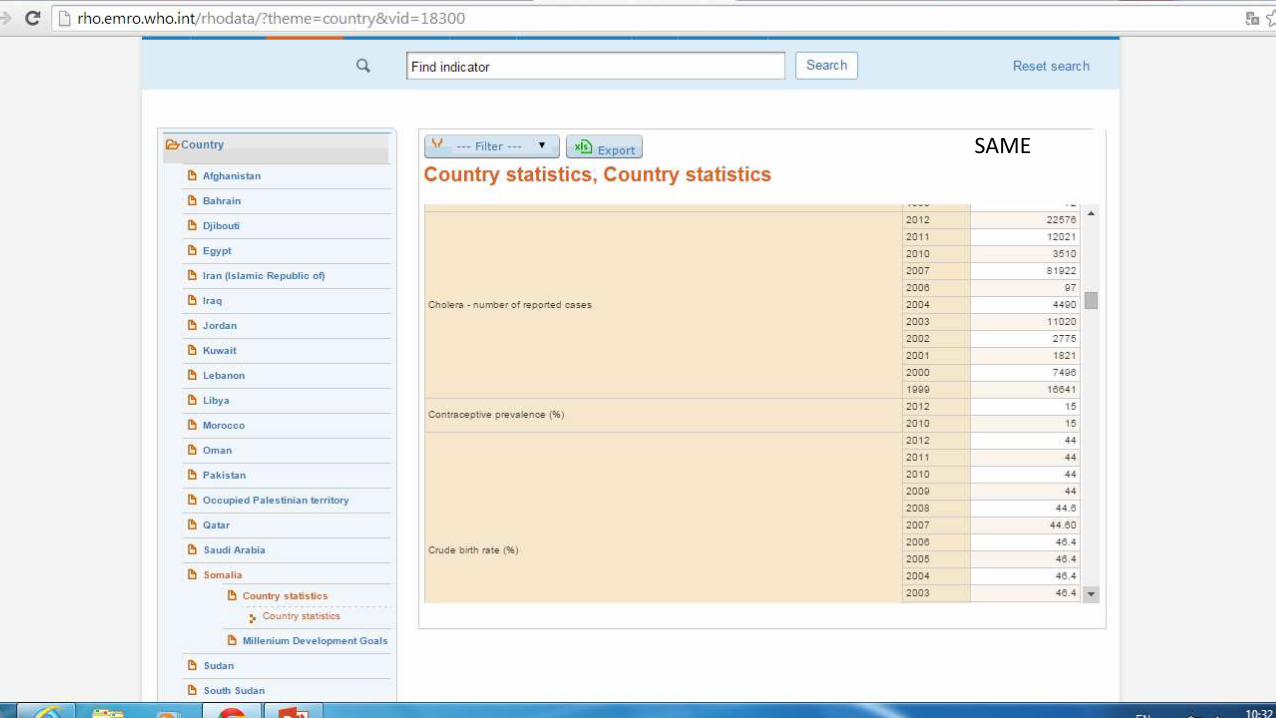
SAME
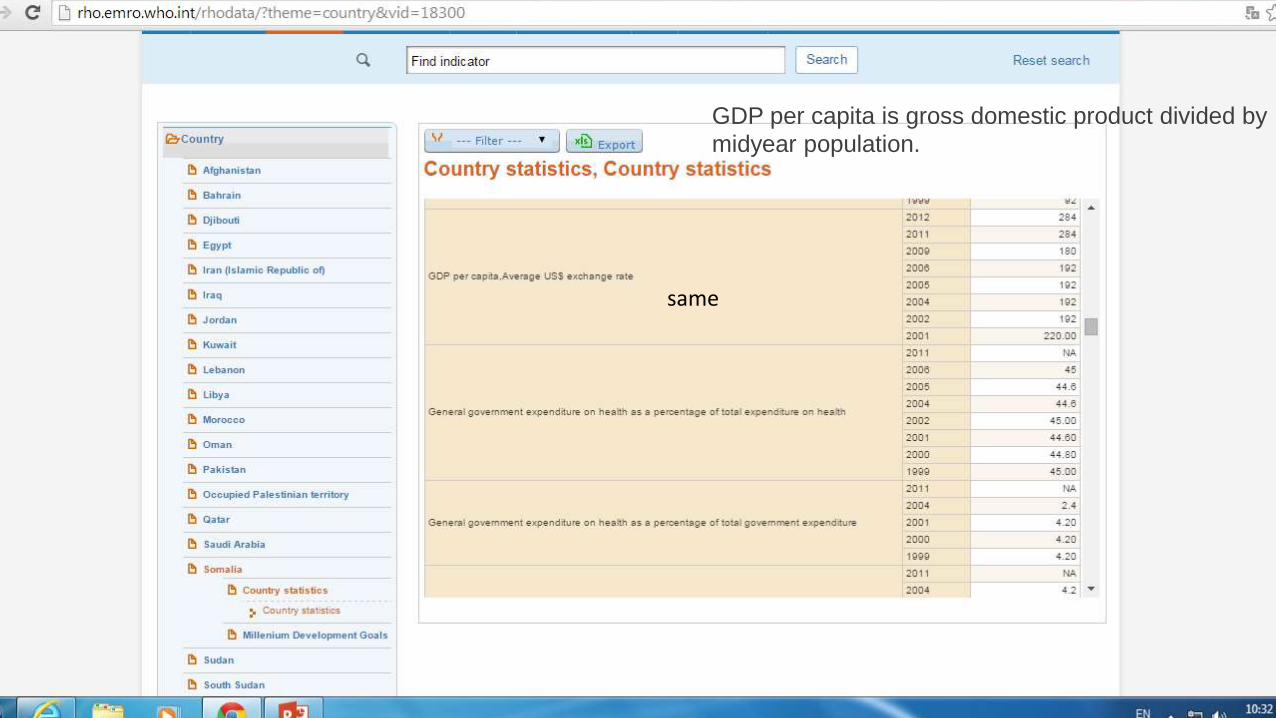
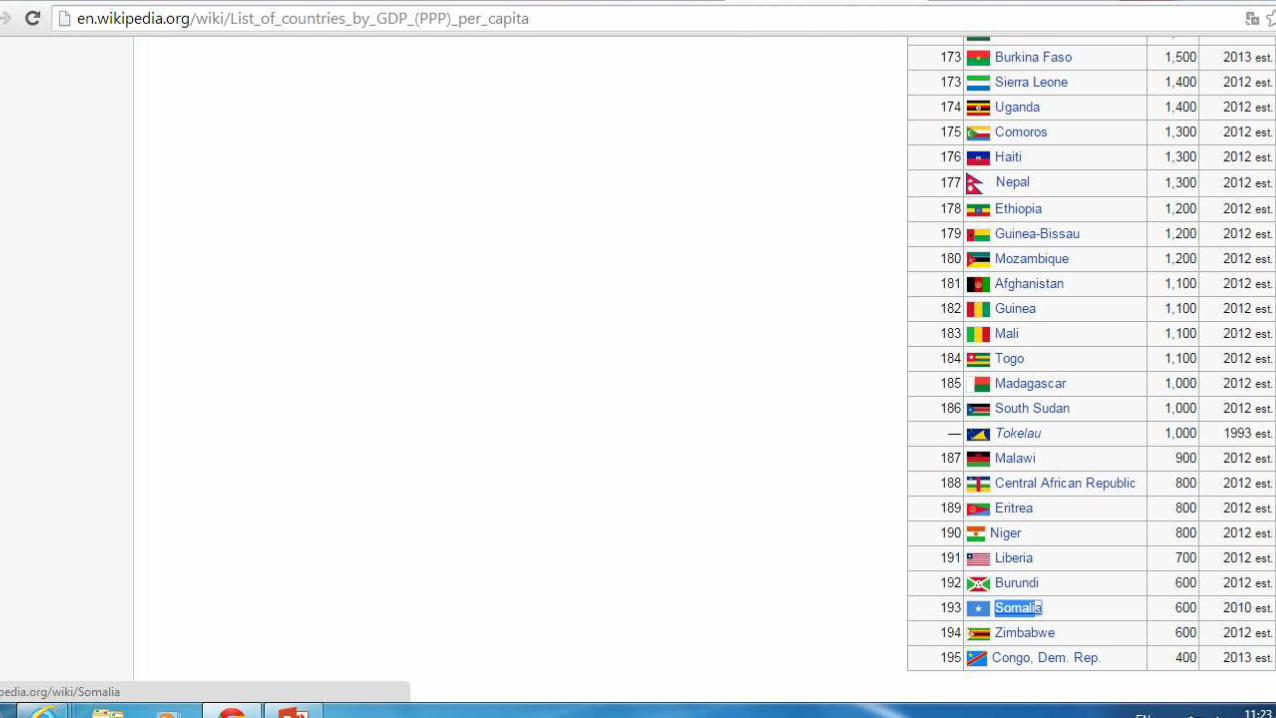
GDP per capita is gross domestic product divided by
midyear population.
same

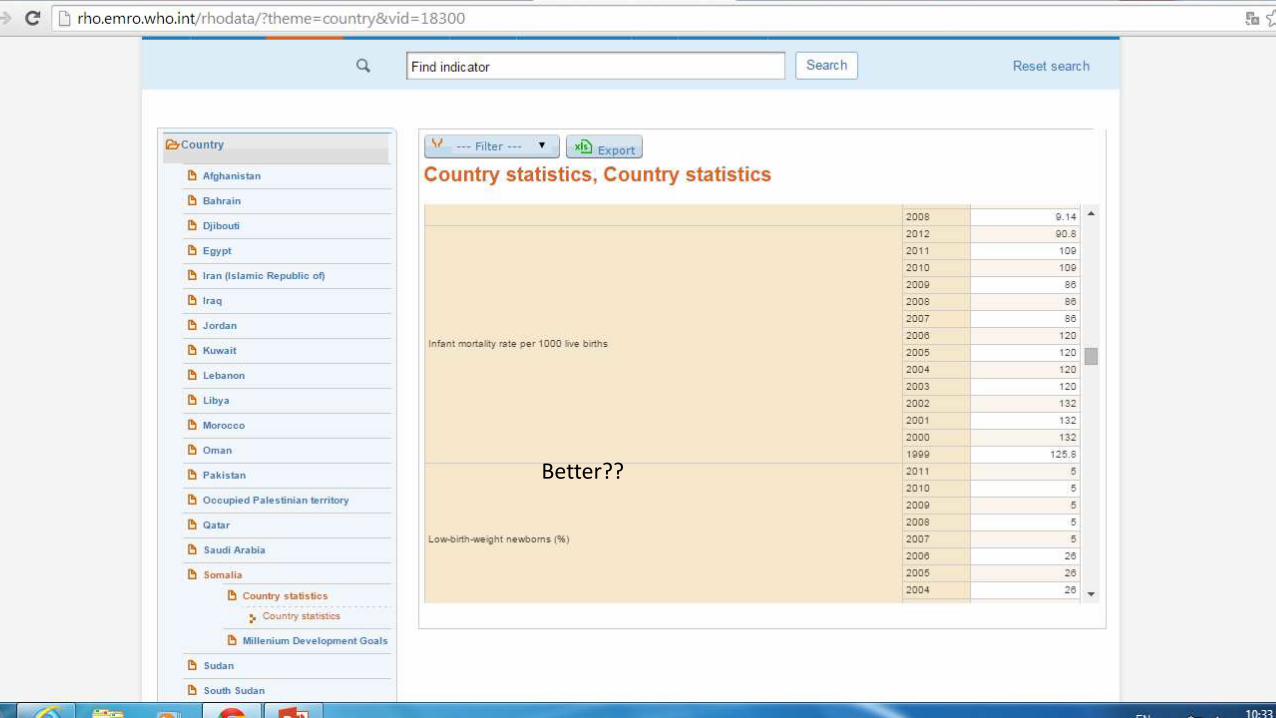
Better??
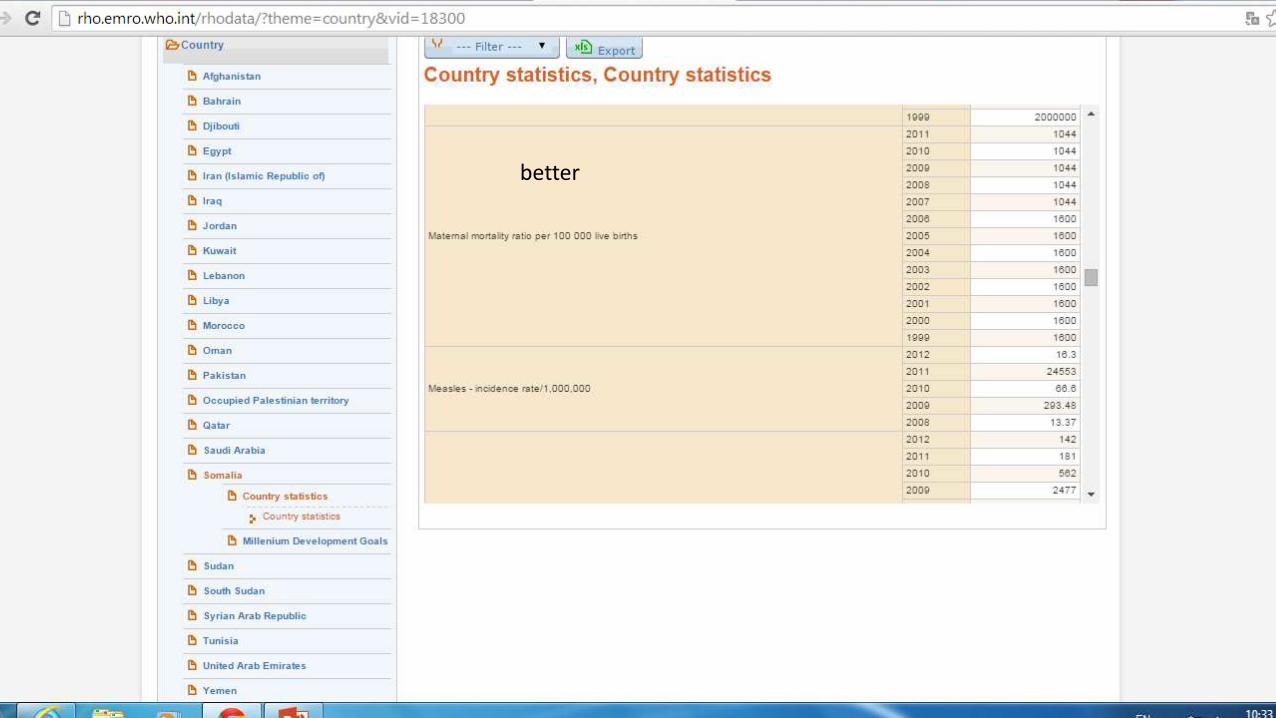
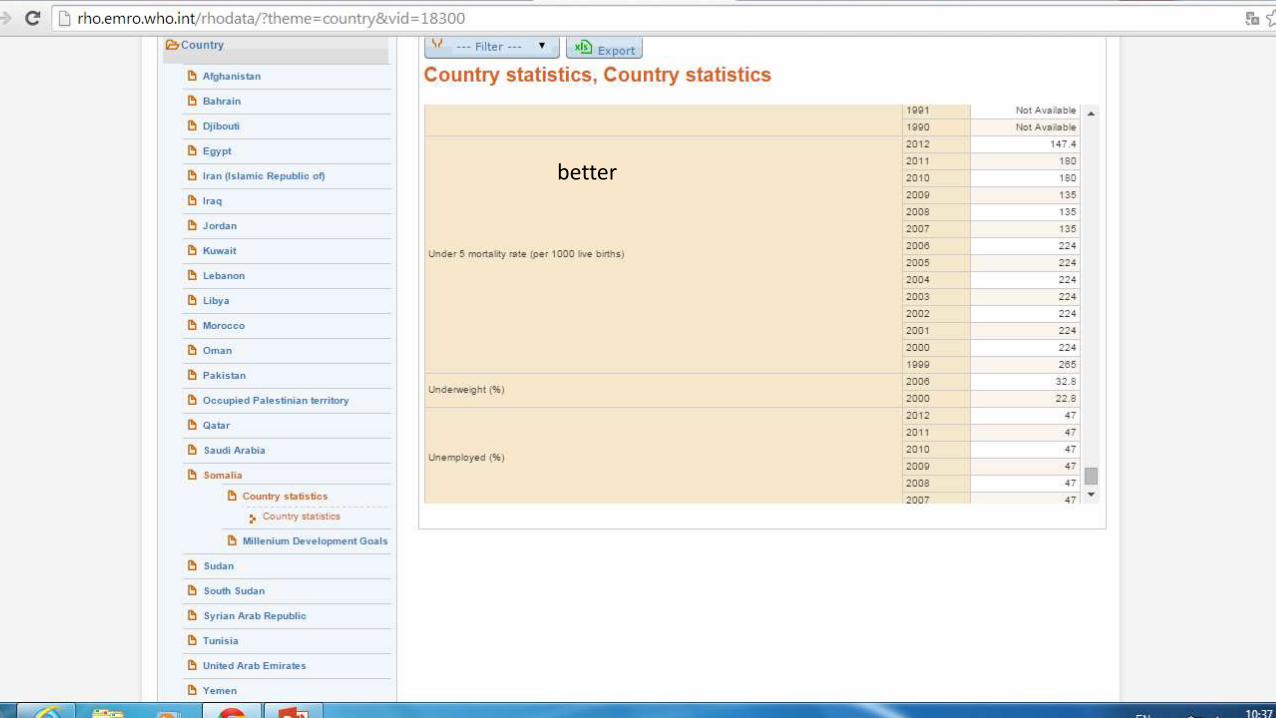
better
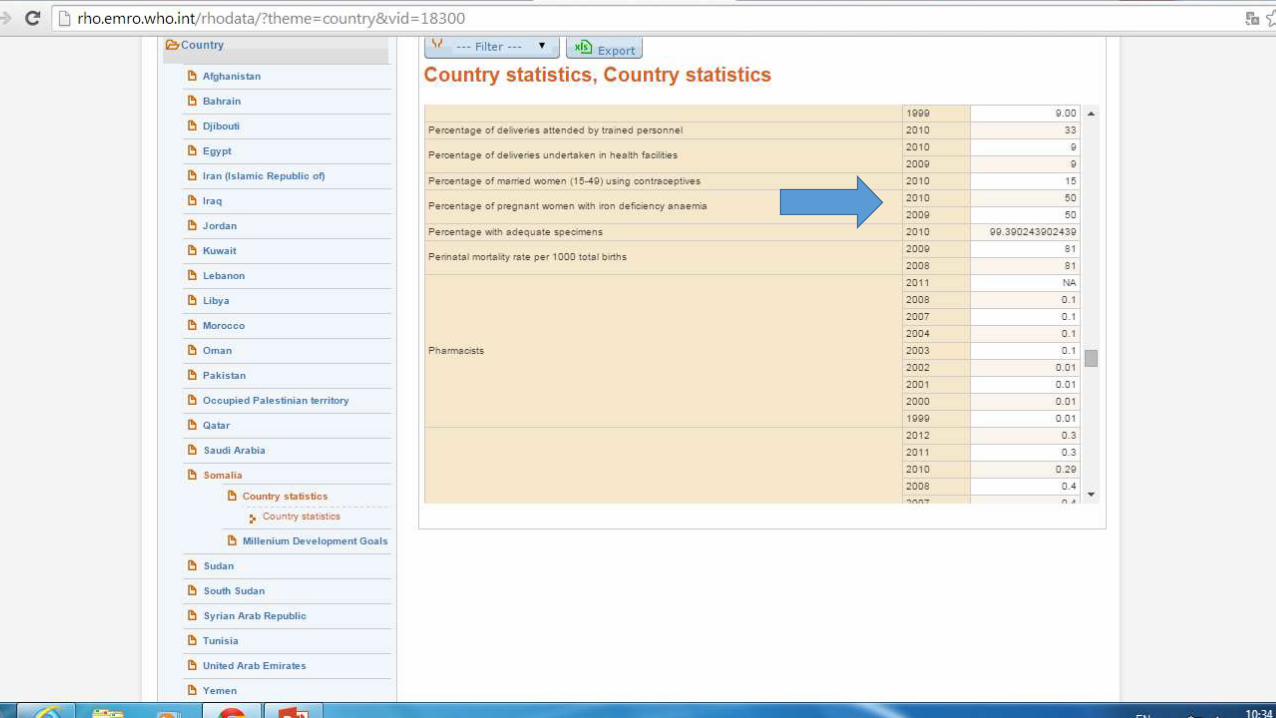


better
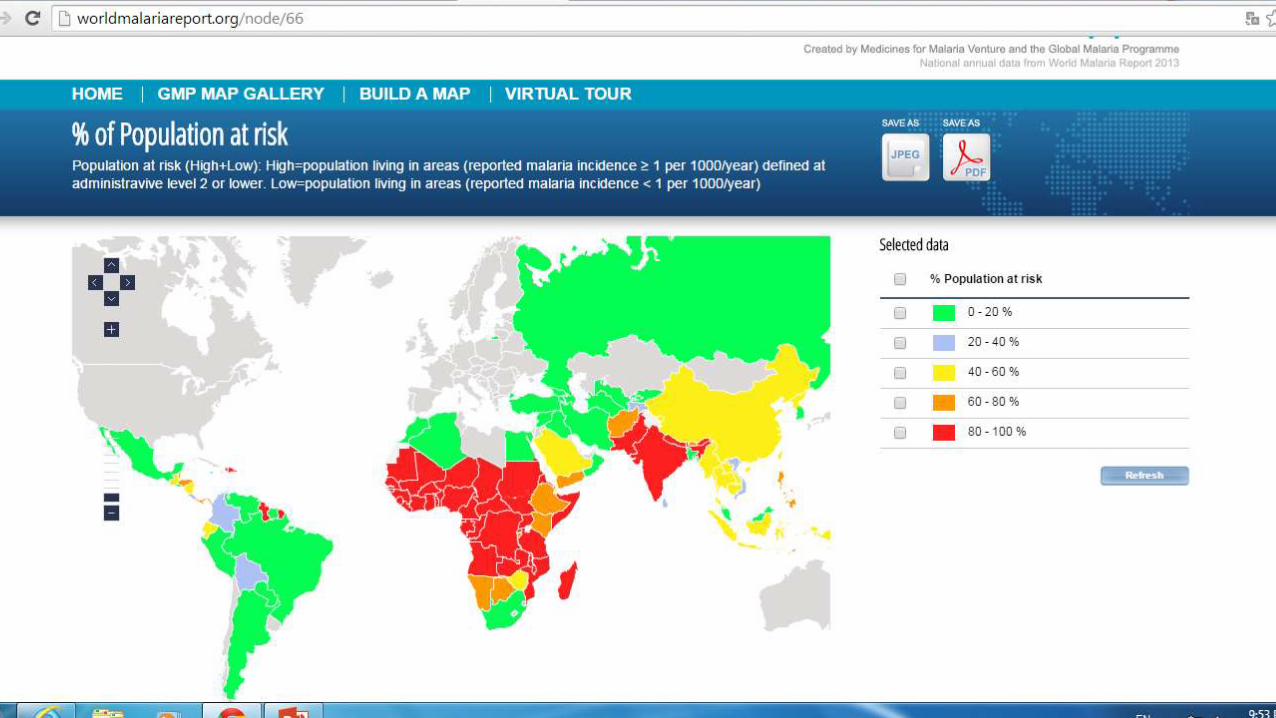
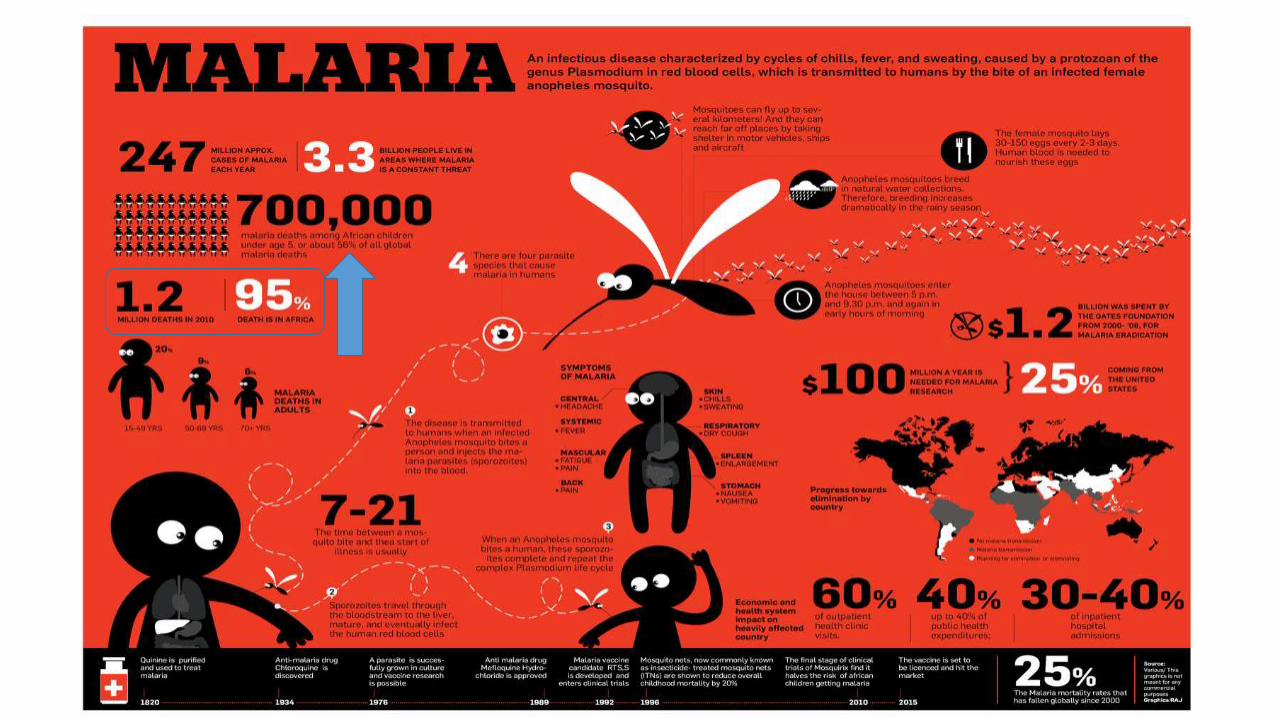
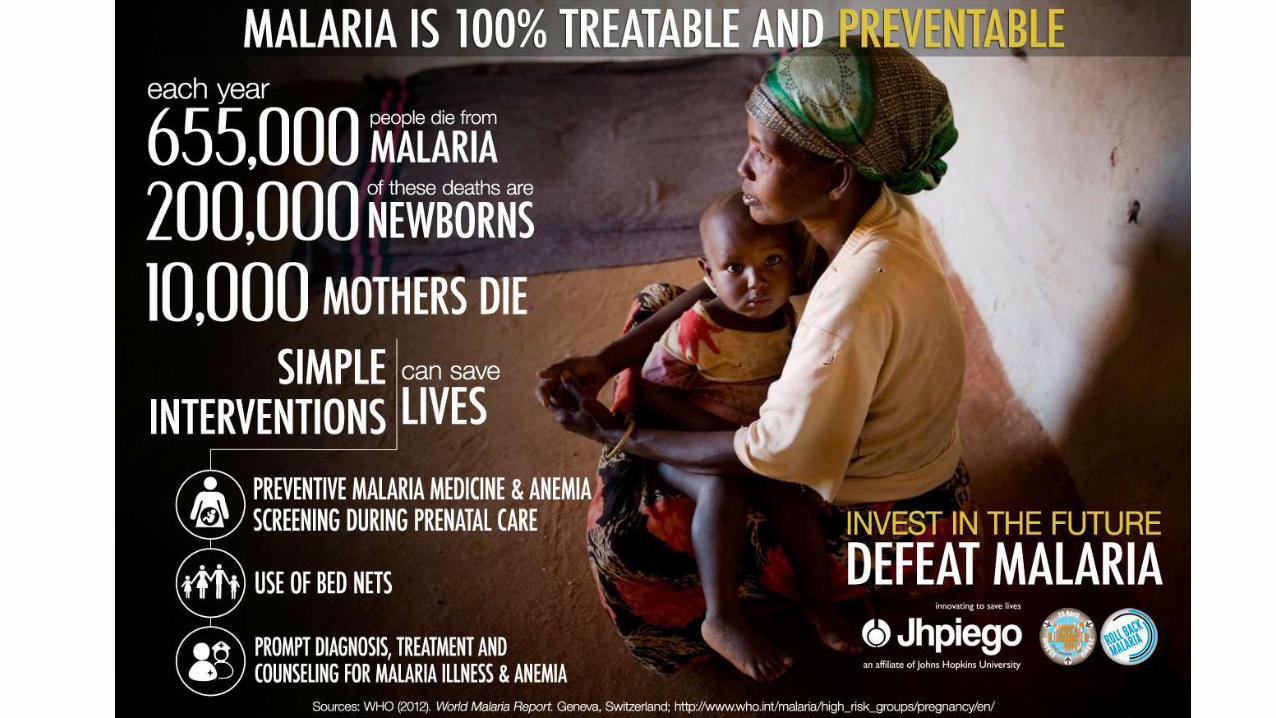
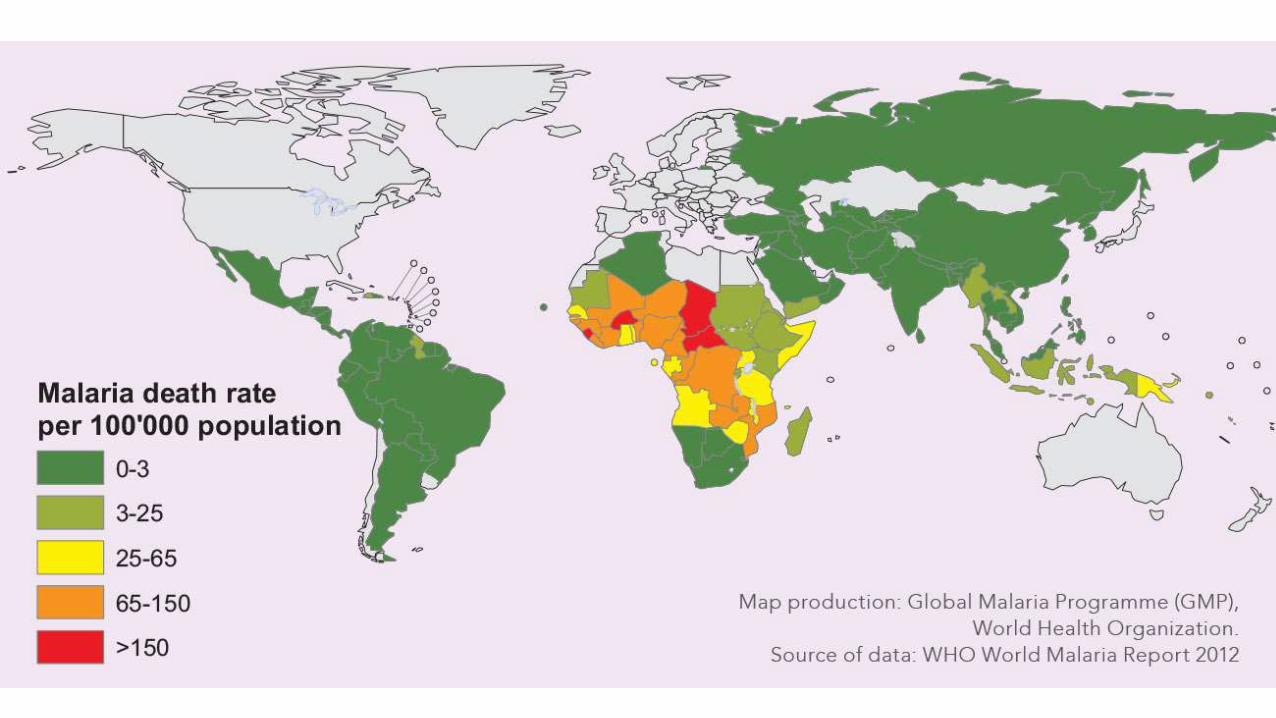



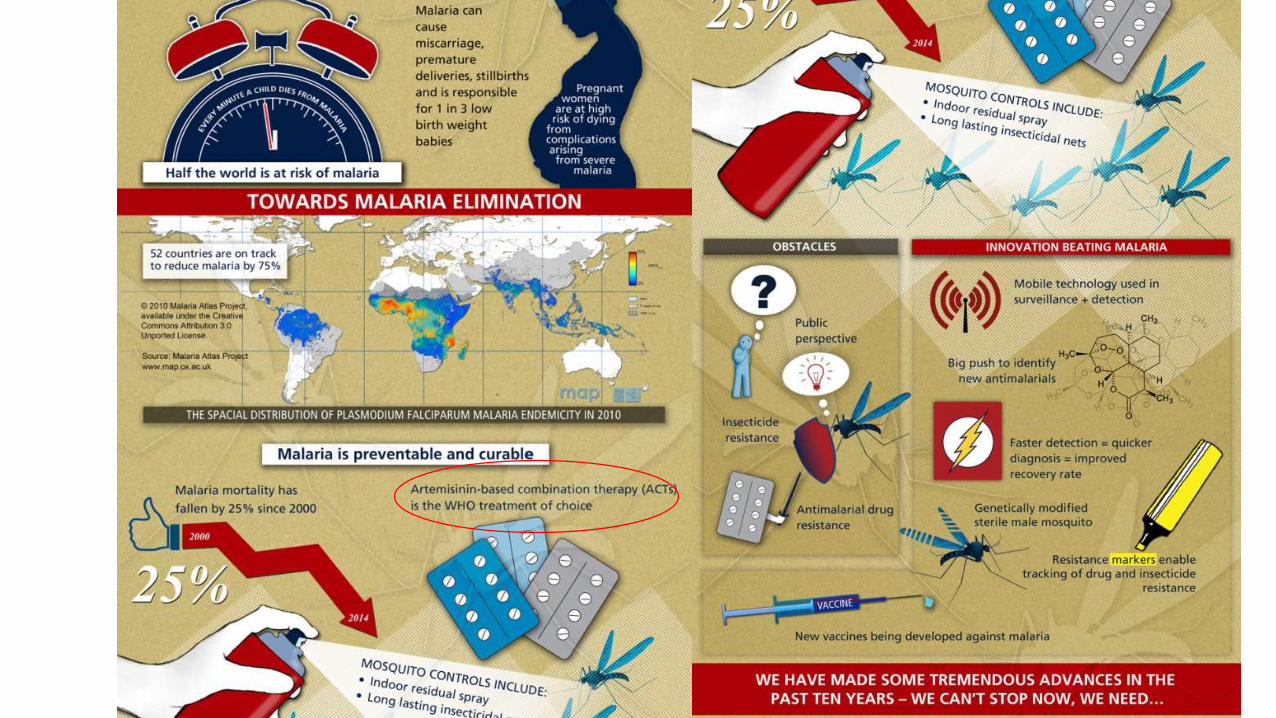


• Malaria threatens the lives of 40% of the world’s population – over
2 200 million people. Each year, there are an estimated 300-500 million clinical cases. Malaria is estimated to kill more than 1 million people annually, the majority of whom are young children.
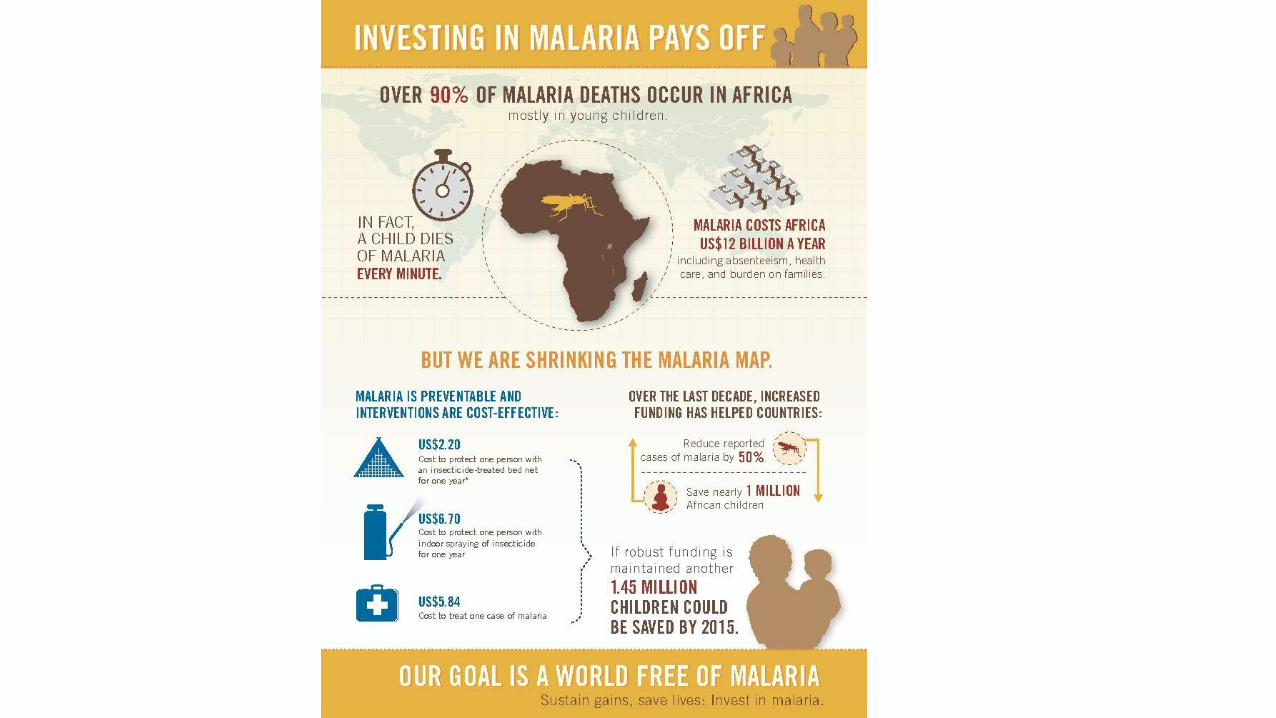
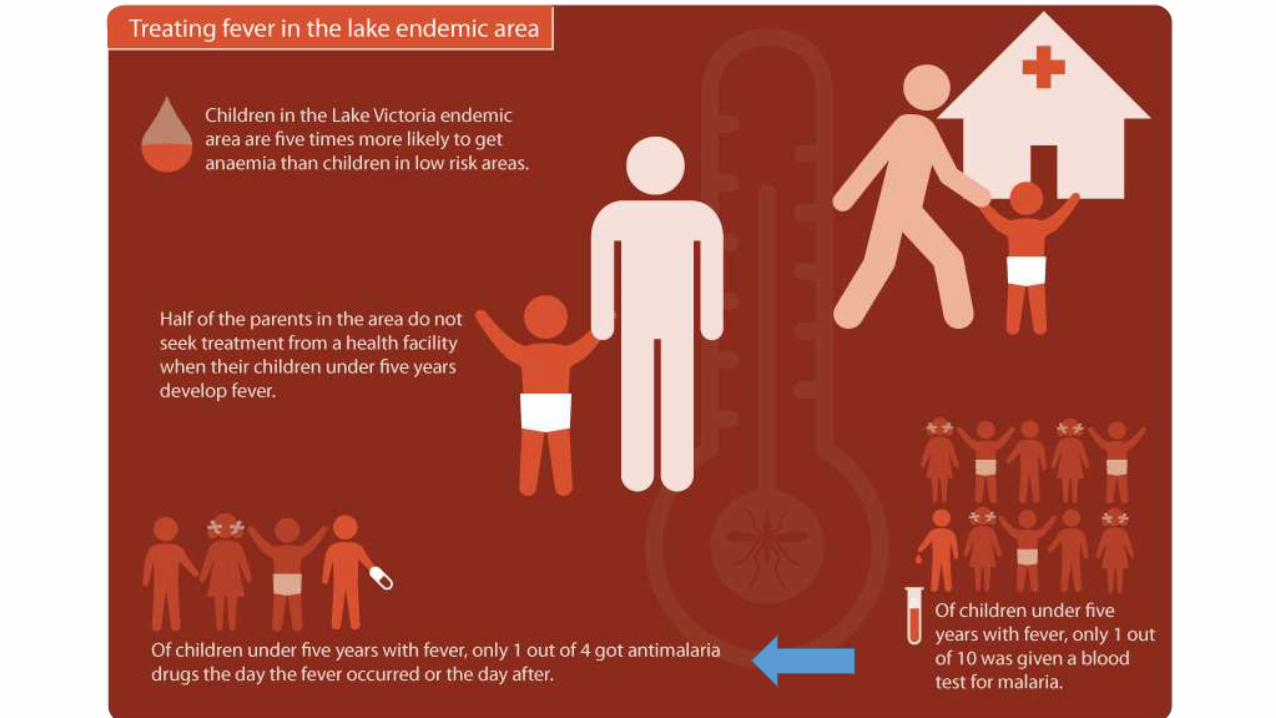
• Ninety percent of malaria cases in the world occur in Africa south of the Sahara. Children under 5 years of age and pregnant women are the worst affected by malaria.
• Africa, malaria is responsible for about 20-30% of hospital admissions and about 30-50% of outpatient consultations.
• Widespread drug resistance against commonly used antimalarial drugs such as chloroquine and pyrimethamine/sulfadoxine (Fansidar) has been reported all over the world.
ATTENTION ON;1-insecticide treated
• mosquito nets and other materials such as curtains and screens on windows and doors. The success of three large trials on insecticide-treated mosquito nets conducted in the Gambia, Kenya and Ghana and another one using treated curtains in Burkina Faso, have demonstrated that the use of insecticide-treated materials can reduce all-cause child mortality by about 25%.
• 2-changes in treatment regimen in areas of chloroquine resistance arepossible. Alternative drugs, such as pyrimethamine/sulfadoxine,mefloquine, quinine and artemisinin derivatives, provide effectivecure
• 3-increase the general care skills of parents, caregivers and health workers
> When a mosquito bites a person it sucks up blood. If the person hasmalaria, some of the parasites in the blood will be sucked into themosquito. The malaria parasites multiply and develop in the mosquito.After 10-14 days they are mature and ready to be passed on to
someone else.
Re-bite > liver (multiplies 10 times in every2 day) > bloodstream >destroying RBC’ entering to a new one

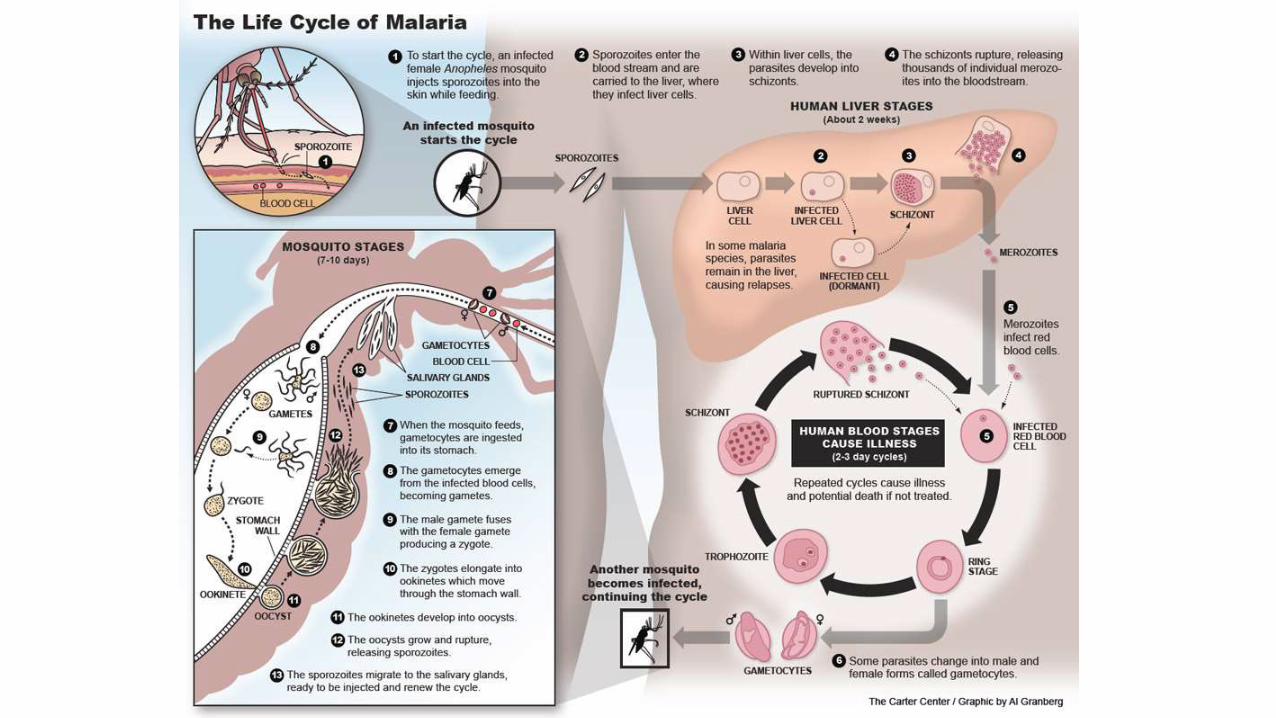

>Plasmodium falciparum which causes the severest type of malaria,
>Plasmodium vivax/ovale/malariae which cause less severe symptoms.
INC PERIOD: week to several months after infection, but usually in 7-21days.
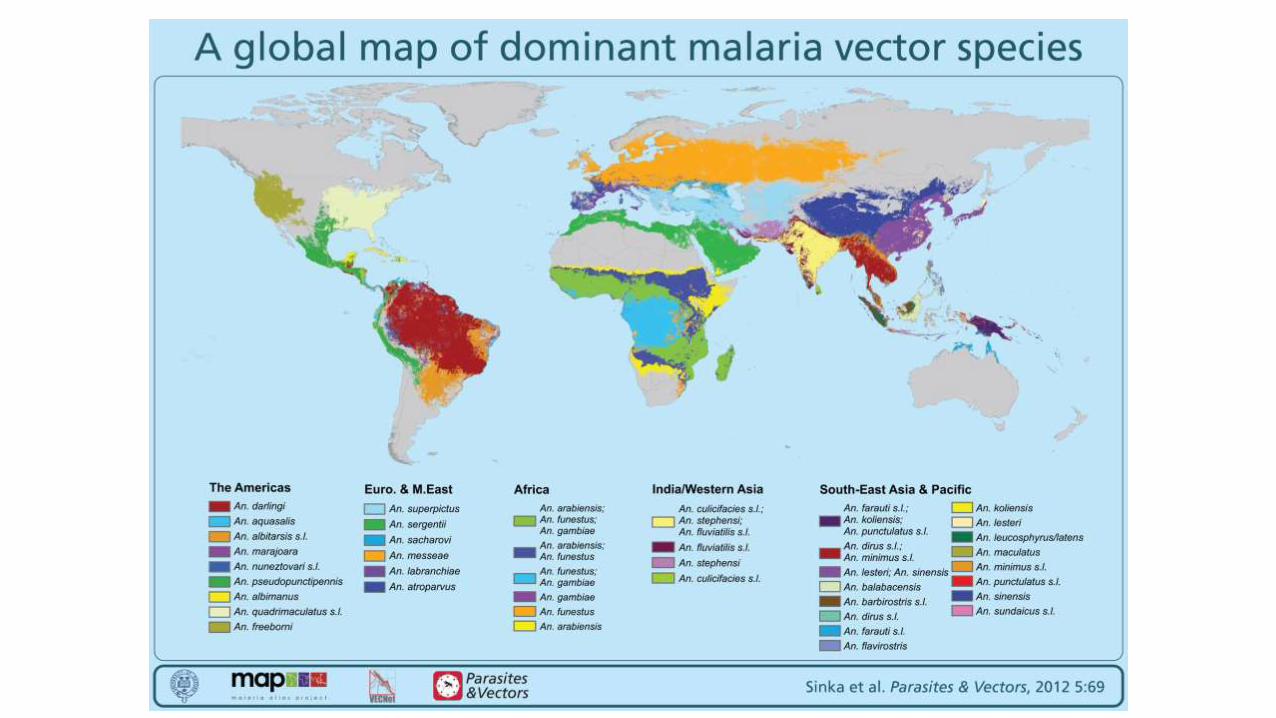
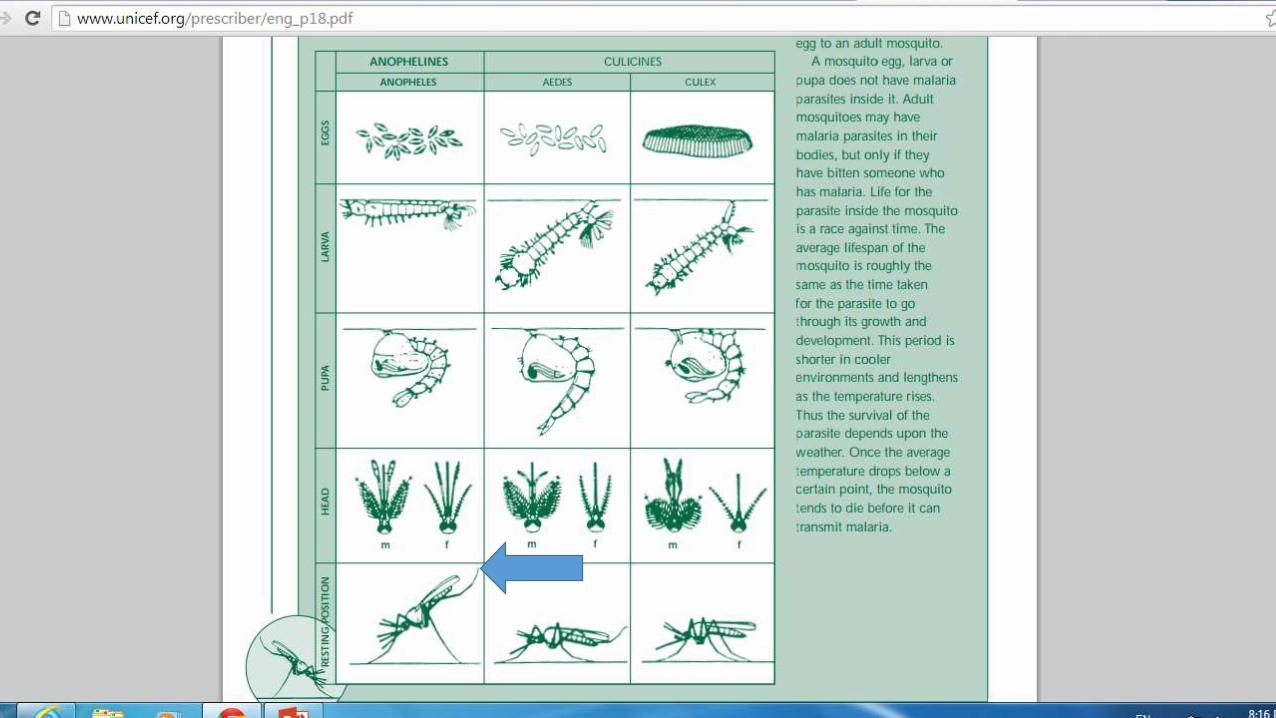
VECTOR: female Anopheles mosquitoes, can be recognized by itsupturning tail. (2-5mm wide) black spots on the surface of water,chooses stagnant or slow-flowing water, 2-3 days later larva comes out.Turns to pupa, hatches and mosq flies away, lays eggs around. All takes7-14 days.
egg, larva or pupa does not have malaria parasites inside it. Lifespanof mosq is equal to growth time of parasite
lifespan is shorter in cooler environments and lengthens as thetemperature rises. Thus the survival of the parasite depends upon theweather. Once the average temperature drops below a certain point,the mosquito tends to die before it can transmit malaria.

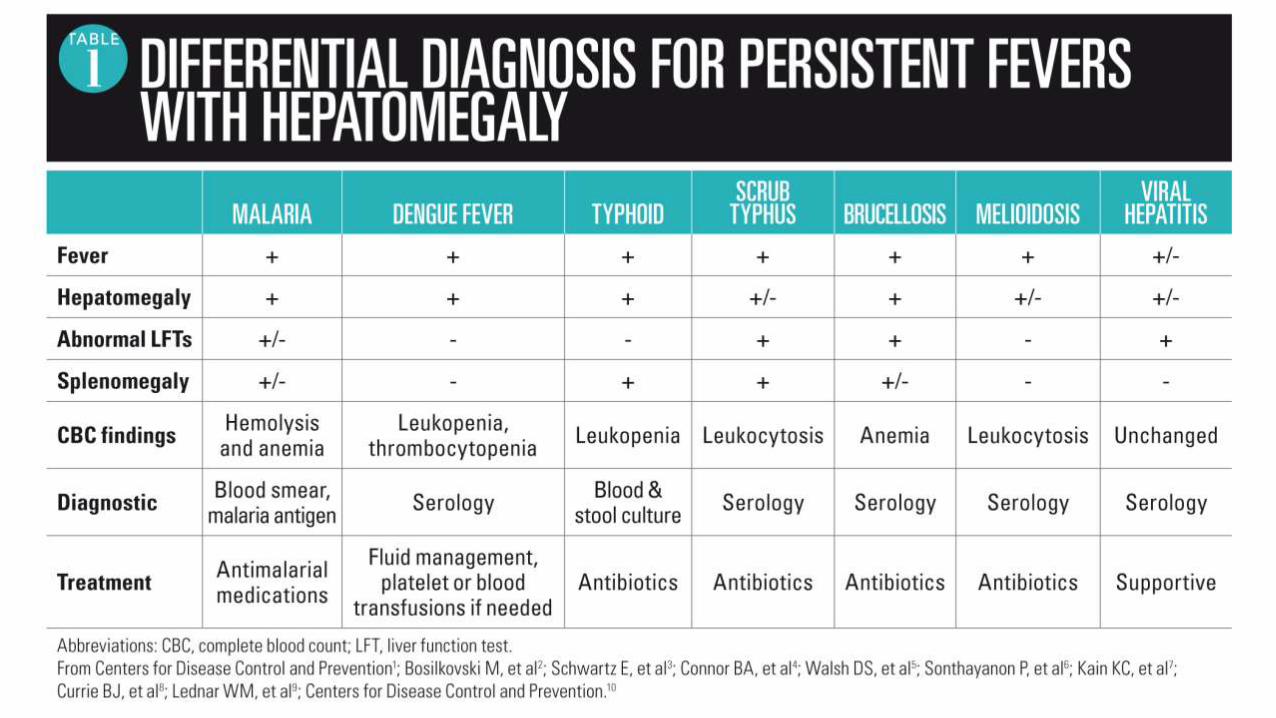
UNCOMPLICATED MALARIA• Like a minor systemic viral illness.
• headache, lassitude, fatigue, abdominal discomfort, and muscle and joint aches, usually followed by fever, chills, perspiration, anorexia, vomiting and worsening malaise, sometimes cough and diarrhea,
• Any child who presents with fever in a malaria endemic region or who recently visited such a region, must be assumed to have malaria until proven otherwise, and requires urgent treatment.
• frequently over-diagnosed,
• FEVER IS EQUAL TO MALARIA
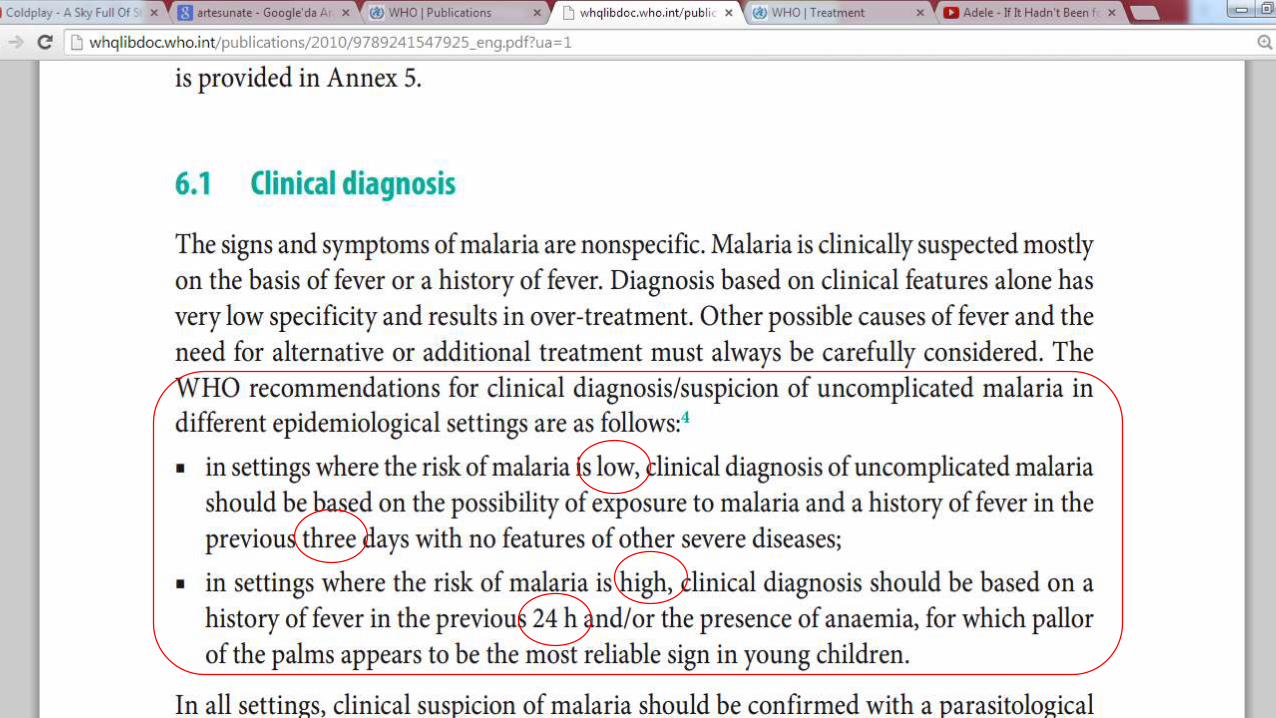
• >Ask the patient, or the adult accompanying a young patient, whether there has been any fever at any time during the past 2-3 days
• Early diagnosis and treatment will save lives
SEVERE OR COMPLICATED MALARIA
• Untreated malaria in a young child or in a non-immune individual may become complicated
• very high body temperature, drowsiness, convulsions and coma indicating heavy parasitaemia and cerebral malaria
• AND bleeding, jaundice, diminished urine output, all signifying liver and/or kidney failure, pulmonary edema, metabolic acidosis
• By this stage of the disease, the case fatality in people receiving treatment is typically 10–20%. However, if left untreated, severe malaria is fatal in the majority of cases.

NOKTURNAL ATTACK: last several hours,
shivering (body shaking) >> period of fever >> finally there is profuse sweating.
>Feels headache and pain in the back, joints and all over the body. loss of appetite, vomiting and diarrhea
Children may present as loss of consciousness, drowsiness and/or convulsions, diarrhoea, dark urine and reduced urine output (anuria).
If untreated (or inadequately treated), malaria may cause several weeks or months
It is particularly important to make an early diagnosis of malaria in young children and in pregnant women.
Malaria during pregnancy is more difficult to treat, because the parasites tend to hide in the placenta

DISEASE IMMUNITY ???>where populations are continuously exposed to a high rate of malarial inoculations partial immunity to the clinical disease and to its severe manifestation is acquired early in childhood.
>sub-Saharan Africa and parts of Oceania, the acute clinical disease described above is mostly confined to young children, who suffer high parasite densities and acute clinical disease. If untreated, this can progress very rapidly to severe malaria; adolescents and adults are partially immune and seldom suffer clinical disease, although they may continue to harbour low blood-parasite densities.
>Immunity is, however, modified in pregnancy, and it is often gradually lost, at least partially, when individuals move out of the endemic areas for long durations (usually many years).
>>Asia and Latin America, and the remaining parts of the world where malaria is endemic, the rates of inoculation fluctuate greatly over seasons and years. Entomological inoculation rates are usually <5 per year and often <1 per year. This retards the acquisition of immunity and results in people of all ages, adults and children alike, suffering acute clinical malaria, with a high risk of progression to severe malaria if untreated.

BLOOD TESTS: Examining a stained blood film under a microscope will
show whether a patient has malaria parasites in the blood (parasitaemia).
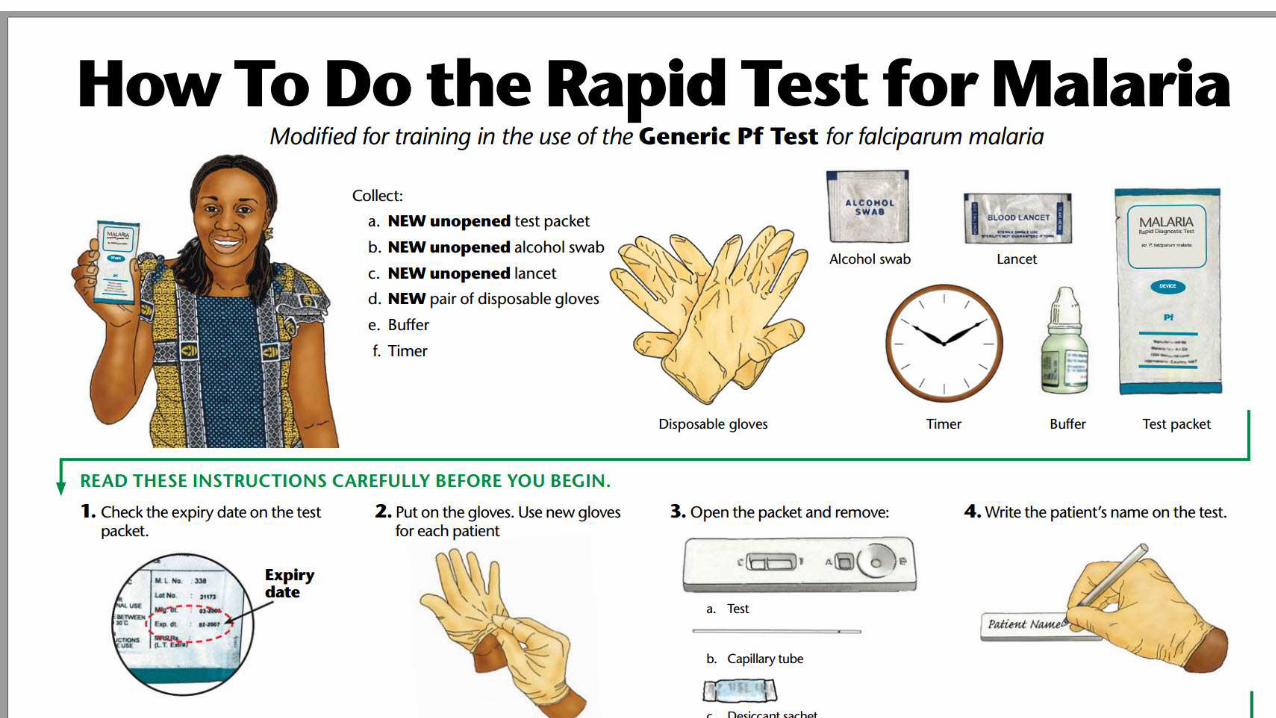
>Prompt parasitological confirmation by microscopy or alternatively by RDTs is recommended in all patients suspected of malaria before treatment is started.
>Treatment solely on the basis of clinical suspicion should only be considered when a parasitological diagnosis is not accessible
>The two methods in routine use for parasitological diagnosis are light microscopy and rapid diagnostic tests (RDTs).
>Microscopy has further advantages in that it can be used for speciation and quantification of parasites, and to assess response to antimalarial treatment.
>In the diagnosis of severe malaria cases, microscopy is a preferred option



DISTINGUISHING MALARIA FROMOTHER SERIOUS CONDITIONS> lumbar puncture may distinguish malarial coma from meningitis; careful examination of the chest may distinguish malarial breathingfrom pneumonia.
>Other conditions which may present with similar symptoms to malariainclude:
hepatitis – causing jaundice;
acute renal (kidney) failure – causing diminished urine output;
diabetes – causing deep acidotic breathing.
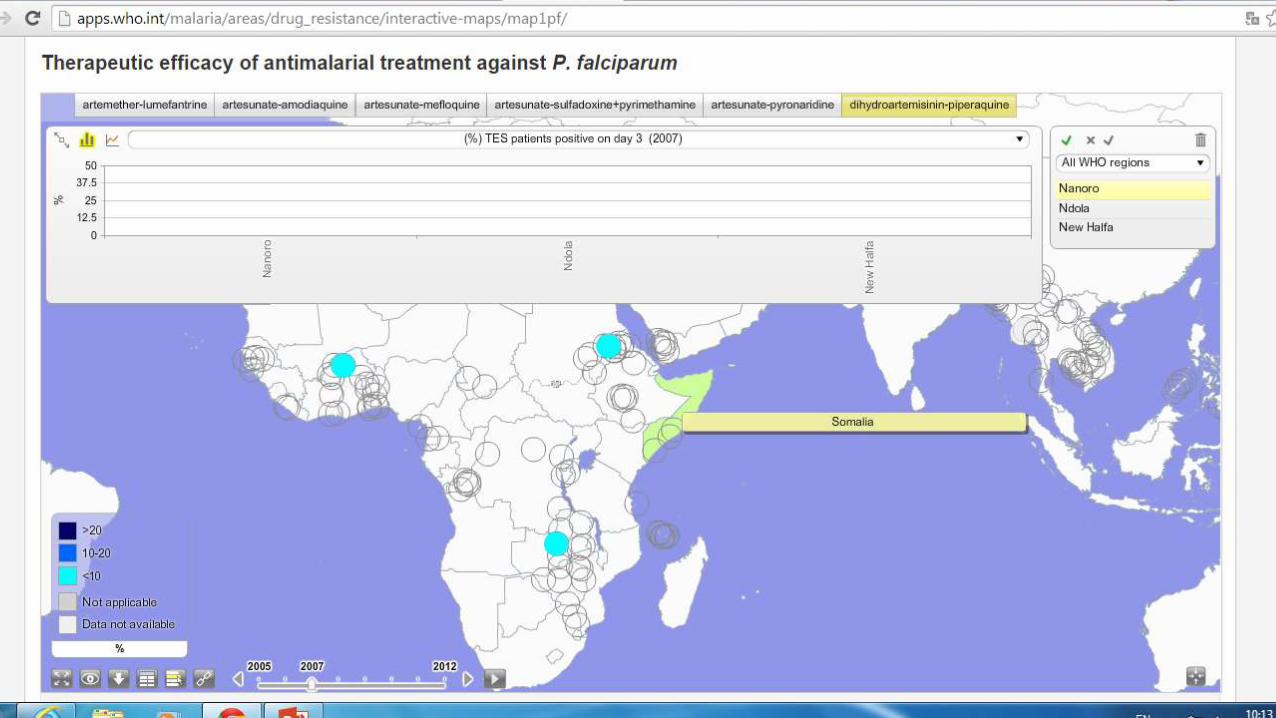
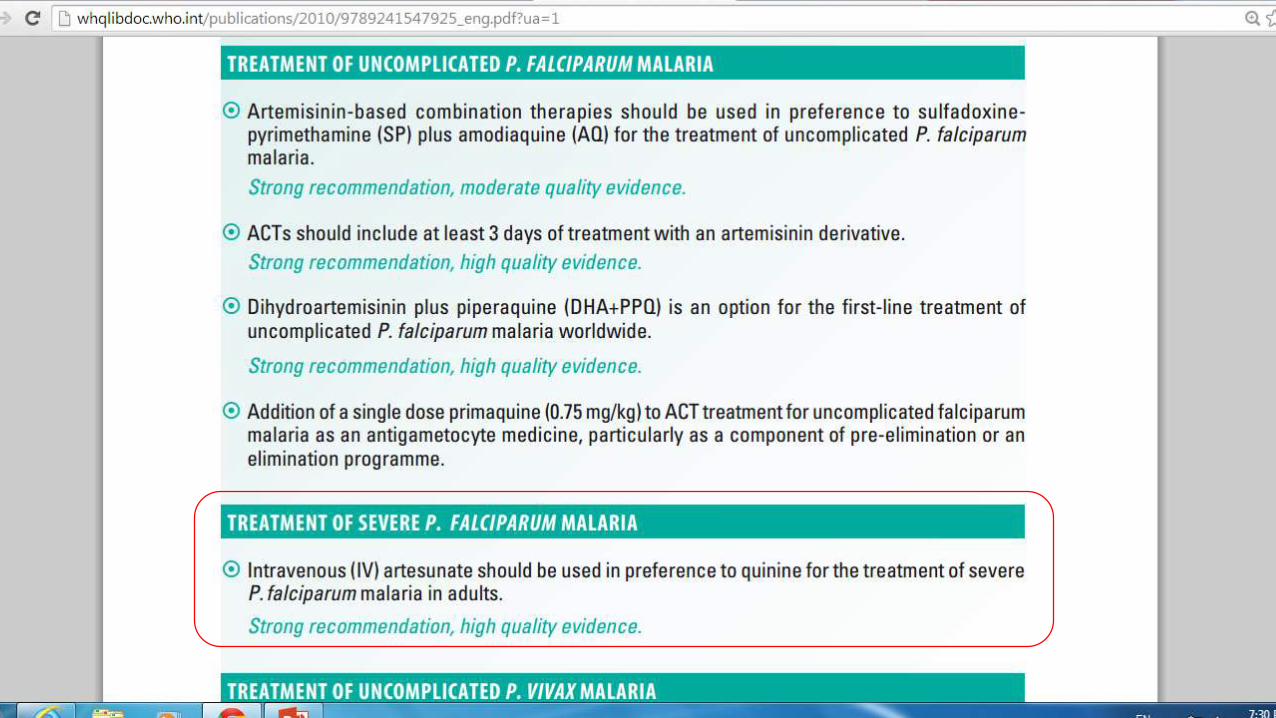
WHO GUIDELINE
>>> Since the publication of the first edition of the guidelines in 2006, most of the countries where P.falciparum is endemic have progressively updated treatment policies from the failing chloroquine (CQ) and sulfadoxine-pyrimethamine (SP) to the recommended artemisininbased combination therapies (ACTs); this is the best current treatment for uncomplicated falciparum malaria. high costs???!!!

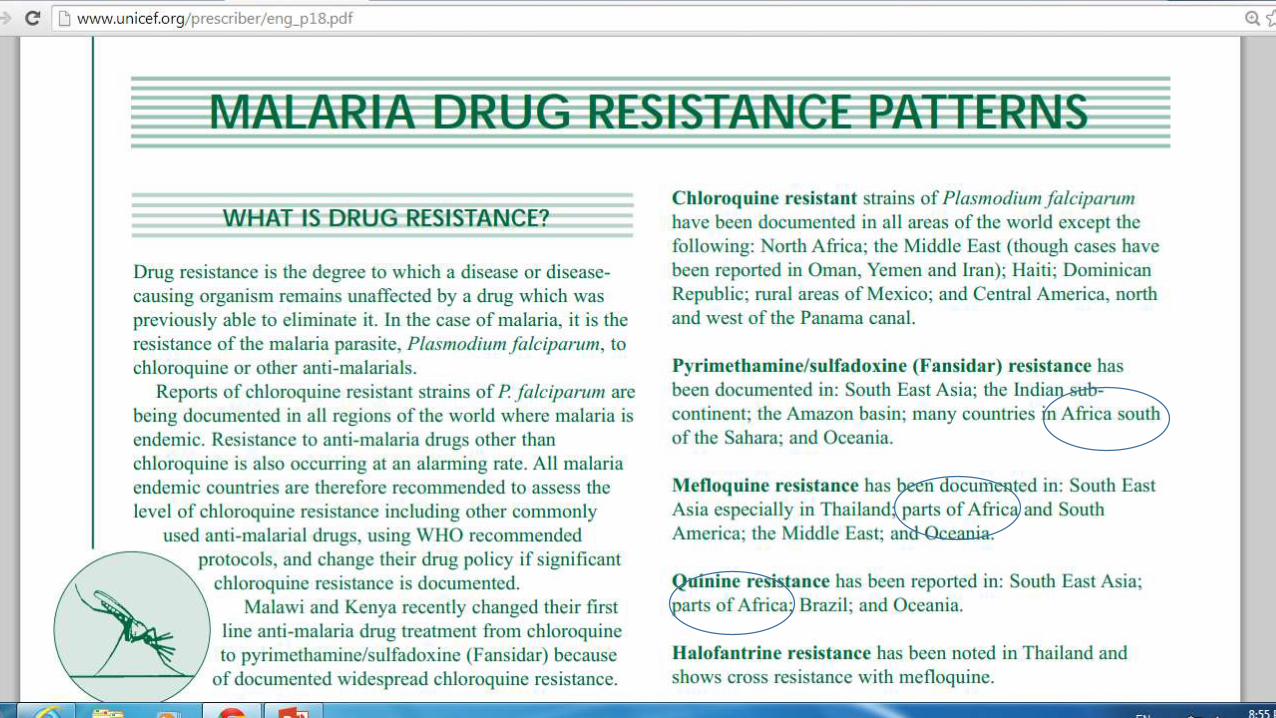
MALARIA DRUG RESISTANCE
>Reports of chloroquine resistant strains of P. falciparum are being documented in all regions of the world where malaria is Endemic.
>Malawi and Kenya recently changed their first line anti-malaria drugtreatment from chloroquine to pyrimethamine/sulfadoxine (Fansidar)
At least %30 resistance is seen…
TREATMENT
chloroquine is no longer effective in treating malaria, hence second line antimalarial drugs are often used. Artemisin comb therapy, pyrimethamine/sulfadoxine (Fansidar) or mefloquine(expensive) may be used as first line drugs
resistance to mefloquine is growing in South East Asia
> vomiting soon after medication may require more treatment
fever which persists during treatment or which returns after a few days of completed anti-malaria treatment may indicate treatment failure.
FAILURE: incomplete treatment (e.g. vomited or forgot to take pills) or because the malaria might be resistant

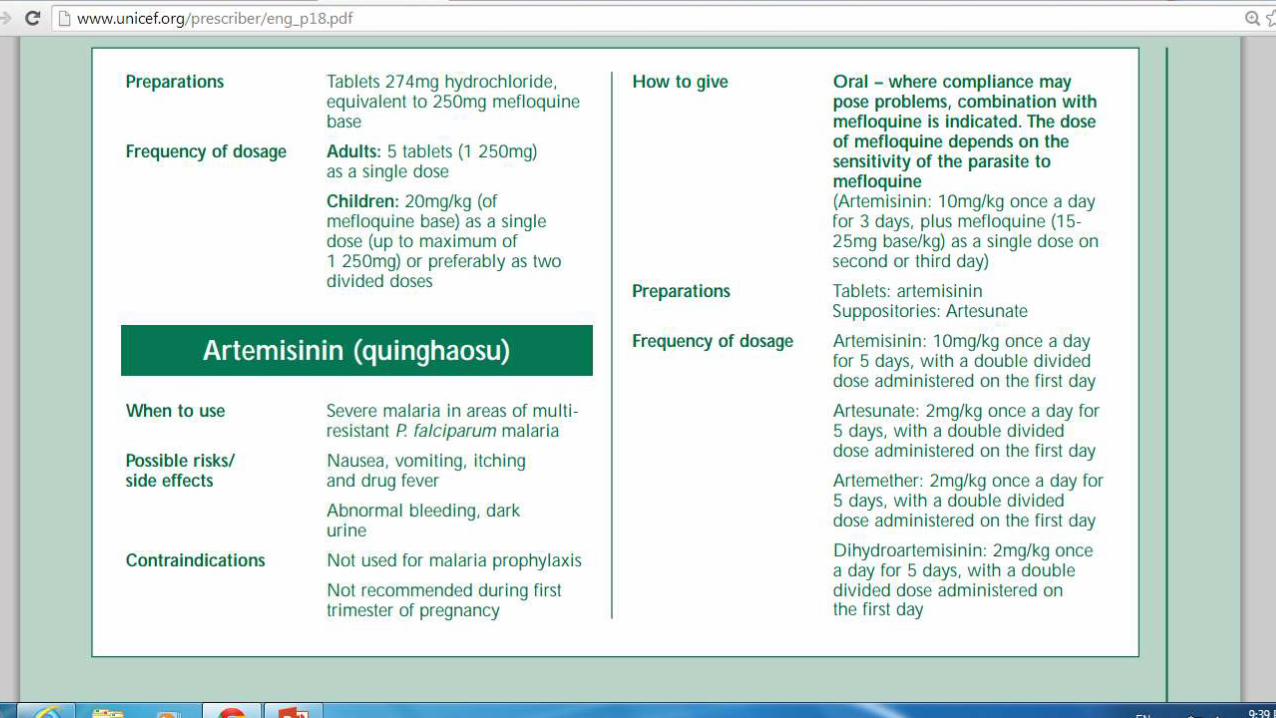
>Artemisinin is a natural product developed by Chinese scientists from the wormwood plant, Artemisia annua.
>Artemisinin clears the parasite from the body more quickly than chloroquine or quinine. It is also considered to be less toxic than quinine.
>Combination drug therapies are being advocated for treatment of malaria, e.g. mefloquine plus artemisinin
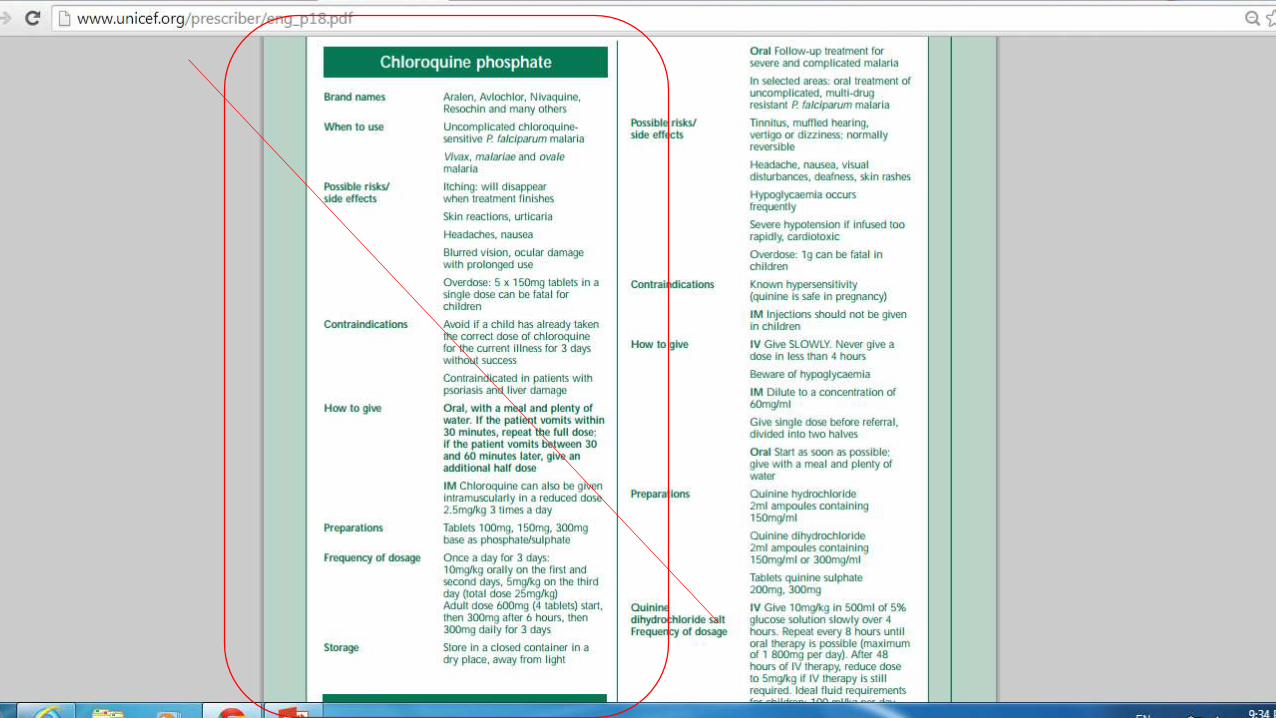
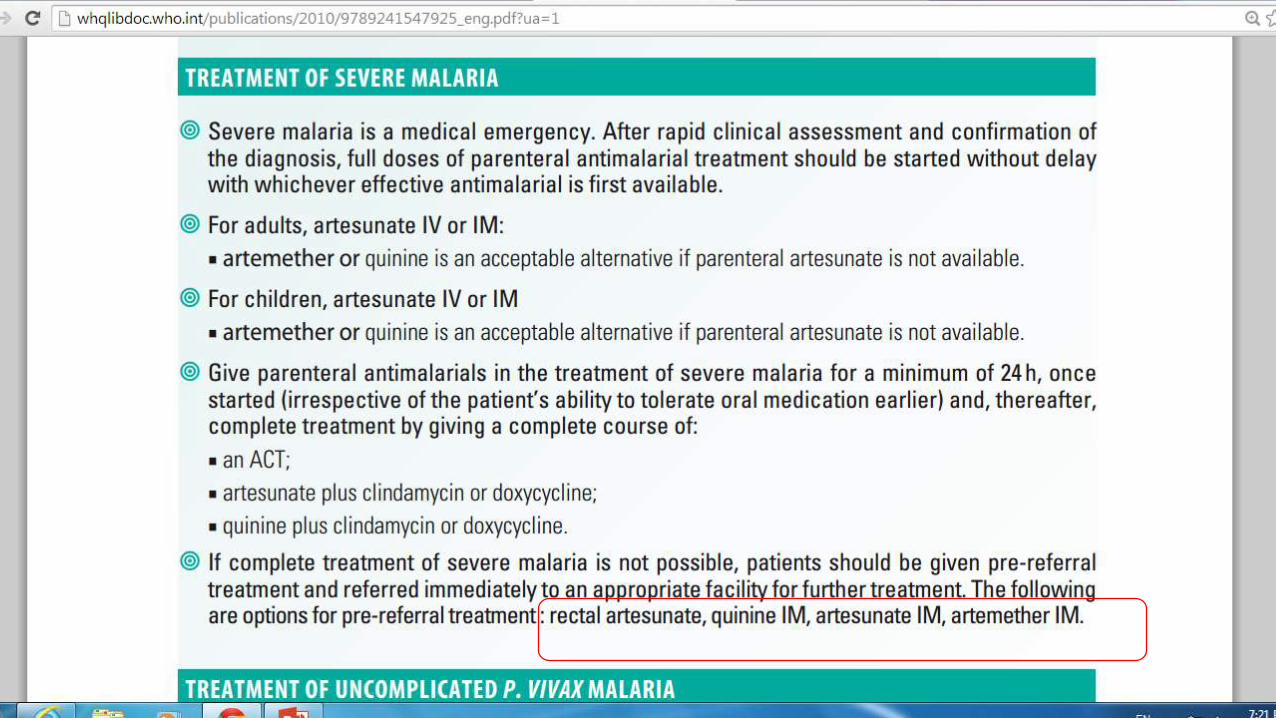
TREATMENT OF SEVERE OR COMPLICATED MALARIA>intravenous quinine or artemisinin derivatives. IV infusion of quinine should be given slowly over 8 hours to avoid cardiac complications. This should be followed by oral quinine tablets for a total of 7 days
Artemisinin, if available, can be given in suppository form
fever, give paracetamol or aspirin


CHILDREN - TREATMENT
> The child should be observed for 1 hour. If the child vomits during
that time, treatment should be repeated (full dose if the drug is vomited before 30 minutes, half dose if vomited between 30 minutes and 1 hour). If the child vomits repeatedly, he or she must be hospitalized.
> Children with malaria may have other infections at the same time, such as meningitis or pneumonia. If coma and fever persist, it may be a result of the common association of severe malaria with meningitis, pneumonia or sepsis

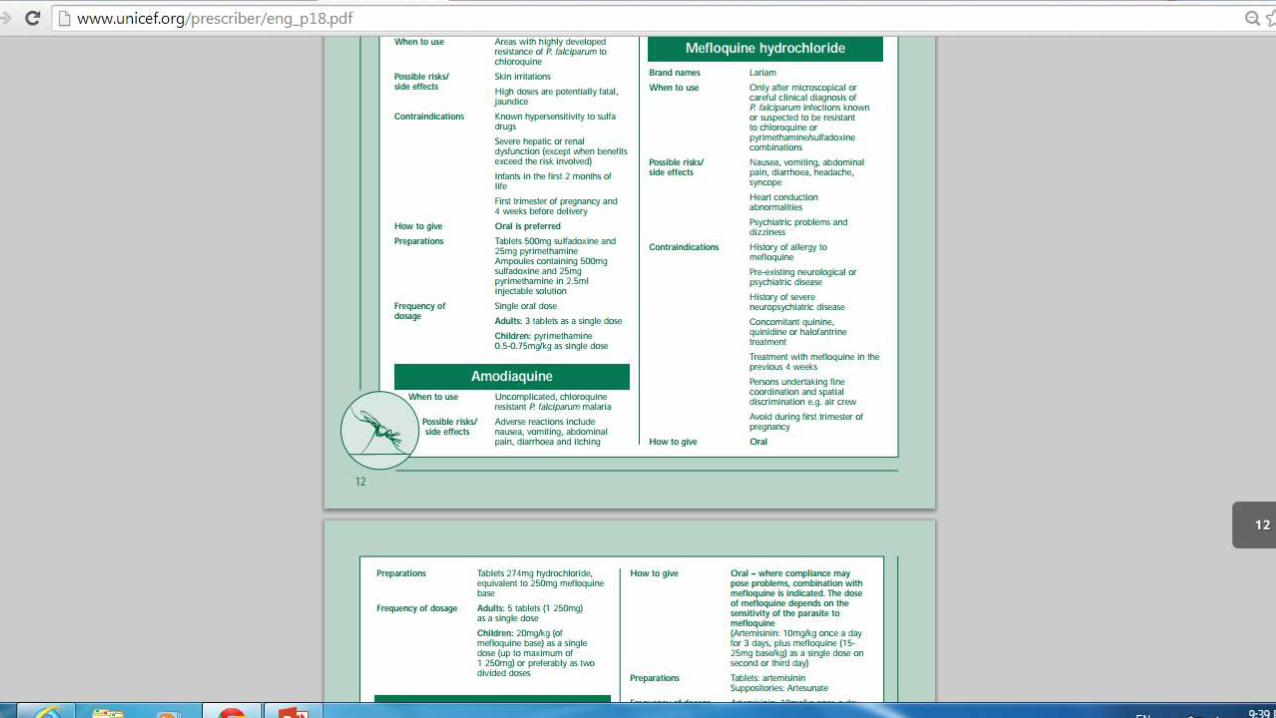
OTHER DRUGS USED IN THE TREATMENT OF MALARIA

(artemisinin-combination therapies, ACTs)


MALARIA IN PREGNANCY In some countries, national policies recommend routine use of anti-
malarial drugs during pregnancy.
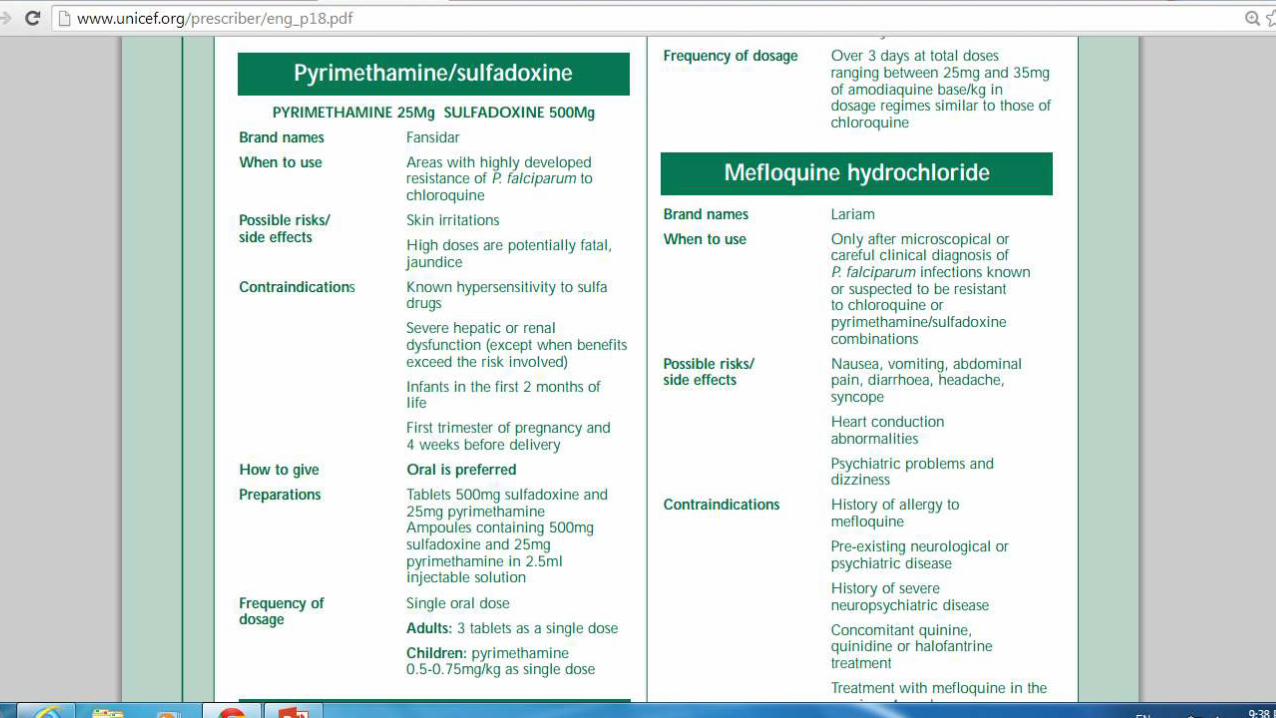
>Pyrimethamine/sulfadoxine (Fansidar) has been used as prophylaxis/intermittent treatment in Malawi and in Kenya with good preliminary results.
Chloroquine, amodiaquine, quinine can all be safely given during pregnancy.
Artemisinin and its derivatives are also safe from the fourth month of pregnancy onwards, though it is not recommended during the first 3 months of pregnancy.
Mefloquine ??? Not known about safety, maybe after 1st tri
CHEMOPROPHYLAXIS AGAINST MALARIA
during pregnancy, all migrants and travelers
>Chemoprophylaxis is an effective strategy for a limited time (ranging from a few weeks to a few years). However, it does not offer lifelong protection
chloroquine resistance in many countries, chloroquine is no longer the drug of choice for prophylaxis in many regions of the world.
Mefloquine is the first drug of choice. The recommended dose is 1 tablet (250mg) weekly starting 1-2 weeks before departure to malaria endemic regions and continued for 4 weeks after return.

>For children the dose is:
Weight over 45kg 1 tablet weekly
31-45kg three-quarters of a tablet weekly
20-30kg half a tablet weekly
5-19kg quarter of a tablet weekly
again continued for 4 weeks after leaving a malaria area.
Side effects of mefloquine are: nausea, vomiting, abdominal pain, diarrhoea, headache, dizziness, abnormal heart rhythm and liver dysfunction.

ALTERNATIVE DRUGS FOR CHEMOPROPHYLAXIS
Doxycycline: Dosage 100mg daily for 2 days before departure and continued for 4 weeks after return from a malaria zone. It is contraindicated in children under 8 years of age. Side effects include nausea, vomiting, abdominal pain and in women it may cause frequent vaginal candida infections. It is contraindicated during pregnancy.
> Pyrimethamine/sulfadoxine (Fansidar), is no longer recommended for routine weekly prophylaxis, because of the danger of severe cutaneous reaction and sudden death.

Artemisinin-based combination therapy(ACT)>These are combinations in which one of the components is artemisinin and its derivatives (artesunate, artemether, dihydroartemisinin).
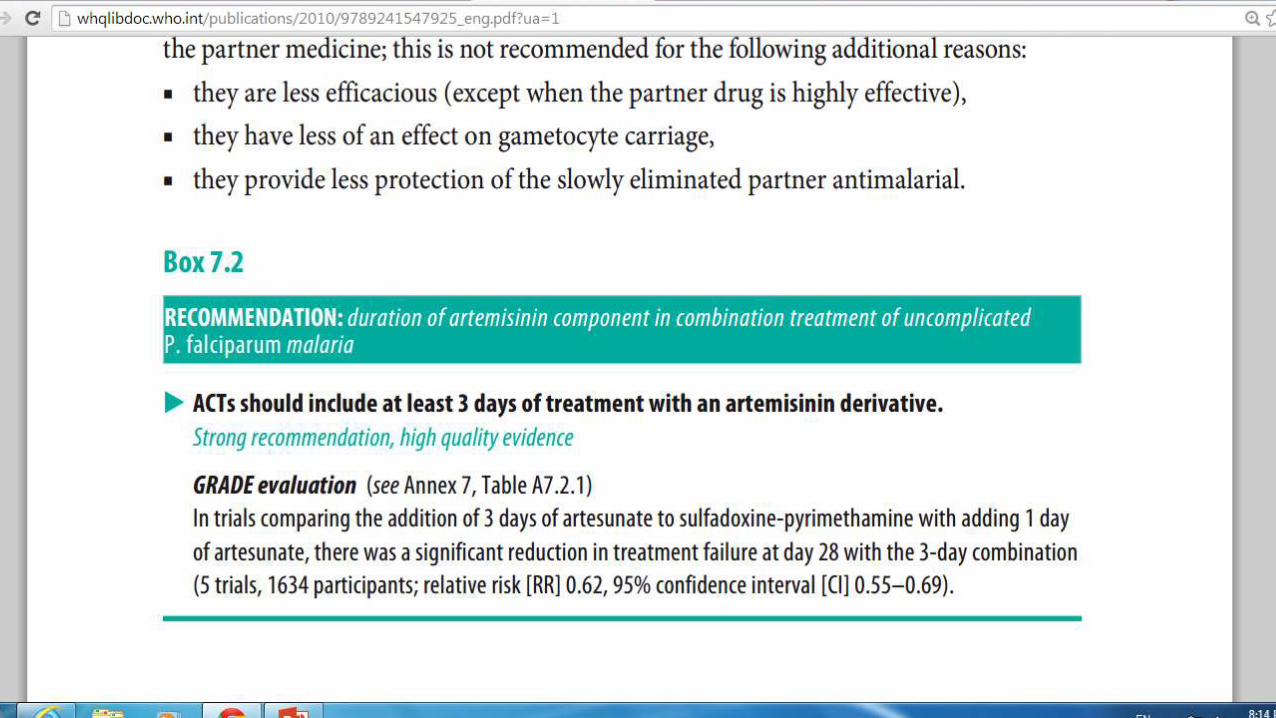
artemisinin and its derivatives are eliminated rapidly, when given alone or in combination with rapidly eliminated compounds (tetracyclines, clindamycin), a 7-day course of treatment
in combination with slowly eliminated antimalarials. With this shorter 3-day course
To eliminate at least 90% of the parasitaemia, a 3-day course of the artemisinin is required to cover up to three post-treatment asexual cycles of the parasite. This ensures that only about 10% of the parasitamia is present for clearance by the partner medicine, thus reducing the potential for development of resistance.


many countries, artemether pluslumefantrine(COARTEM), artesunate plusmefloquine ordihydroartemisinin pluspiperaquine may give thehighest cure rates
The low levels of resistance to AQ and SP in some parts of Africa stillmakes artesunate plusamodiaquine orsulfadoxine-pyrimethamine effectiveoptions.


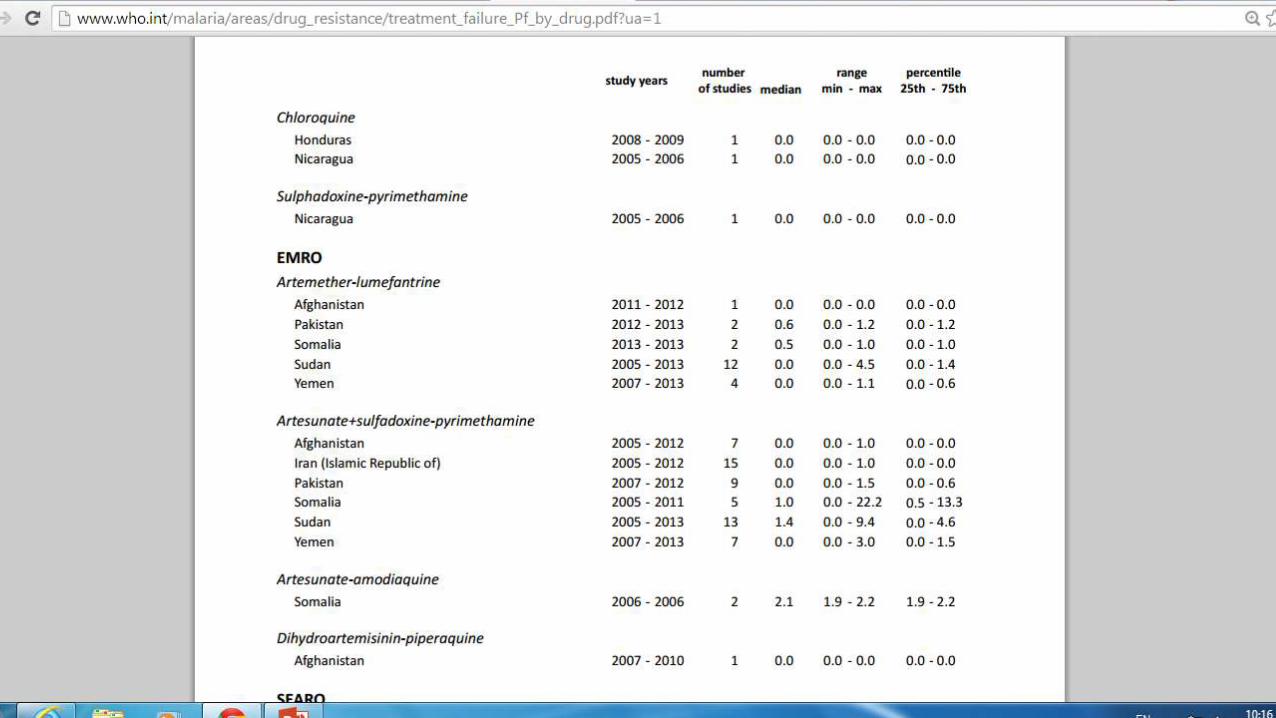
TREATMENT FAILURE OF ACT
if fever and parasitaemia fail to resolve or recur within two weeks of treatment then this is considered a failure of treatment. Treatment failures may result from drug resistance, poor adherence or inadequate drug exposure (from under-dosing, vomiting or unusual pharmacokinetic properties in that individual) or substandard medicines.
Wherever possible, treatment failure must be confirmed parasitologically– preferably by blood slide examination
In many cases, failures are missed because patients who present with malaria are not asked whether they have received antimalarial treatment within the preceding 1–2 months. This should be a routine question in patients who present with malaria.
TREATMENT FAILURE OF ACT
Treatment failure within 14 days of receiving an ACT is very unusual, with the majority of treatment failures occurring after two weeks of initial treatment.
failure rates at day 14 ranged from 1–7%.
Treatment failures within 14 days of initial treatment should be treated with a second-line antimalarial


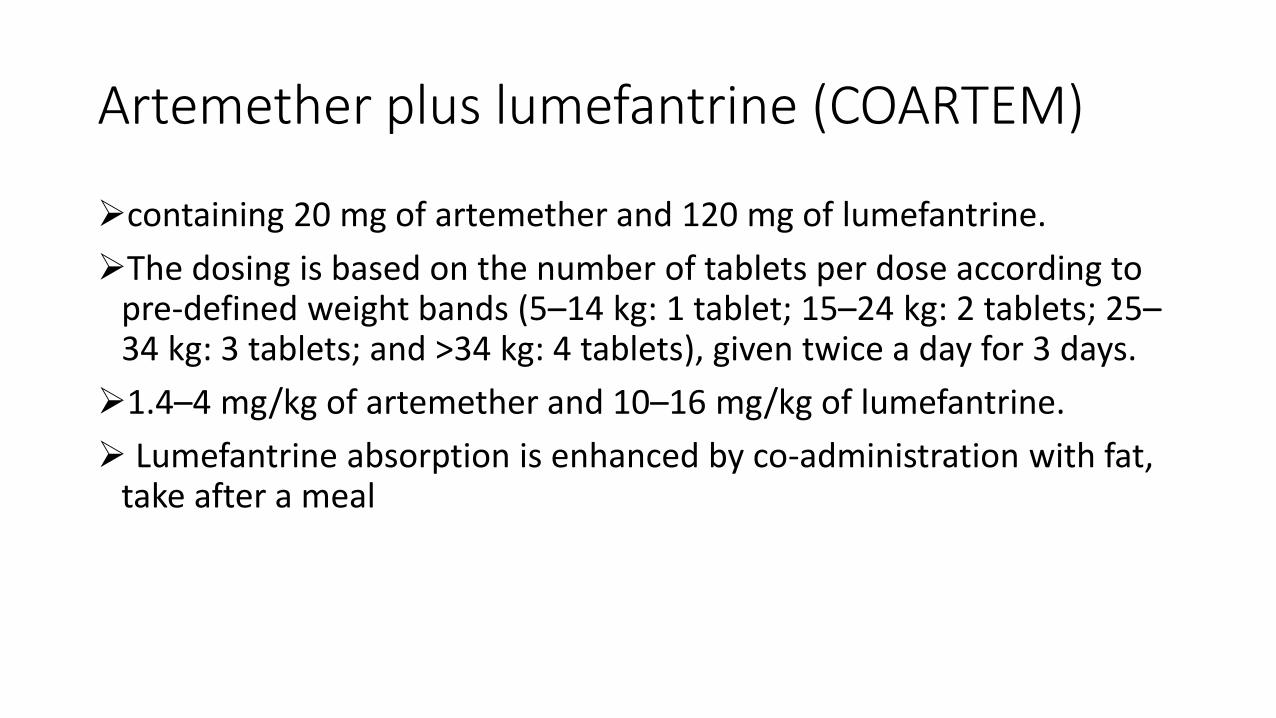
Artemether plus lumefantrine (COARTEM)
containing 20 mg of artemether and 120 mg of lumefantrine.
The dosing is based on the number of tablets per dose according to pre-defined weight bands (5–14 kg: 1 tablet; 15–24 kg: 2 tablets; 25–34 kg: 3 tablets; and >34 kg: 4 tablets), given twice a day for 3 days.
1.4–4 mg/kg of artemether and 10–16 mg/kg of lumefantrine.
Lumefantrine absorption is enhanced by co-administration with fat, take after a meal
Artesunate plus amodiaquine
> A target dose of 4 mg/kg/day artesunate and 10 mg/kg/day amodiaquine once a day for 3 days, with a therapeutic dose range between 2–10 mg/kg/day artesunate and 7.5–15 mg/kg/dose amodiaquine.

Artesunate plus mefloquine50 mg of artesunate and 250 mg base of mefloquine tablets
respectively
A target dose of 4 mg/kg/day artesunate given once a day for 3 days and 25 mg/kg of mefloquine either split over 2 days as 15mg/kg and 10mg/kg or over 3 days as 8.3 mg/kg/day once a day for 3 days. The therapeutic dose range is between 2–10 mg/kg/dose/day of artesunate and 7–11 mg/kg/dose/day of mefloquine.
Mefloquine is associated with an increased incidence of nausea, vomiting, dizziness, dysphoria and sleep disturbance
the 25 mg/kg dose is usually split and given either as 15 mg/kg (usually on the second day) followed by 10 mg/kg one day later, or as a daily dose of 8.3 mg/kg for 3 days.
Artesunate plus sulfadoxine-pyrimethamine
> separate scored tablets containing 50 mg of artesunate and tablets containing 500 mg of sulfadoxine and 25 mg of pyrimethamine
>A target dose of 4 mg/kg/day artesunate given once a day for 3 daysand a single administration of 25/1.25 mg/kg sulfadoxine-pyrimethamine on day 1, with a therapeutic dose range between 2–10 mg/kg/day artesunate and 25–70/1.25–3.5 mg/kg sulfadoxine-pyrimethamine.

Dihydroartemisinin plus piperaquine
> fixed-dose combination with tablets containing 40 mg of
dihydroartemisinin and 320 mg of piperaquine.
> A target dose of 4 mg/kg/day dihydroartemisinin and 18 mg/kg/day
piperaquine once a day for 3 days, with a therapeutic dose range between 2–10 mg/kg/day dihydroartemisinin and 16–26 mg/kg/dose piperaquine
Artesunate plus tetracycline or doxycycline orclindamycin> Artesunate (2 mg/kg once a day) plus tetracycline (4 mg/kg four times a day or doxycycline (3.5 mg/kg once a day) or clindamycin (10 mg/kg twice a day). Any of these combinations should be given for 7 days.
COMBINATION THERAPYYYYYYYYYYY
• With the exception of lumefantrine, the partner medicines of all other ACTs have been used previously as monotherapies, and amodiaquine, mefloquine and SP continue to be available as monotherapy in many countries. Despite recommendations and warnings, artemisinin derivatives are available as monotherapy in the market place in many countries, and they are being used as such for the treatment of uncomplicated malaria

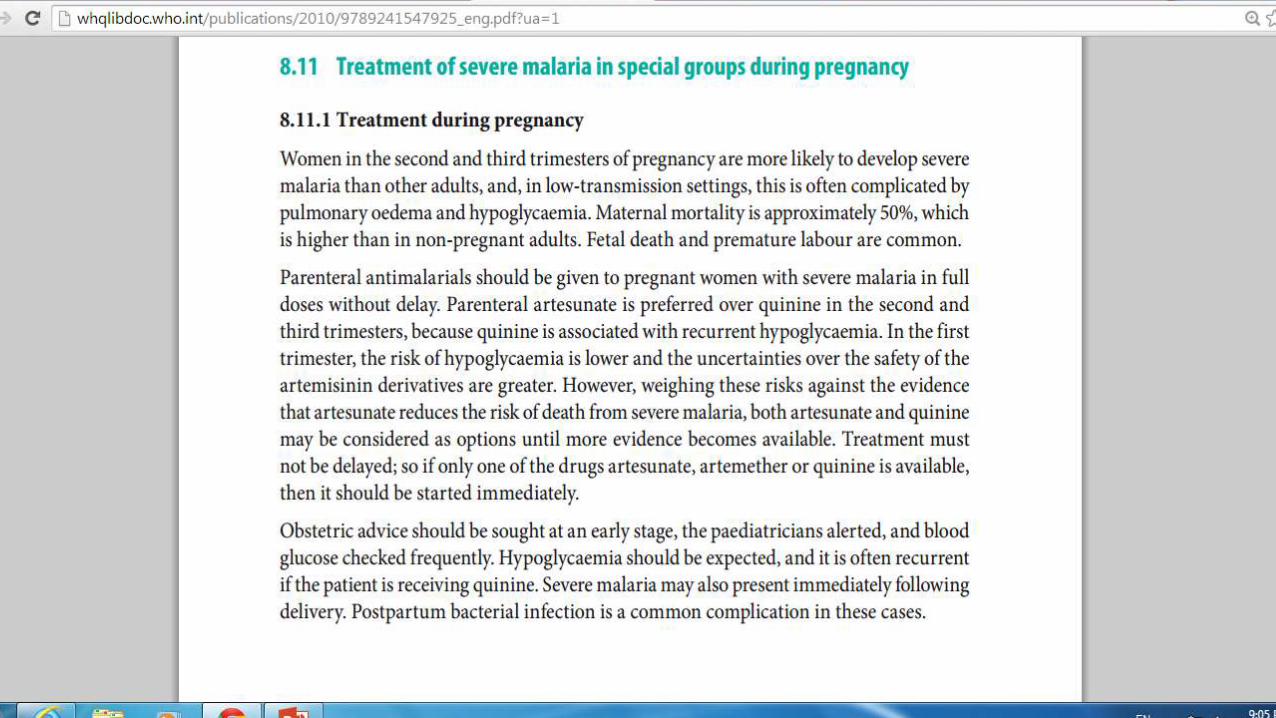
PREGNANCY & MALARIAMalaria in pregnancy is associated with low birth weight, increased
anaemia and, in low-transmission areas, an increased risk of severe malaria and death.
antimalarial medicines considered safe in the first trimester of pregnancy are quinine, chloroquine, clindamycin and proguanil.
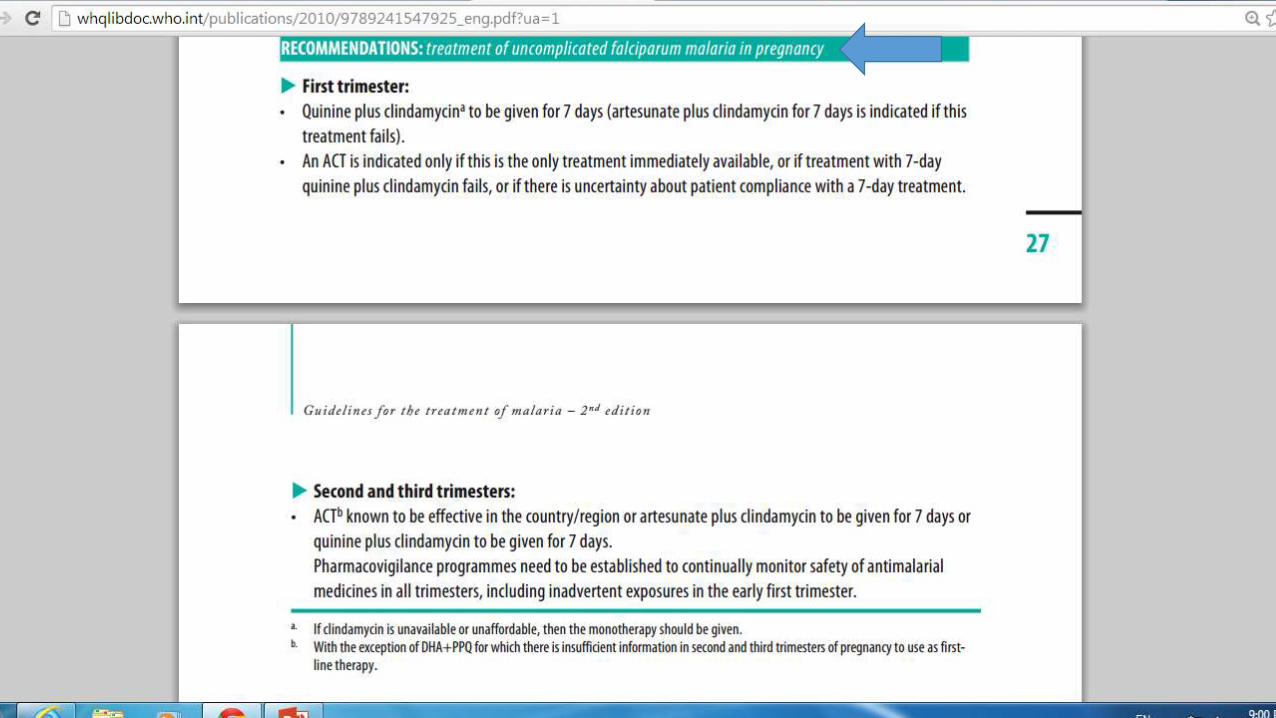
Pregnant women in the first trimester with uncomplicated falciparum malaria should be treated with quinine plus clindamycin for seven days (and quinine monotherapy if clindamycin is not available). Artesunate plus clindamycin for seven days is indicated if this treatment fails.
ACT exposed pregnancies in the first trimester (n=123) indicate no adverse effects of artemisinins (and the partner drugs) on pregnancy or on the health of the fetus and neonates
>There is increasing experience with artemisinin derivatives in the second and third trimesters (over 1500 documented pregnancies). There have been no adverse effects on the mother or fetus.
>Mefloquine monotherapy has been associated with an increased risk of stillbirth
>There is no published information about the combination of amodiaquineand artesunate.
> six-dose artemether plus lumefantrine regimen has been evaluated in 125 women in the second and third trimesters in a controlled trial for the treatment of uncomplicated falciparum malaria on the Burmese-Thai border. It was well tolerated and safe, but efficacy was inferior to seven days of artesunate monotherapy.
>Clindamycin is also considered safe, but it must be given for seven days in combination with quinine. Quinine is associated with an increased risk of hypoglycaemia in late pregnancy, and it should be used only if effective alternatives are not available.
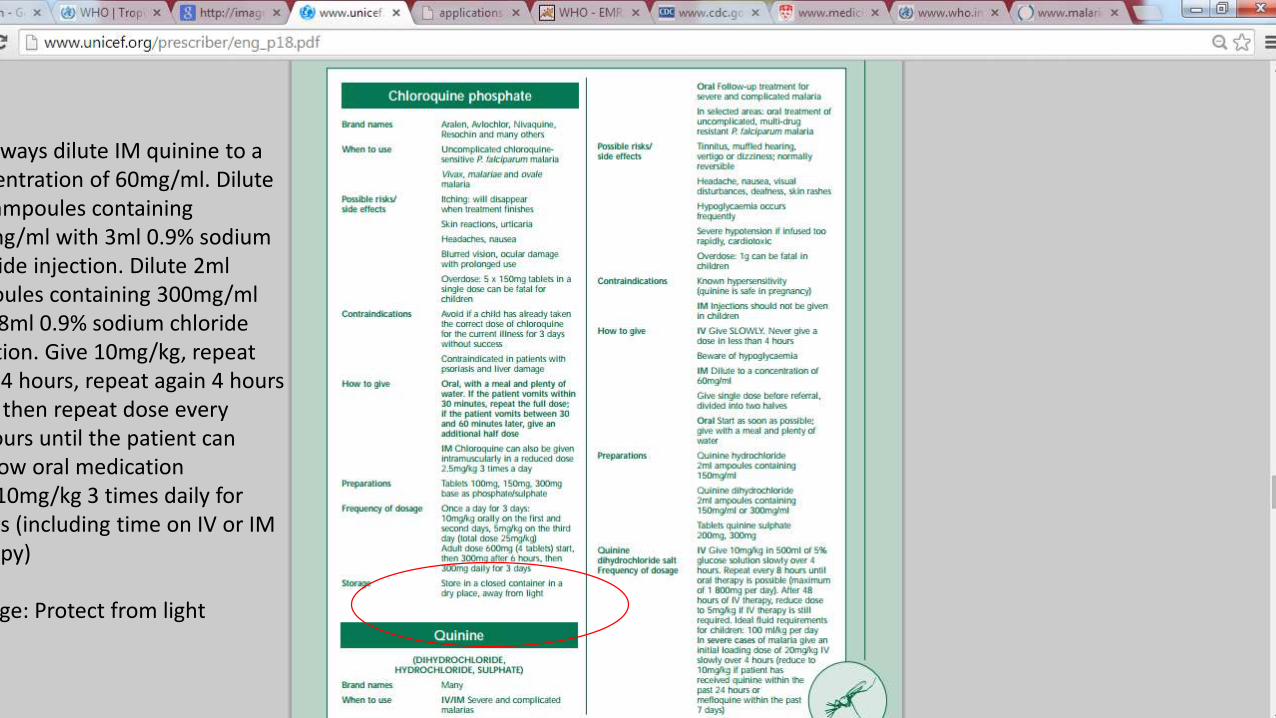
Always dilute IM quinine to aconcentration of 60mg/ml. Dilute2ml ampoules containing150mg/ml with 3ml 0.9% sodiumchloride injection. Dilute 2mlampoules containing 300mg/mlwith 8ml 0.9% sodium chlorideinjection. Give 10mg/kg, repeatafter 4 hours, repeat again 4 hourslater, then repeat dose every
hours until the patient canswallow oral medicationOral 10mg/kg 3 times daily for
days (including time on IV or IMtherapy)
Storage: Protect from light
• > Withdrawal of oral artemisinin-based monotherapies
• The continued use of oral artemisinin-based monotherapies is considered to be a major contributing factor to the development of resistance to artemisinin derivatives. WHO urges regulatory authorities in malaria-endemic countries to take measures to halt the production and marketing of these oral monotherapies, and promote access to quality-assured artemisinin-based combination therapies (ACTs).
• For oral artemisinin-based monotherapies to be effective in eliminating malaria parasites, they need to be taken as a full seven-day treatment course. However, due to the rapid clinical response – i.e. clearance of signs and symptoms within 2-3 days – most patients do not complete the full regimen. On day three, the cure rates of all artemisinin derivatives are as low as 52%, leaving the parasite exposed to sub-therapeutic blood levels.
• >2007, WHO Member States adopted World Health Assembly resolution WHA 60.18 which calls for a progressive removal of oral artemisinin-based monotherapies from markets.


Additional considerations for clinical managementCan the patient take oral medication?
Treatment is with antipyretics and, if necessary, fanning and tepid sponging.
Vomiting is common in acute malaria and may be severe. Antiemeticsare widely used
Management of seizures: patients with repeated seizures (more than two seizures within a 24h period) should be treated as for severe malaria. This suggests an overlap between the cerebral pathology resulting from malaria(seizure that is not relieving after 30 min) and febrile convulsions.
TRAVELLERS
> When within the malaria endemic country, they should be treated
according to national policy, provided this has a recent proven cure rate exceeding 90%.
> if the patient has taken chemoprophylaxis, then the same medicine should not be used for treatment.


PERSONAL PROTECTION AND SELECTIVEVECTOR CONTROL MEASURES• rainfall patterns, temperature and humidity. In many places,
transmission is seasonal, with the peak period during and just after the rainy season.
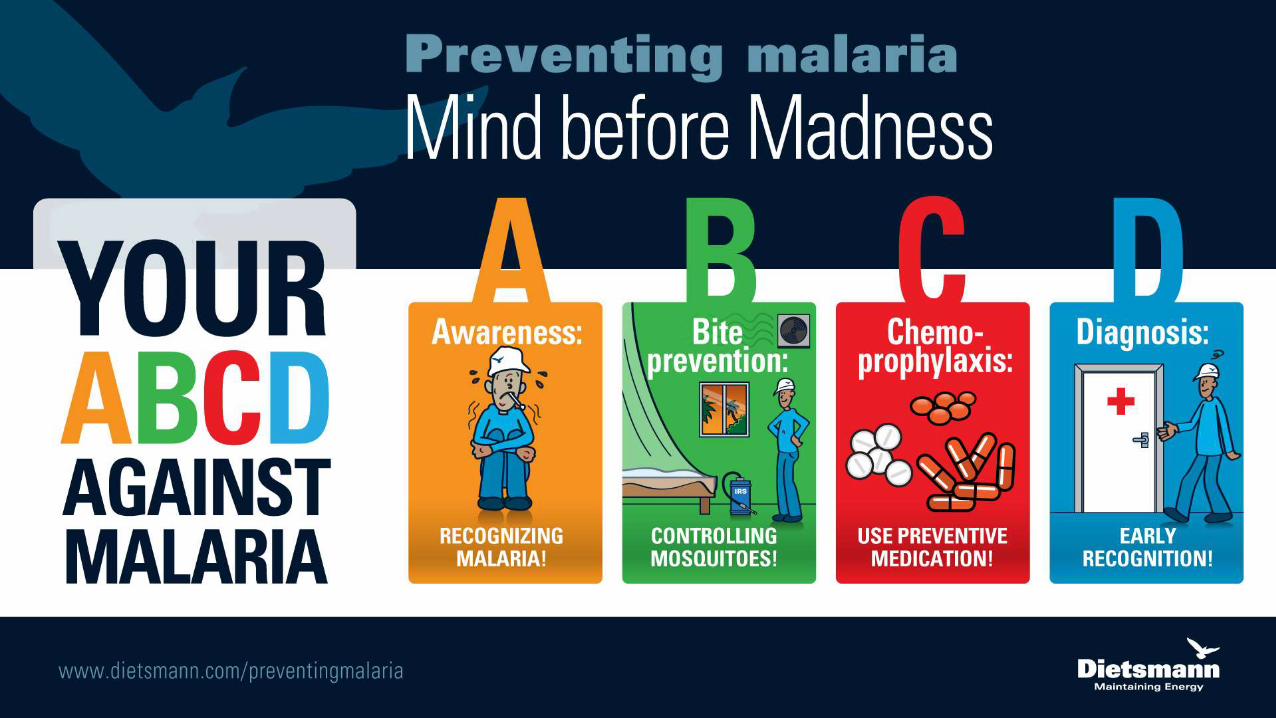
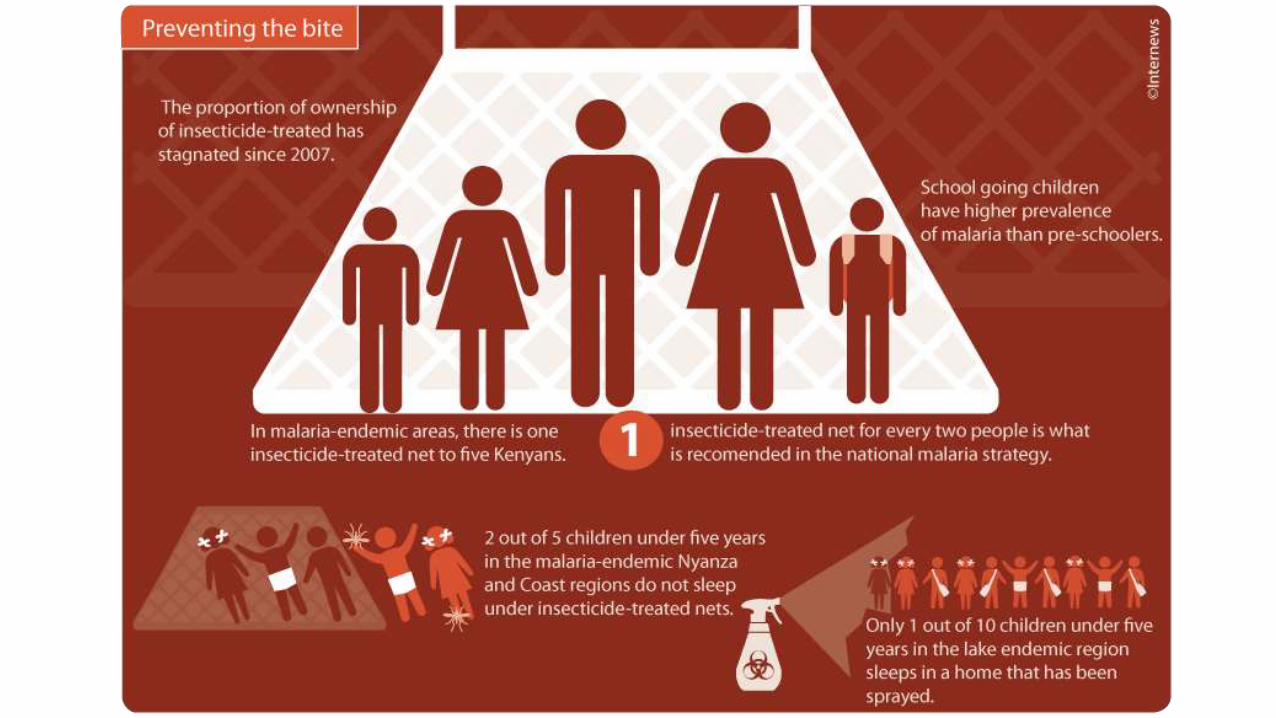
USE OF INSECTICIDE-TREATED MOSQUITO NETS
insecticide treated mosquito nets and other materials such as curtains and screens on windows and doors.
>The success of three large trials on insecticide-treated mosquito nets conducted in the Gambia, Kenya and Ghana and another one using treated curtains in Burkina Faso, have demonstrated that the use of insecticide-treated materials can reduce all-cause child mortality by about 25%.
VECTOR CONTROL-INSECTICIDE SPRAYING
>Many countries in Europe and North America have already banned the use of DDT.
> The health worker plays an enormously important role in
early diagnosis and prompt treatment of malaria cases
• WHO has initiated several key preventive and curative interventions that include:
• prompt and effective treatment with artemisinin-based combination therapies
• rolling out long-lasting insecticide-treated bed net distribution to protect pregnant women and children
• indoor residual spraying with insecticide.
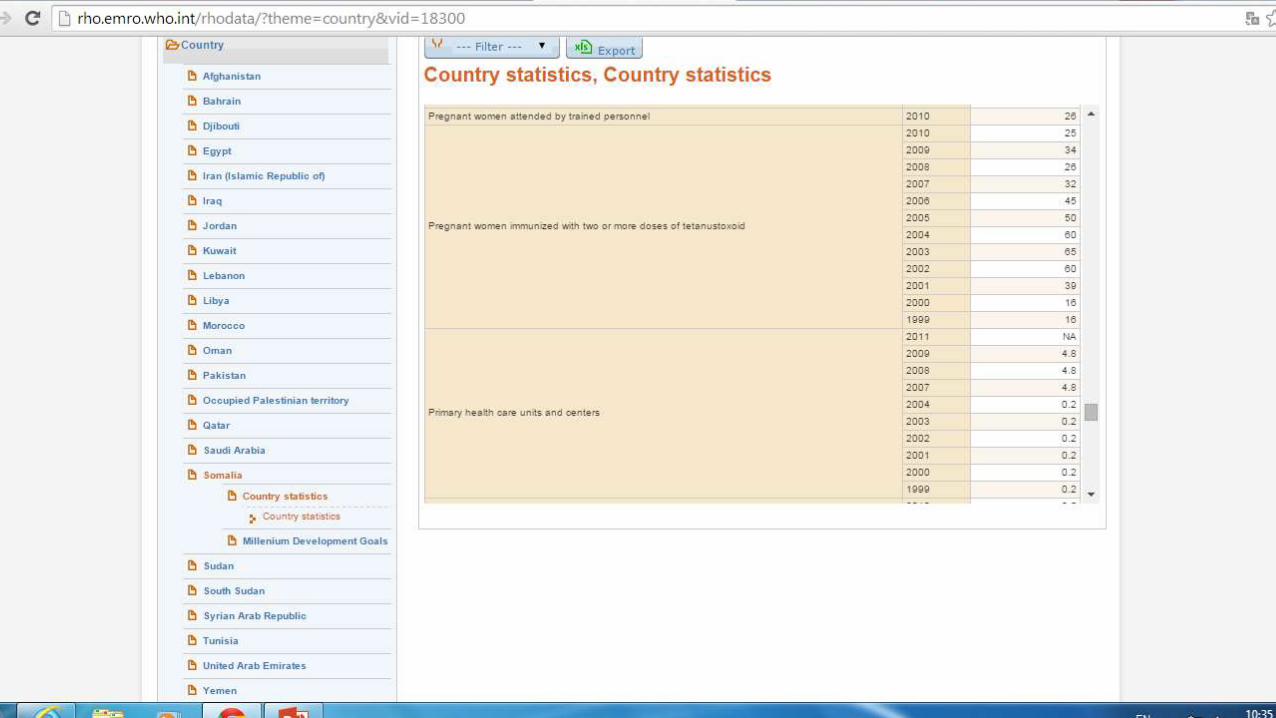
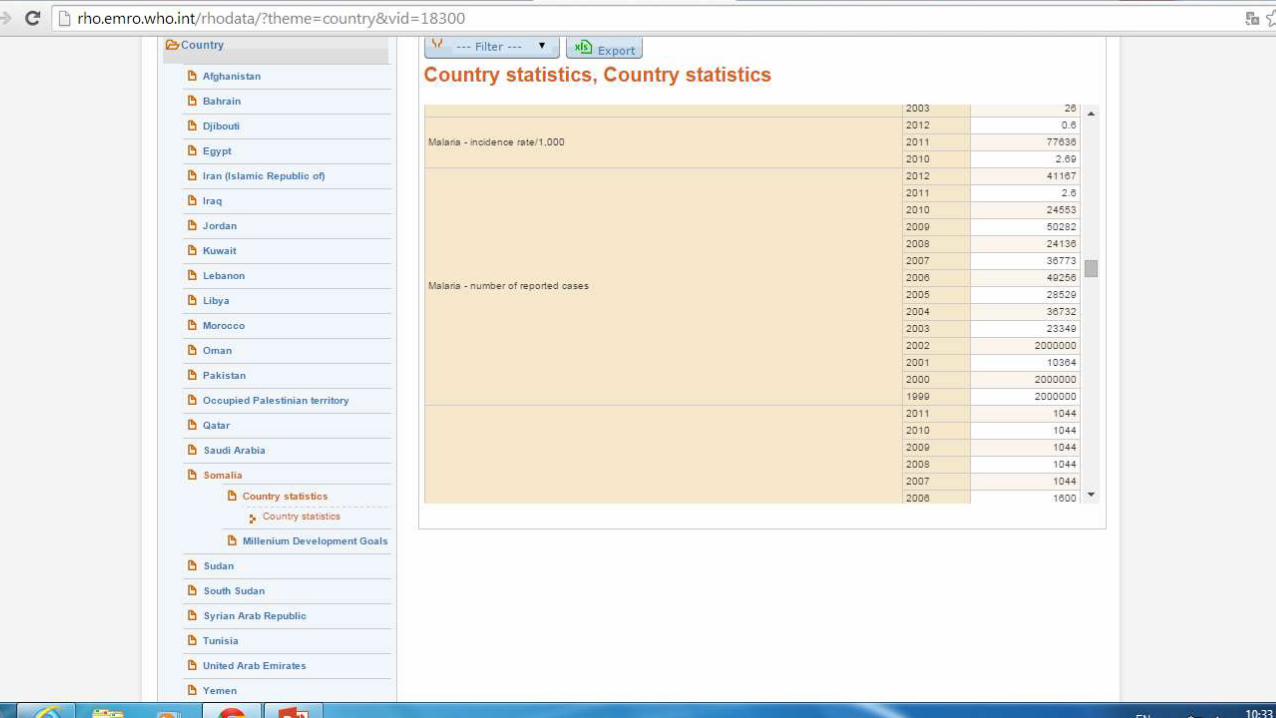
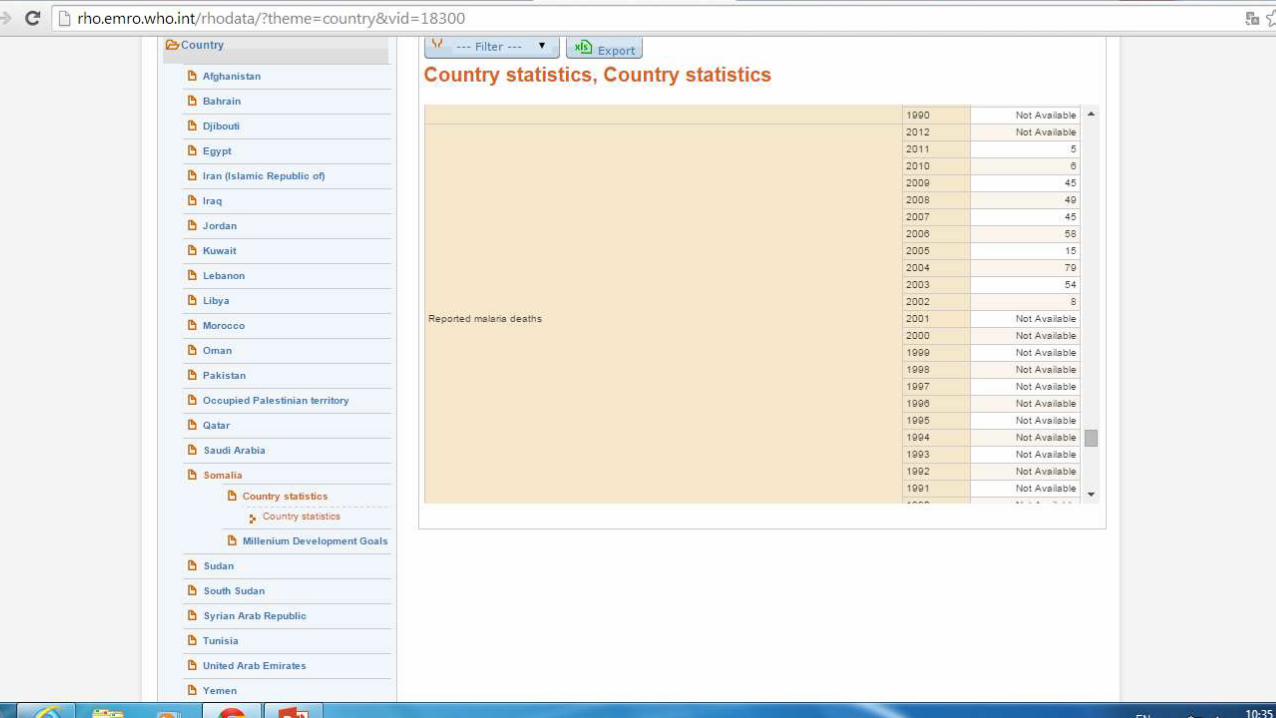
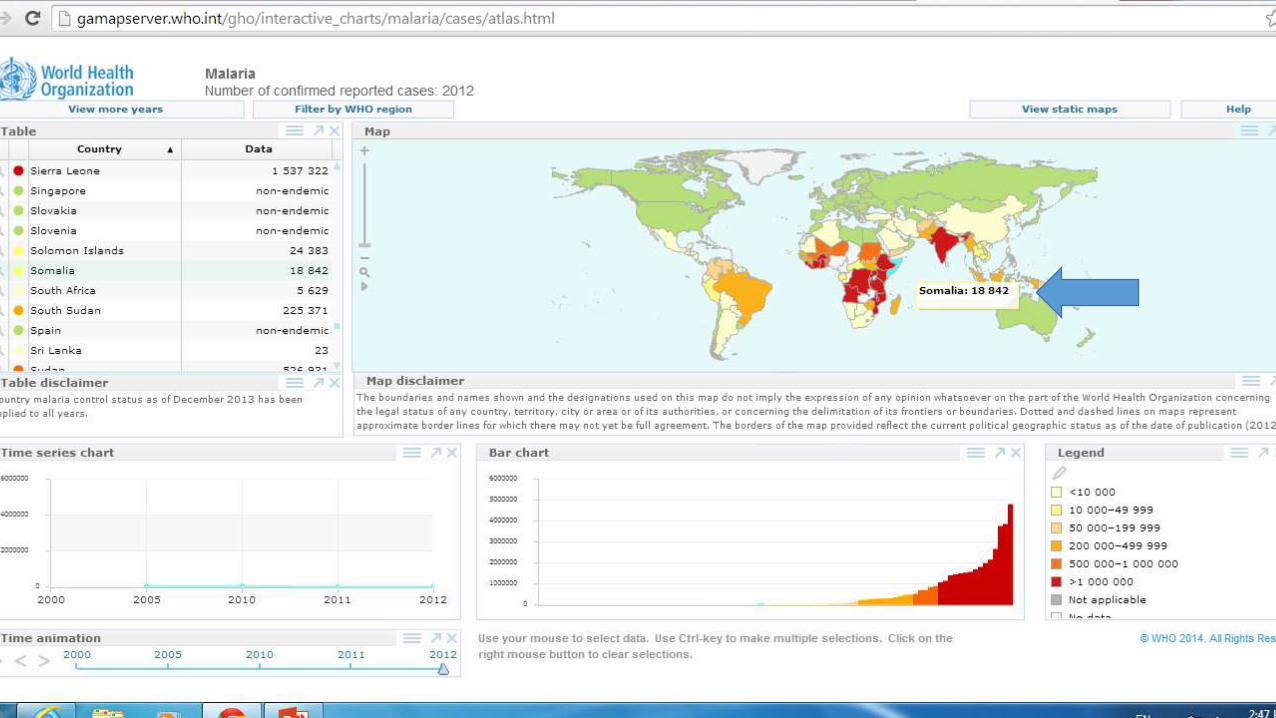
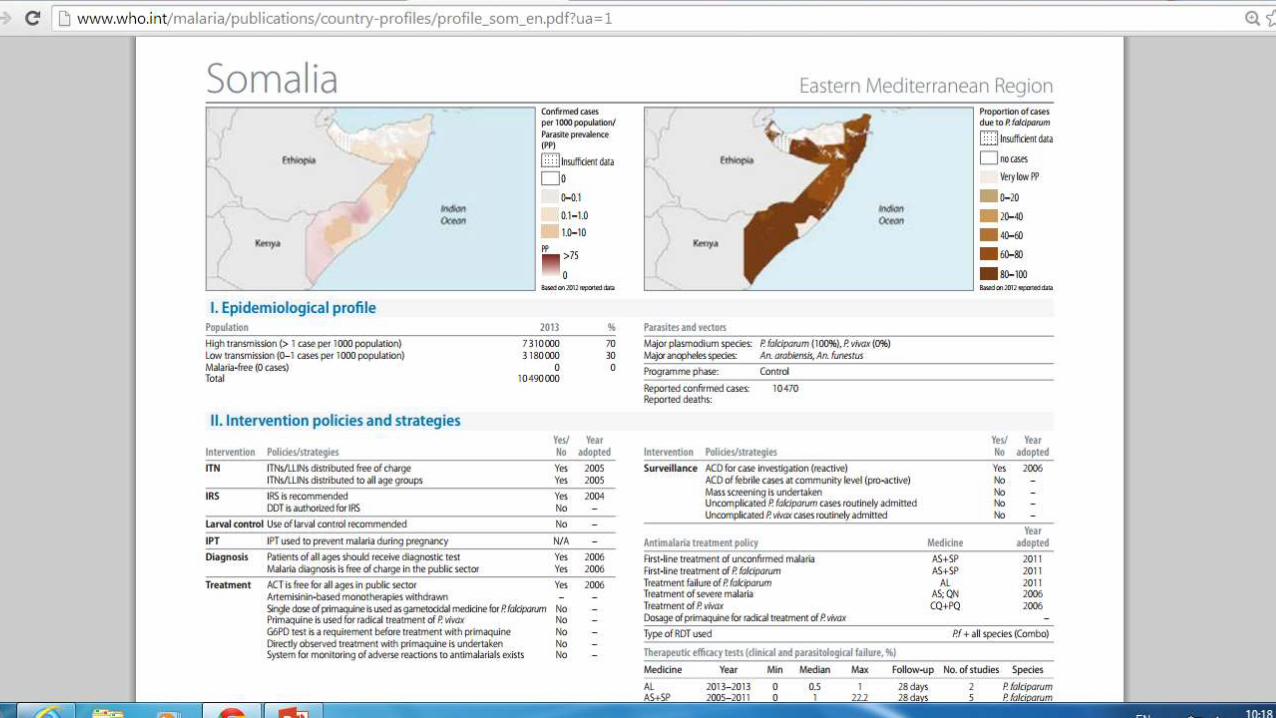
• In 2010, about 9500 malaria cases were reported in Somalia, compared to over 49 000 cases reported in 2006. This significant decrease was a result of prompt treatment, indoor household spraying campaigns and the distribution of bednets.
• UNICEF has distributed 732,000 long lasting insecticide treated nets over the last two years in malaria prone districts across Somalia. This has contributed to reduction of malaria morbidity. A recent survey indicates that distribution of nets has enhanced coverage to about 45 per cent of households.
• “In some instances the true cause of fever may not be malaria and by not getting tested for malaria, individuals can miss the opportunity to treat the real cause of fever,” says Ahmed Jama - Malaria Coordinator for the Global Fund Programme in Northwest Somalia (“Somaliland”). “Generally we see that 1 per cent of persons tested in Northwest Somalia actually have malaria while the others are suffering from other illnesses that require different treatment.