Embed Size (px)
Citation preview
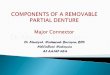
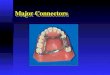
Major Connectors
(Rigidity and Support)
Requirements:
1. Rigidity and strength- for uniform distribution of forces to the abutment teeth and soft tissues.
2. Conform to and do not interfere with normal anatomic structures of the mouth- Borders
should not impinge the free gingival margins for free flow of blood supply on gingival tissues to
prevent inflammatory changes.
On dentulous areas, Upper major connectors should have a clearance of 6mm from the gingival
margins while lower major connectors should have a 3-4 mm clearance.
On edentulous areas major connectors should lie lingual to an imaginary line following the
gingival margins of the missing natural teeth. (2mm lower than the gingival margins of the teeth
adjacent to the edentulous space running parallel to the crest of the ridge.
3. They avoid food entrapment.
Sharp corners/angles should be avoided.
Border outlines should taper toward the tissues to be inconspicuous to the tongue.
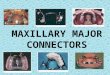
Types of Maxillary Major Connectors
1. U-shaped/Horseshoe-shaped palatal major connector - At least 8mm wide
Characteristics:
Lacks necessary rigidity across the midline for adequate cross-arch distribution
Often interferes with the tongue with speech production since it covers the anterior
portion of the palate.
Indications:
For anterior or both anterior and posterior missing teeth and RPD is supported by
natural teeth
Splinting of anterior teeth is required
Presence of torus palatinus
When patient cannot tolerate complete palatal coverage or posterior palatal bar.
2. Posterior Palatal Strap- At least 8mm in width
Very versatile. If periodontal support is compromised it can be made wider and thin to
get support from the hard palate.
When periodontal support is good and edentulous area is small it can be made
narrower but thick to maintain rigidity.
Its wide area of tissue coverage aids in retention of RPD through forces of adhesion
and cohesion.

***** Upper RPDs are subjected to the pull of gravity
Indications:
1. Short span posterior unilateral or bilateral edentulous space/s.
2. Posterior tooth supported or distal free end cases.
3. Single Palatal Bar - at least 4mm in width but thick to maintain its rigidity.
4. Palatal Plate - More than 8mm wide and therefore can be made thin.
Indications:
1. When the remaining natural teeth have lost extensive periodontal support.
2. When the residual ridges have undergone severe resorption.
3. When the anatomic form of the hard palateis flat.
4. When there are long span and bilateral posterior edentulous areas.
5. When a cleft-palate patient is treated with RPD.
6. When an RPD is considered a transitional prosthesis before a maxillary CD.
****Its large coverage makes it uncomfortable to wear than any other type
of maxillary major connector.
**** Full palatal plate – a palatal plate with extension of metal to cover the cingulum areas of
anterior teeth.
5. Modified palatal plate – a full palatal plate with a window.
Advantages:
Less metal
Less tissue coverage
Lighter weight
Indications:
Extensive class 1 and 2 with sufficient periodontal support to abutments, high alveolar
ridge and palatal vault.
6. Antero-posterior palatal connector - Crosses the midline at 90degree angle
Characteristics: anterior strap – 8-10 mm
Lateral strap – 7-9mm
Posterior strap – 5-7mm
Indications:

1. Extensive Class 1&2
2. Missing anterior and molar posterior tooth/teeth
3. Extensive Class 4 – posterior strap serves as indirect retainer
****On distal extension area – major connectors are extended up to the maxillary tuberosity area on
sharp termination which is the boundary between the metal and acrylic denture base.
Mandibular Major Connectors
1. Lingual Bar - Simplest mandibular major connector to use. First choice except for high floor of the
mouth.
Characteristics:
Half pear-shaped in cross section
Thickest inferior portion located as far below the free gingival margin at least 3-4mm.
At least 4mm in width.
2. Sublingual bar - Structurally the same as the lingual bar except for its location.
Placed on patients with well rounded lingual sulcus.
Patient’s choice
The linguoplate should not be placed higher than the middle third of the teeth
The projections cover the interproximal spaces and extend up to the contact points of the teeth.
It should have a scalloped appearancewith sharp-pointed projections.
It should have an intimate contact with the teeth.
It should be placed above the survey line of the teeth to avoid food entrapMENT
3. Linguoplate- Thin metal plate is added to the superior portion of the bar and covers the lingual surfaces of the mandibular anterior teeth
The linguoplate should be made thin as possible.The superior border of the linguoplate should cover
thecingula of the mandibular anterior teeth.
Terminal rests - Linguoplate should be supported bilaterally with incisal rests on canines or occlusal rests on mesial fossae of mandibular first premolars.

Indications
1. When the floor of the mouth is shallow or gingival recession of the mandibular anterior teeth
contraindicates the use of the lingual bar.
2. When adequate rigidity can not be obtained by the use of a lingual bar alone.
3. When the mandibular posterior teeth have been lost and the major connector must be used
to supply indirect retention on appropriately prepared anterior rest seats.
4. When periodontically weakened mandibular anterior teeth require stabilization, that is the
linguoplate is used with the swing lock-attachment
5. When extrusion of the mandibular anterior teeth must be prevented, or to avoid placing
rests on the anterior teeth.
6. When future replacement of one or more mandibular anterior teeth is anticipated.
7. When there is severe resorption of the residual ridges and a distal-extension RPD is to be
constructed
8. When a prosthesis is to be constructed to circumvent covering mandibular tori.
9. When the patient objects to a mandibular lingual bar.
• ***When there is marked spacing between mandibular natural teeth, make the plate
discontinuous to eliminate the show of Cr-Co.
4. Continuous / Kennedy Bar
Modification of lingual bar where a continuous bar is placed resting on the cingula of teeth.
6. Labial bar
Linguoplate may extend up to the posterior area.
5. CingulumBar - Least rigid