Embed Size (px)
Citation preview
Randomized trials in complex settings: Lessons learned from developing a healthcare prevention intervention for frequent emergency department visitors
Nuffield conference: Evaluation of complex care
22 June 2015
Person-centred care and patient activation
Who are we?
1
Dr Gustaf Edgren
• MD PhD, Karolinska Institutet
• Associate professor of Epidemiology, Department of Medical Epidemiology and Biostatistics, Karolinska Institutet
• Scientific advisor, Health Navigator
Magnus Liungman
• UK Country Manager Health Navigator
• MSc Business Administration, Stockholm School of Economics
• UCLA Anderson School of Management, Los Angeles
We are presenting work from a 5-year scientific collaboration
2
5 county councils (regional payors) and 12,000 participating patients in the study
All 15 acute hospitals in the 5 county councils participate
Health Navigator develops and delivers the actual intervention program
Our main messages today
3
A randomised controlled trial is often the only viable option to achieve sufficiently strong evidence – especially if you want to measure effects of interventions
Different RCT variants come with different advantages and can sometimes provide different answers
With iterative, adaptive designs, randomized trials can be used to not only develop, but also implement new interventions
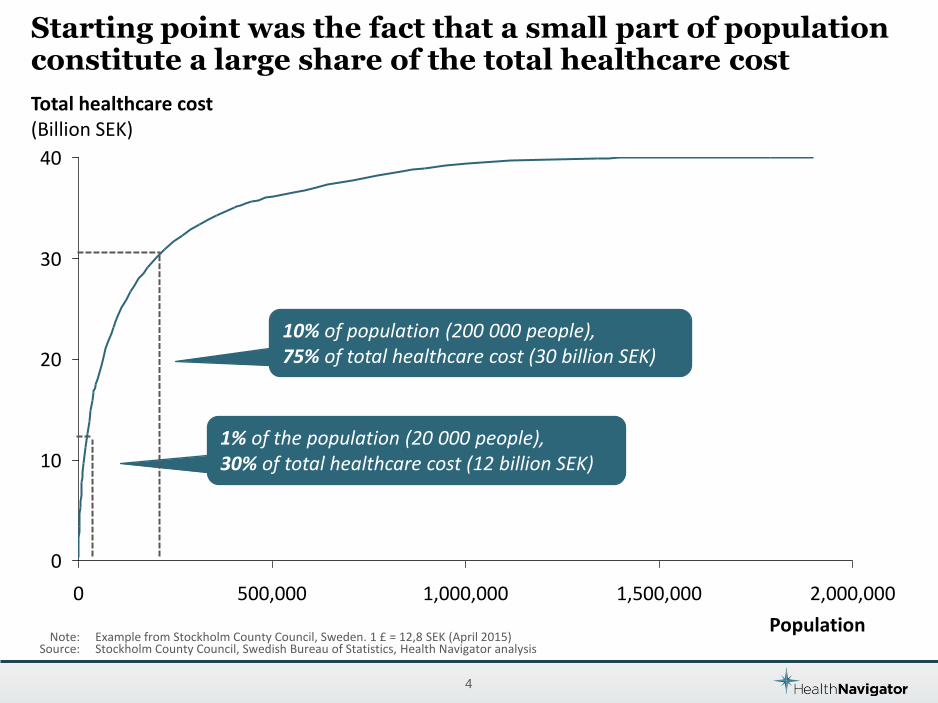
Starting point was the fact that a small part of population constitute a large share of the total healthcare cost
4
Note: Example from Stockholm County Council, Sweden. 1 £ = 12,8 SEK (April 2015) Source: Stockholm County Council, Swedish Bureau of Statistics, Health Navigator analysis
Population
10% of population (200 000 people), 75% of total healthcare cost (30 billion SEK)
1% of the population (20 000 people), 30% of total healthcare cost (12 billion SEK)
Total healthcare cost (Billion SEK)
2,000,000
0
40
20
30
10
1,000,000 500,000 1,500,000 0
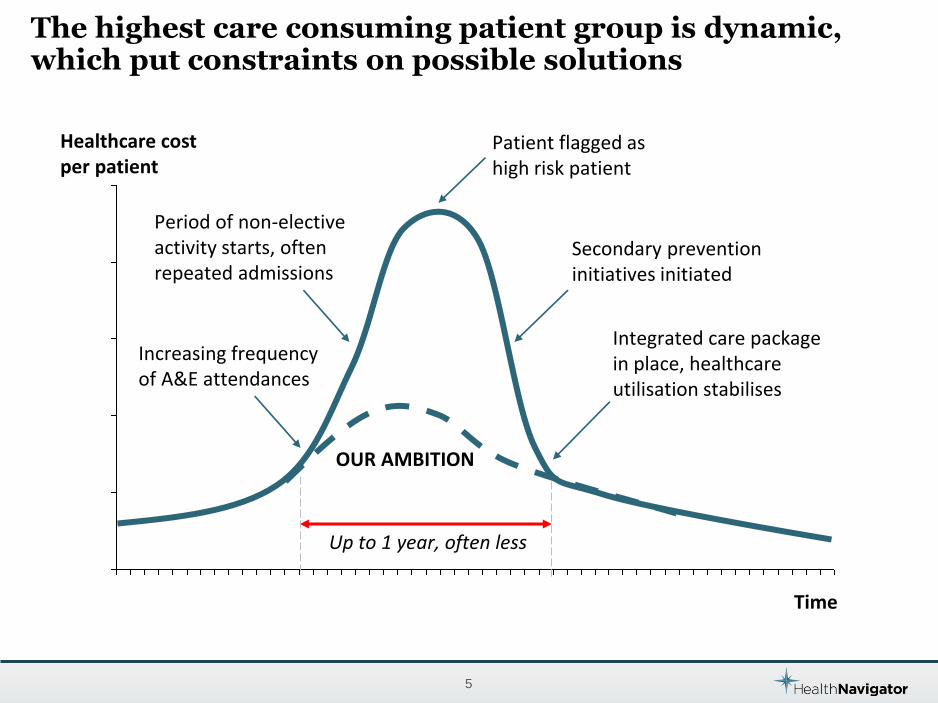
The highest care consuming patient group is dynamic, which put constraints on possible solutions
5
Increasing frequency of A&E attendances
Period of non-elective activity starts, often repeated admissions
Integrated care package in place, healthcare utilisation stabilises
Patient flagged as high risk patient
Secondary prevention initiatives initiated
Healthcare cost per patient
Time
OUR AMBITION
Up to 1 year, often less
Our aim was to develop a new effective case management intervention for frequent emergency department visitors
6
The implementation of the intervention had a high degree of uncertainty on approach and target group
7
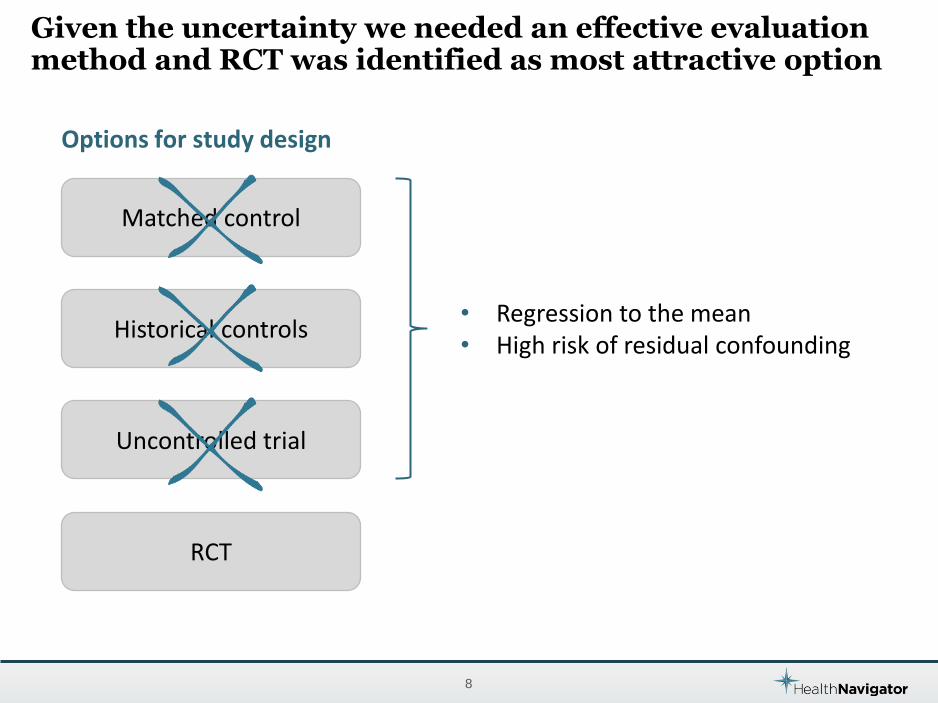
Given the uncertainty we needed an effective evaluation method and RCT was identified as most attractive option
8
Matched control
Historical controls
RCT
Uncontrolled trial
Options for study design
• Regression to the mean • High risk of residual confounding
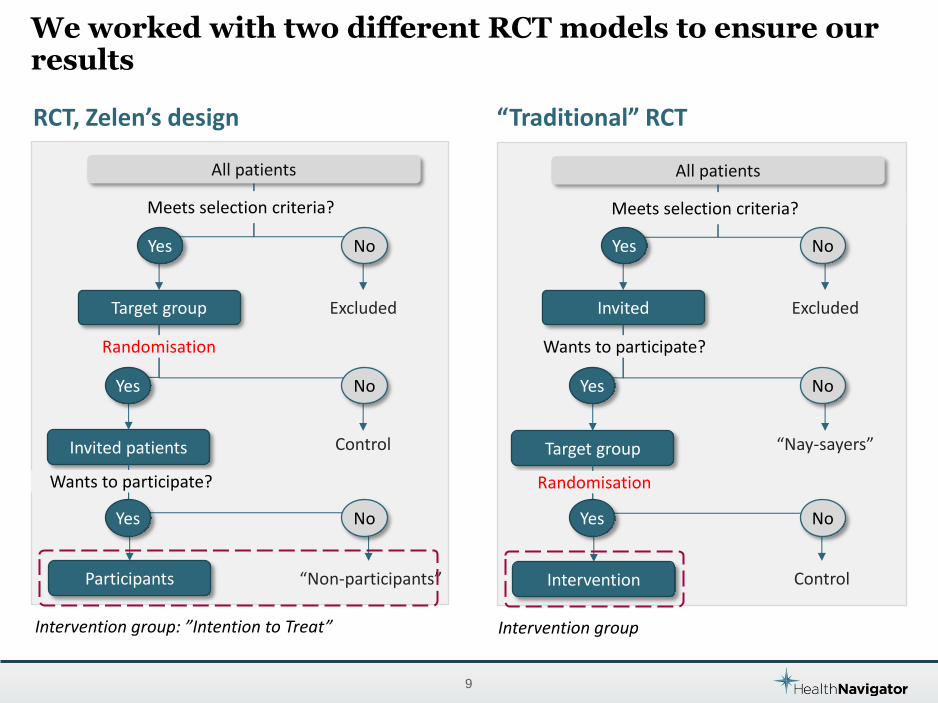
We worked with two different RCT models to ensure our results
9
All patients
Target group
Invited patients
Participants
Excluded
Control
“Non-participants”
No
RCT, Zelen’s design
Intervention group: ”Intention to Treat”
No
Yes
Yes
Meets selection criteria?
Randomisation
No
Wants to participate?
Yes
All patients
Invited
Target group
Intervention
Excluded
“Nay-sayers”
Control
No
Intervention group
No
Yes
Yes
Meets selection criteria?
No
Wants to participate?
Yes
“Traditional” RCT
Randomisation
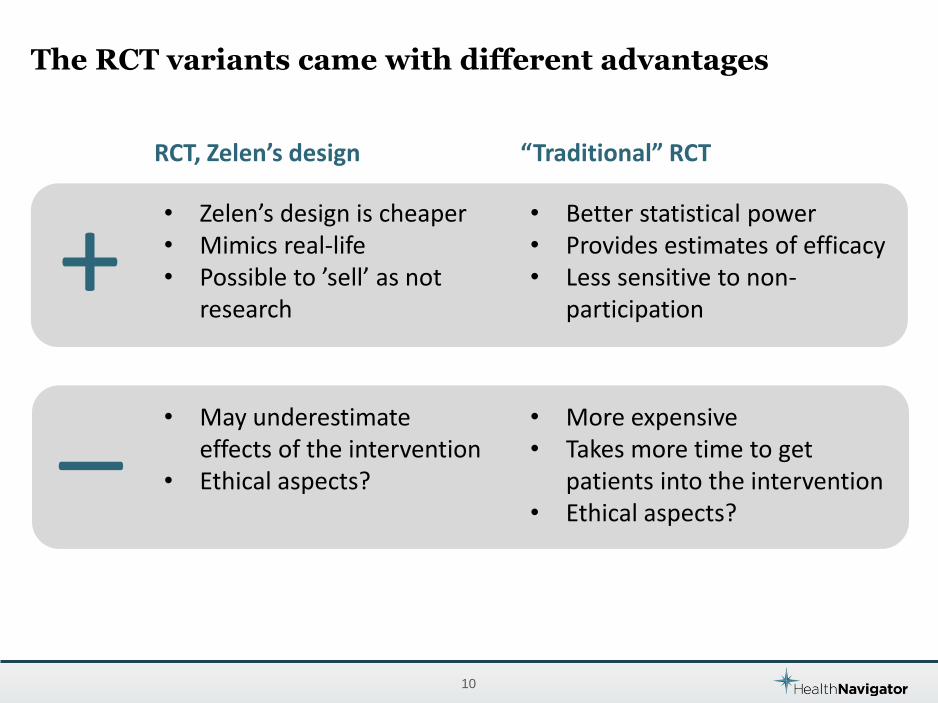
The RCT variants came with different advantages
10
• Zelen’s design is cheaper • Mimics real-life • Possible to ’sell’ as not
research
• Better statistical power • Provides estimates of efficacy • Less sensitive to non-
participation
RCT, Zelen’s design “Traditional” RCT
+ _ • More expensive
• Takes more time to get patients into the intervention
• Ethical aspects?
• May underestimate effects of the intervention
• Ethical aspects?
We used an adaptive approach during the study
11
Traditional approach Adaptive approach
VS
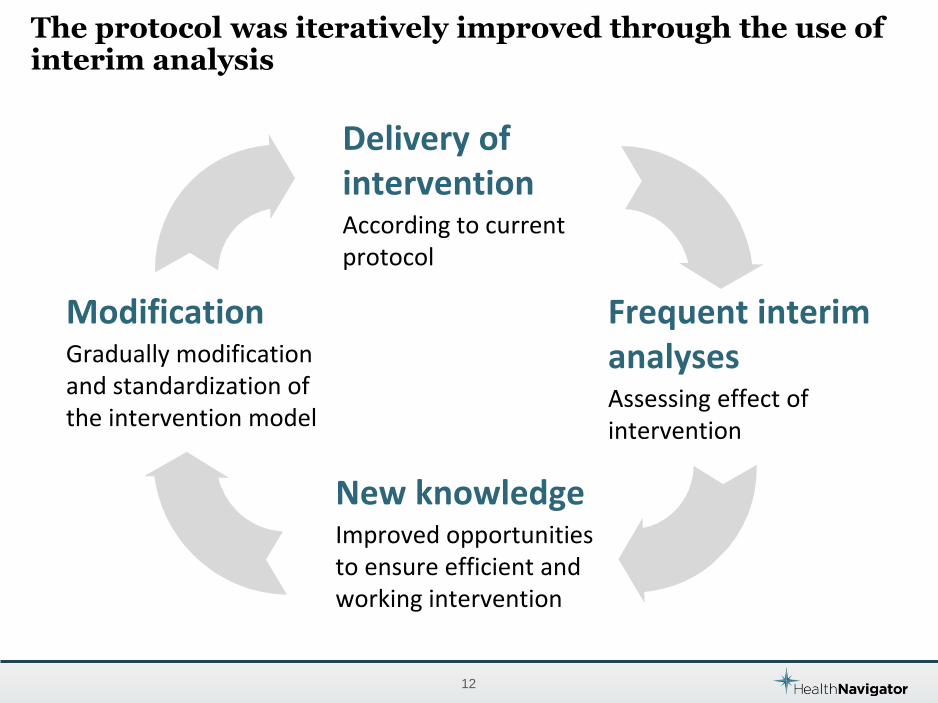
The protocol was iteratively improved through the use of interim analysis
12
Frequent interim analyses Assessing effect of intervention
New knowledge Improved opportunities to ensure efficient and working intervention
Modification Gradually modification and standardization of the intervention model
Delivery of intervention According to current protocol
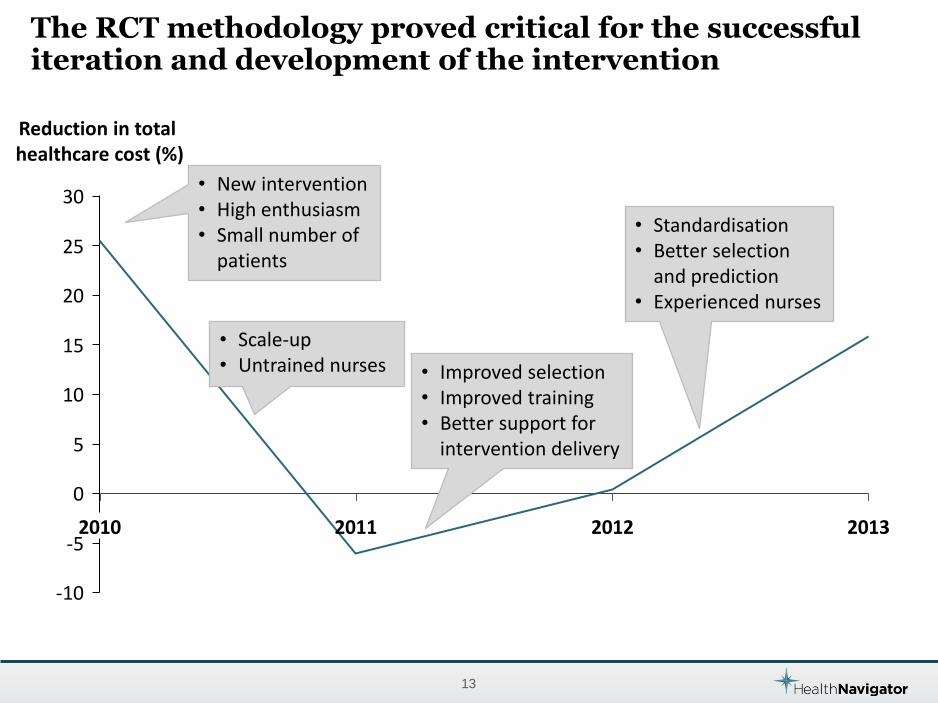
The RCT methodology proved critical for the successful iteration and development of the intervention
13
-10
-5
0
5
10
15
20
25
30
2010 2011 2012 2013
Reduction in total healthcare cost (%)
• Improved selection • Improved training • Better support for
intervention delivery
• Standardisation • Better selection
and prediction • Experienced nurses
• New intervention • High enthusiasm • Small number of
patients
• Scale-up • Untrained nurses
Today, five years later…
14
• The case management intervention is permanently implemented in Stockholm
• Reducing A&E admissions with 2-4% on system-wide level • Readmissions within 30 days have declined with 15-20%
• Based on the results achieved in Sweden, Denmark has taken a national decision to implement the intervention
• It will be implemented as a huge RCT that starts now and will go on at least until 2018
• In UK we are now starting up RCTs to test and improve the interventions in several CCGs
To summarize…
15
A randomised controlled trial is often the only viable option to achieve sufficiently strong evidence – especially if you want to measure effects of interventions
Different RCT variants come with different advantages and can sometimes provide different answers
With iterative, adaptive designs, randomized trials can be used to not only develop but also implement new interventions