Embed Size (px)
Citation preview
Life-Threatening Allergies
in the School Setting
including
Epinephrine Injection Training
Prepared by the South Portland School Department
Health Services
Developed- August 2011 Updated November 2014
COMPETENCY
This power point and concluding competency test will satisfy the knowledege portion of life-threatening allergies in the school setting and Epinephrine Injection medication training.
To complete the medication skills training, you will need to demonstrate your EpiPen® and Auvi-Q™ administration skills which will be verified and documented by the school nurse.
Presentation Goals
Provide basic understanding of life-threatening allergies: definition, common allergens, treatment
Review the significance of life-threatening allergies in the school setting and avoidance management
Explain anaphylaxis: definition, signs & symptoms and treatment
Explain Emergency Plan and Medications used for allergic reactions and treatment plan
Describe technique for administering EpiPen® and medication
School personnel are encountering more children
with life-threatening allergies.
18% increase from 1997-2007!
AND
Recent research study presented in 2010 found
significant food allergy knowledge gaps exist
among school and child care providers.
Source: Study by researchers at Children’s National Medical Center, Johns Hopkins and Safe@School Partners cited in: Food Allergy News
Special Issue for School Nurses, Spring 2011
Food Allergies are Rising!
Study findings…
Overall knowledge was fair. In several areas, knowledge was poor!
68% were unaware that hand sanitizer is not effective in removing food residue after eating.
63% incorrectly believed that epinephrine is an extremely dangerous drug.
78% were unaware that a 2nd dose of epinephrine could be safely administered if allergic symptoms did not improve 10 minutes after the first dose.
42% incorrectly responded that Benadryl® or other antihistamine should always be the first medication given to a student experiencing a food allergic reaction.
C. A. R. E.
COMPREHENDFood Allergy Basics
AVOIDThe Allergen
RECOGNIZEAllergic Reactions
ENACTEmergency Plan
Source: How to C.A.R.E for Students with Food Allergies-What Every Educator Should Know
Visit www.allergyready.com for more information
C.A.R.E. for Kids with Food Allergies
COMPREHEND!
Food Allergy
Basics
C
What is a Food Allergy?
A food allergy is an abnormal response by the immune system to an otherwise harmless food protein.
When the food is eaten, the immune system incorrectly identifies the food protein as a “threat”and attempts to attack it.
Immune system OVER-REACTS, releasing chemicals into the blood…causing an allergic reaction.
Food Allergies vs. Intolerance
Food allergies are different than food intolerances and other allergies (i.e. cat, pollen).
Seasonal and Animal Allergies while uncomfortable, usually do not cause major medical problems because the immune system reactions are more limited, such as sneezing and watery eyes.
Food intolerances are the body’s inability to process or digest a particular food, such as lactose, celiac. Immune system is not involved.
What foods cause allergic
reactions?People can be allergic to almost any food, but most
food allergy reactions are caused by 8 foods:
Peanuts
Eggs
Soy
Fish Shellfish
Wheat
Tree Nuts
Milk
Source: * Food Allergy Network, Five Steps Forward for Food Allergy, 2008
Other Allergens:
Insect Stings
Latex
Medications (penicillin, sulfa drugs, etc.)
Exercise-induced (less common)
Common Causes cont.
Food Allergy Facts
The food does not have to be ingested to cause a reaction; skin contact or inhalation of the protein can sometimes trigger reactions.
Some food allergies (milk, soy, egg, wheat) can be “outgrown,” but most food allergies are life long.
Peanut and Tree Nut allergies are more likely to produce a life-threatening allergic response.
Even trace, not visible, amounts can cause a reaction.
1. There is NO cure for life-
threatening allergies.
2. Strict avoidance of allergens is
ONLY way to prevent allergic
reactions!
Treatment
AVOID!
The Allergen
A
AVOID Know which students have life threatening allergies
Review alternatives for lessons or celebrations involving food
Check labels on products: art supplies, hand lotions, etc
K-5 level Classroom snack restrictions
Student education lessons: hand washing, food sharing
Parent notifications home
Nut Restricted cafeteria tables
Prevent cross-contact concerns Hand washing to remove food residue
Read food labels
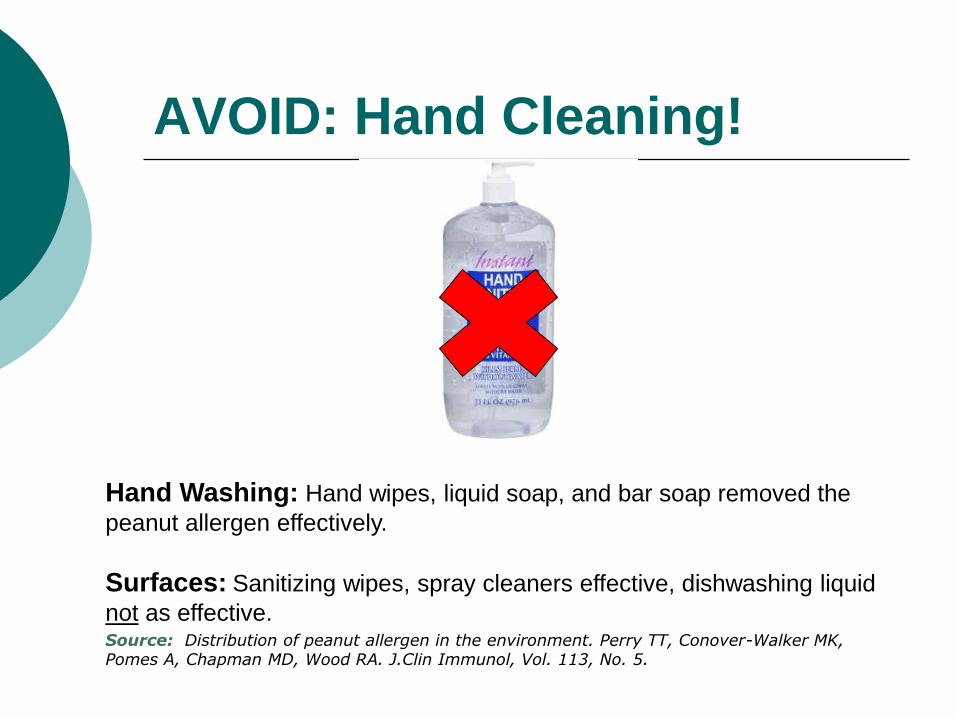
AVOID: Hand Cleaning!
Hand Washing: Hand wipes, liquid soap, and bar soap removed the
peanut allergen effectively.
Surfaces: Sanitizing wipes, spray cleaners effective, dishwashing liquid
not as effective.Source: Distribution of peanut allergen in the environment. Perry TT, Conover-Walker MK, Pomes A, Chapman MD, Wood RA. J.Clin Immunol, Vol. 113, No. 5.
AVOID: Read Food Labels!
http://www.foodallergy.org/document.doc?id=133
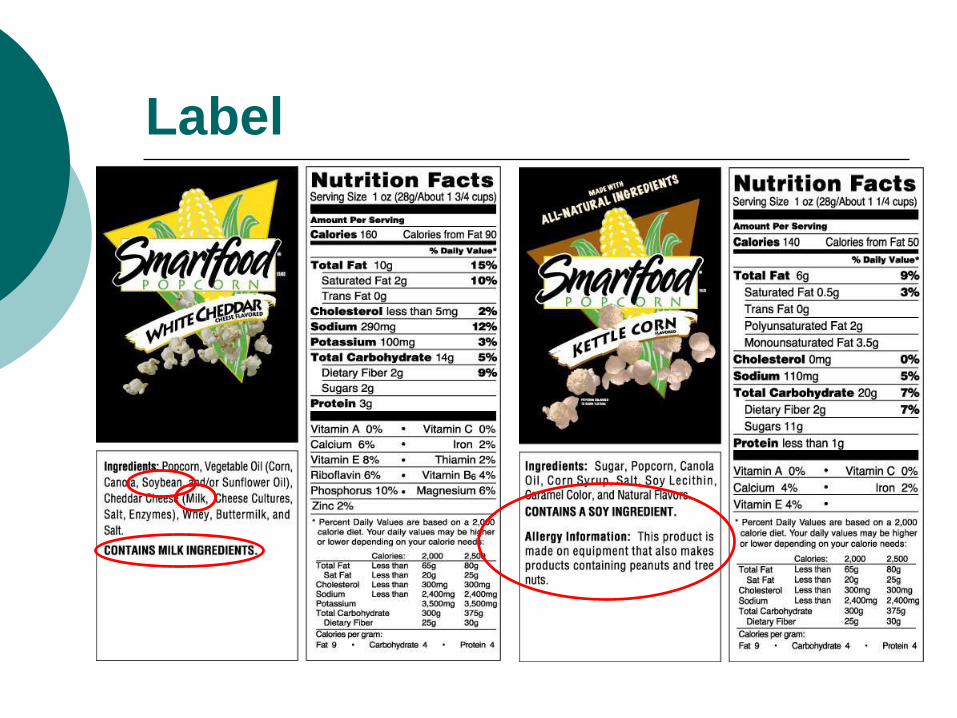
Label
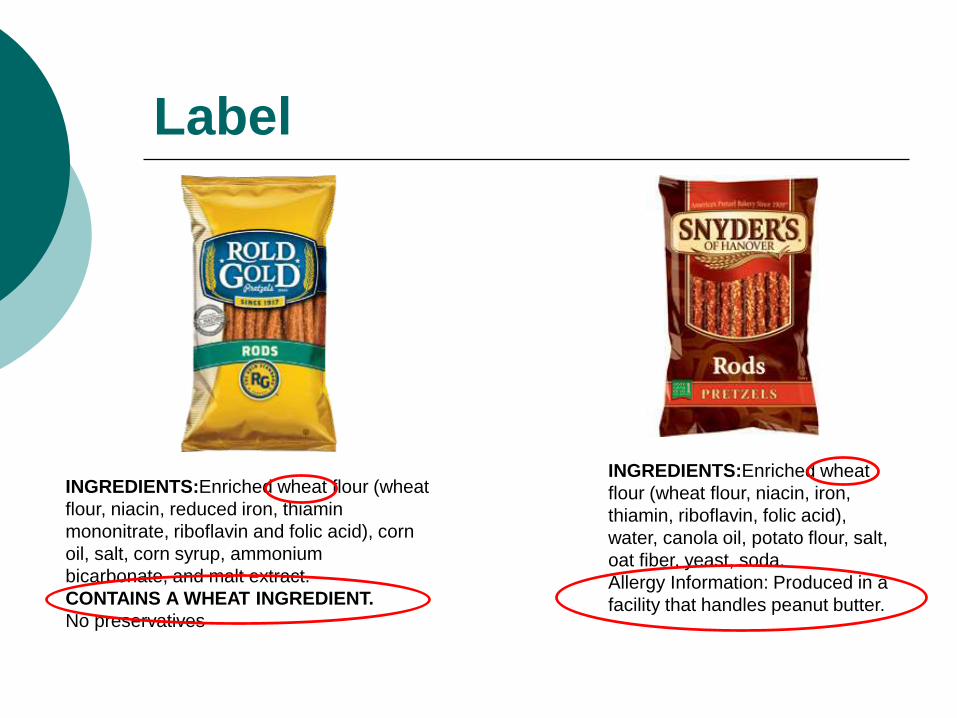
INGREDIENTS:Enriched wheat
flour (wheat flour, niacin, iron,
thiamin, riboflavin, folic acid),
water, canola oil, potato flour, salt,
oat fiber, yeast, soda.
Allergy Information: Produced in a
facility that handles peanut butter.
Label
INGREDIENTS:Enriched wheat flour (wheat
flour, niacin, reduced iron, thiamin
mononitrate, riboflavin and folic acid), corn
oil, salt, corn syrup, ammonium
bicarbonate, and malt extract.
CONTAINS A WHEAT INGREDIENT.
No preservatives

Food Allergy Deaths do occur…
Majority are from accidental ingestion of a
food allergen.
January 4, 2012Chesterfield, Virginia
A 7 year old student with a peanut and egg allergy died at school of an accidental peanut ingestion.
TAKE HOME POINTS!
Strict avoidance is the only way to prevent allergic reactions.
Check all food items used in the classroom and notify parents in advance.
Handwashing is best.
RECOGNIZE!
Signs & Symptoms
of Allergic Reactions
R
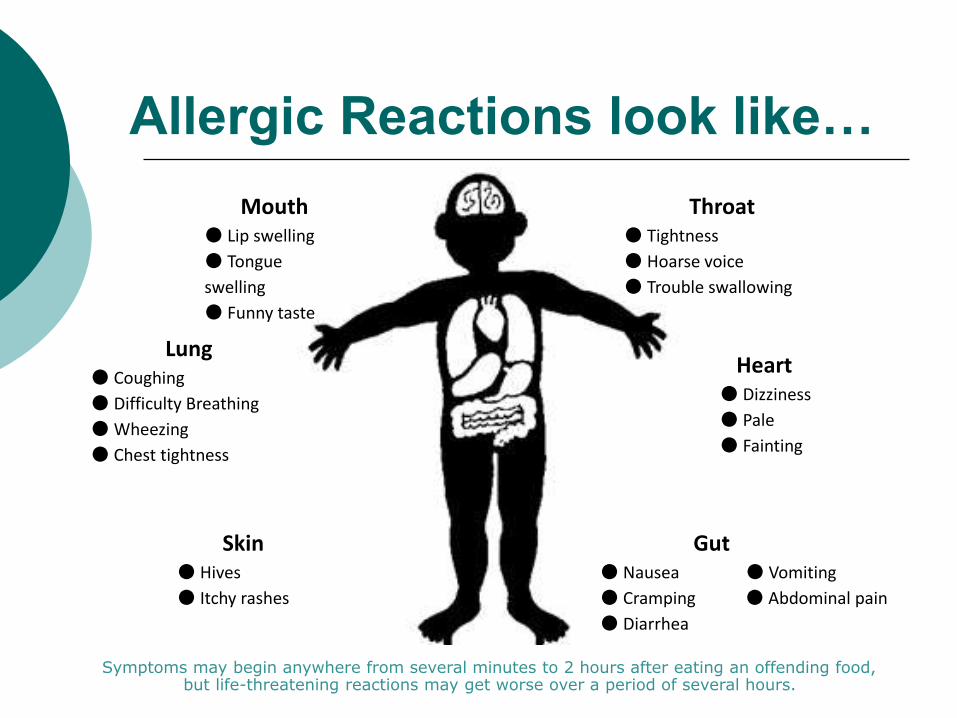
Allergic Reactions look like…
Gut ● Nausea ● Vomiting
● Cramping ● Abdominal pain
● Diarrhea
Heart ● Dizziness
● Pale
● Fainting
Lung ● Coughing
● Difficulty Breathing
● Wheezing
● Chest tightness
Throat ● Tightness
● Hoarse voice
● Trouble swallowing
Mouth● Lip swelling
● Tongue
swelling
● Funny taste
Skin ● Hives
● Itchy rashes
Symptoms may begin anywhere from several minutes to 2 hours after eating an offending food, but life-threatening reactions may get worse over a period of several hours.
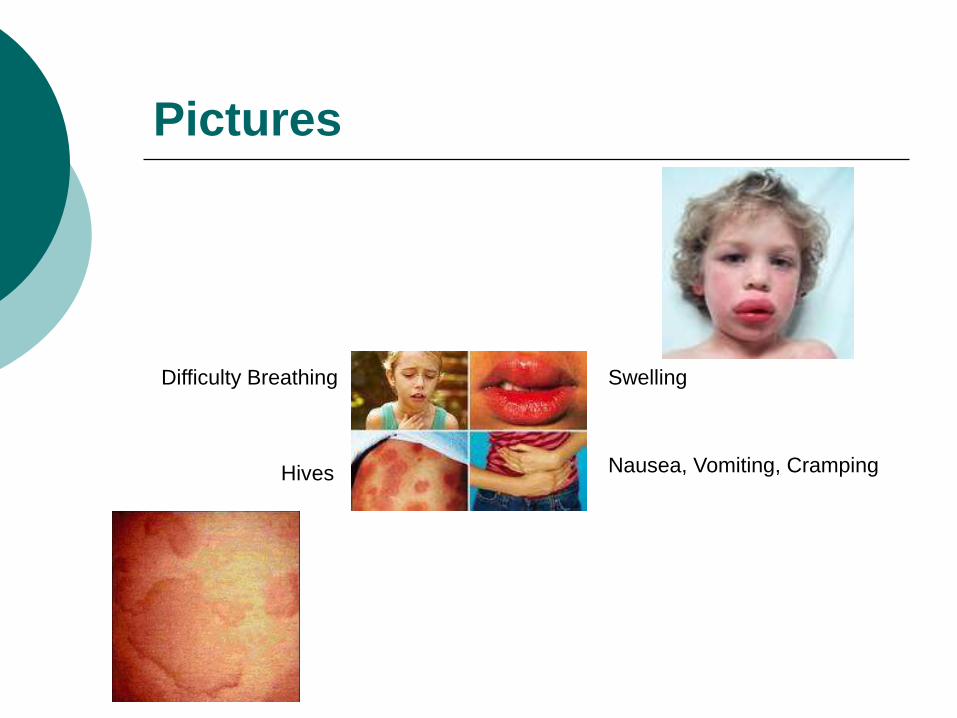
Pictures
Difficulty Breathing
Hives
Swelling
Nausea, Vomiting, Cramping
What is Anaphylaxis?
Collection of symptoms often affecting multiple body systems
Can occur immediately or delayed 2-4 hours following allergen exposure
History of asthma and eczema increase the chance of anaphylactic reactions
Each exposure has the potential to cause anaphylaxis.
Cannot predict what type of allergic symptoms a student may have after allergen exposure.
A serious allergic reaction that is rapid in onset and may cause death.
TAKE HOME POINTS!
EVERY allergic reaction is different.
Signs of Allergic reactions can Be delayed up to 2 hours after ingestion
Have mild symptoms that quickly progress to severe symptoms
Have immediate severe symptoms of anaphylaxis
A student experiencing anaphylaxis may show NO skin symptoms.
ENACT!
Emergency Plan
E
ENACT Emergency Plan!
Follow emergency plan
Follow student’s food allergy action plan.
Copy with Classroom Teacher
Copy in Medication Envelope
Administer Epinephrine, if necessary
Always Call 911 if Epinephrine is given.
Emergency Plan Ask if there has been exposure to known allergens. If in doubt,
treat as allergic reaction.
Adult to stay with student.
Immediately access Emergency Allergy Action Plan, Benadryl® and Epinephrine by contacting School Nurse (or Secretary if Nurse is unavailable).
Administer emergency medication(s) per Allergy Action Plan, note time given.
Call 911, tell operator Epi was given and request ambulance with Epi. Due to possible delayed wave of symptoms in 2-4 hours, emergency medical care must be obtained (includes ambulance and hospital care)!
Notify parent/guardian.
Monitor status of symptoms.
Administer 2nd dose of epinephrine in 5 minutes or more if symptoms persist or recur.
Remain with student while awaiting ambulance transport to hospital.
If severe reaction, keep student lying on back with legs raised.
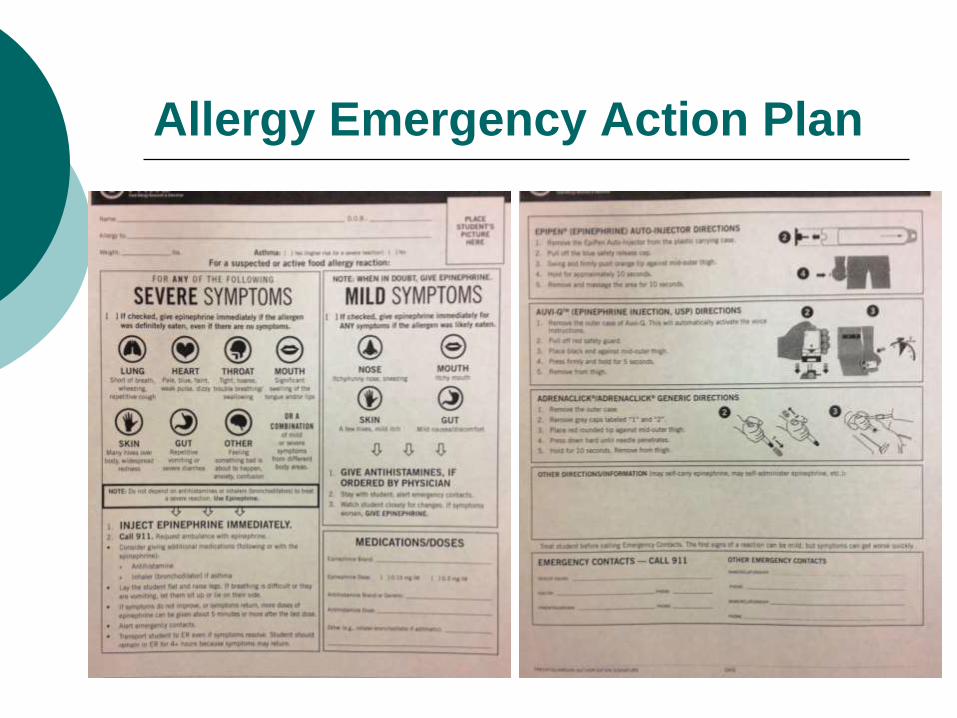
Allergy Emergency Action Plan

Treatment
Medication can help treat and stop
allergic reactions.
Early recognition & treatment
saves lives!
Benadryl®
Use: to treat only MILD allergic symptoms, cannot stop anaphylaxis!
Dose: 12.5mg-50mg depending on weight. Prescribed dose indicated on Allergy Action Plan
Action: antihistamine
Forms: capsule, liquid, dissolving tablet
Common Side Effects: headache, drowsiness, dizziness, dry mouth
Epinephrine
Use: 1st line drug for any severe symptoms after suspected or known allergen ingestion/contact
Is a naturally occurring hormone in our bodies, also known as adrenaline
Dose: .15mg (Epi ) or .3 mg (Epi) depending on weight. Prescribed dose indicated on Allergy Action Plan
Action: reverses anaphylaxis effects
Common Side Effects: increased heart rate, heart pounding sensation, sweating, nausea/vomiting, dizziness, shakiness, headache nervousness

Epinephrine Delivery Devices
EpiPen®(yellow)
EpiPen Jr.®(green)
Auvi-Q Jr™(blue)
Auvi-Q™(red)
TAKE HOME POINTS!
Follow Allergy Action Plan for instructions-BUT… when in doubt, it is better to give epinephrine & seek medical attention!
Give Epi & then Call 911
Fatalities occur when epinephrine is withheld or delayed!
Be prepared…every second counts.
EPI
ADMINISTRATION
EpiPen® Administration Steps
Flip open cap on carrier tube.
Slide EpiPen® out of tube.
Grasp unit with fist, orange tip pointing down.
Pull off blue safety release cap with other hand.
Swing and firmly push orange tip into outer thigh until it “clicks” so that unit is at 90° angle to thigh.
Hold firm against thigh for 10 seconds to deliver drug.
Remove tip from leg (protective cover extends to cover needle) and massage injection site for 10 seconds.
Keep used EpiPen and give to EMS/paramedic.
Note: The pen can inject through clothing.
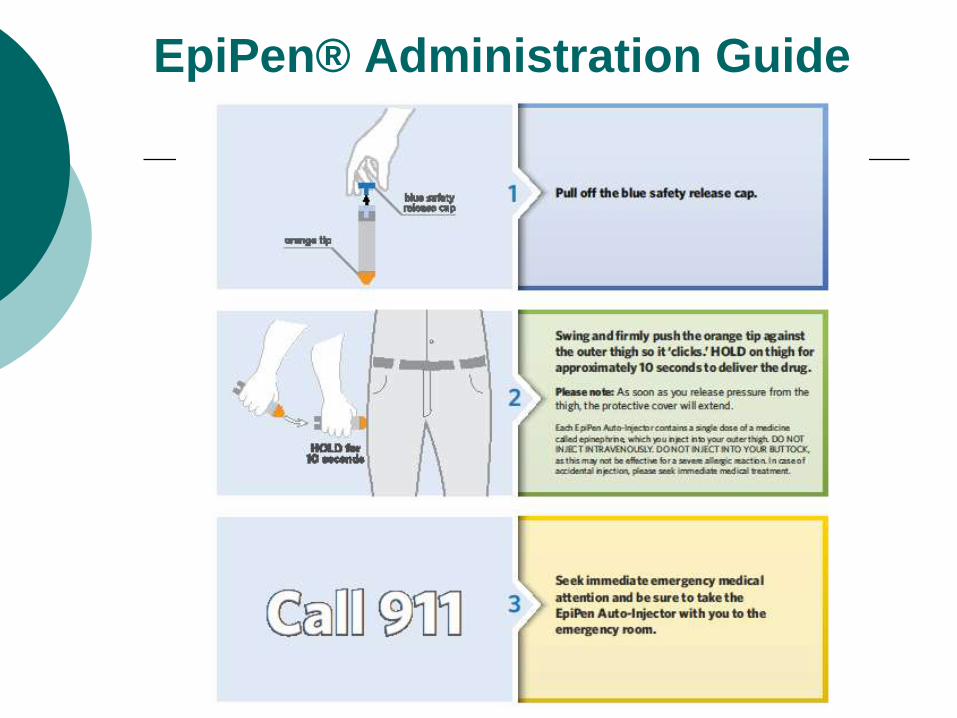
EpiPen® Administration Guide
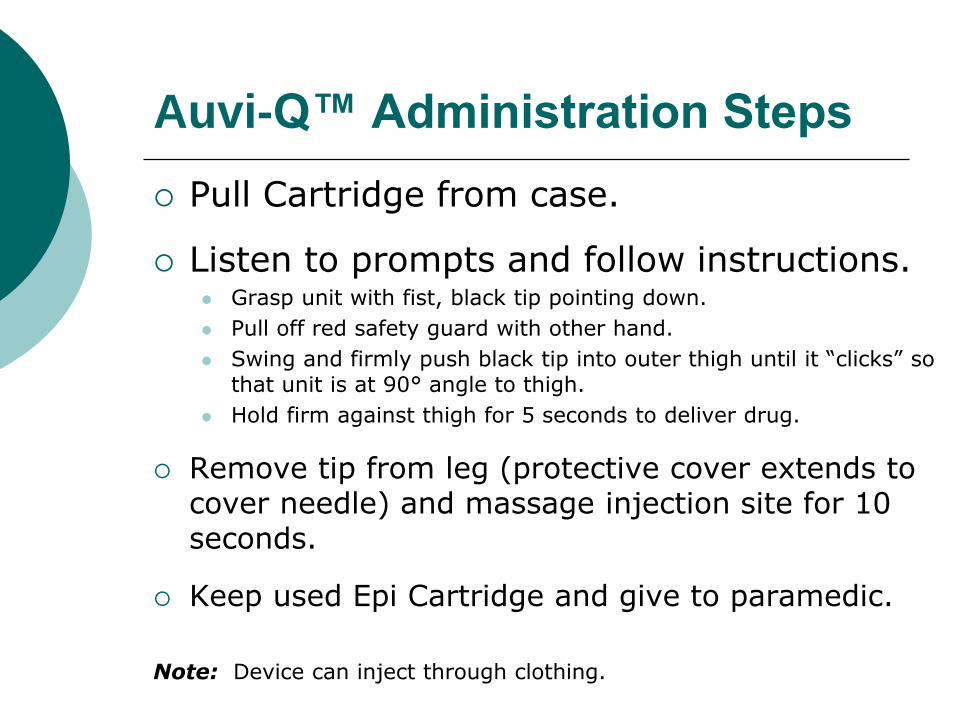
Auvi-Q™ Administration Steps
Pull Cartridge from case.
Listen to prompts and follow instructions. Grasp unit with fist, black tip pointing down.
Pull off red safety guard with other hand.
Swing and firmly push black tip into outer thigh until it “clicks” so that unit is at 90° angle to thigh.
Hold firm against thigh for 5 seconds to deliver drug.
Remove tip from leg (protective cover extends to cover needle) and massage injection site for 10 seconds.
Keep used Epi Cartridge and give to paramedic.
Note: Device can inject through clothing.
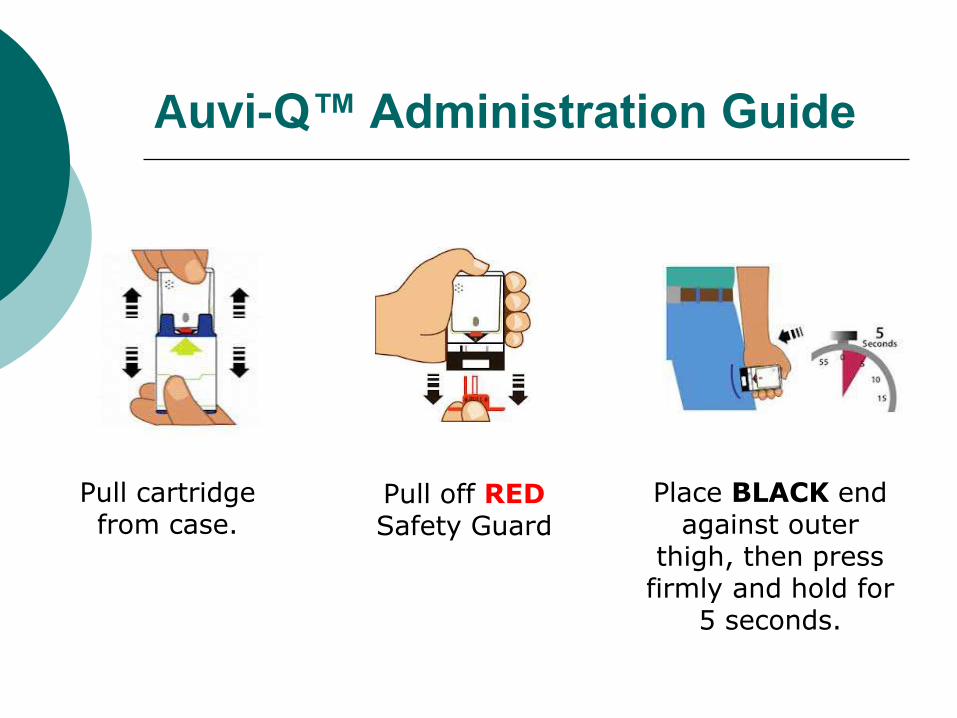
Auvi-Q™ Administration Guide
Pull cartridge from case.
Pull off REDSafety Guard
Place BLACK end against outer
thigh, then press firmly and hold for
5 seconds.
Demonstration Videos
EpiPen® Video link
http://www.epipen.com/professionals/tools/video
Auvi-Q™ Video link
http://www.auvi-q.com/demonstration-video
Right Person: verify student’s name on Allergy Action
Plan and prescription label (if provided)
Right Medication: verify the medication name
against the medication prescribed on the Allergy Action Plan
Right Dose: verify the medication dose as prescribed on
the student’s Allergy Action Plan
Right Time: immediate administration based on allergic
reaction symptoms
Right Route: Epi- injection, Benadryl®- oral
Emergency Medications: 5 Rights
Documentation
Every dose of medication givenneeds to be documented with the:
DATE, TIME, INITIALS
of person administering the medication on the student’s
medication envelope(s).

ALL SPSD staff play
an important role in the
food allergy
management team!
New Legislation!
School Epinephrine Act
The law uses financial incentives to encouragestates to require schools to keep “stock”epinephrine on hand in schools -- meaningepinephrine that is not prescribed to a specificstudent but can be used for any student orstaff member in an anaphylactic emergency. Italso provides incentives for schools to ensureschool personnel are trained to use it.
TAKE HOME POINTS!
School Staff
Need to C.A.R.E. Signs & symptoms of allergic reactions
How to respond to allergic reactions
They are often 1st responders to students in distress!
Questions?
Test
Written Post-test: 80% passing rate required
Demonstate Epinephrine administration skill
THANK YOU!
Michelle Arpin, RNFrank I. Brown Elementary School
South Portland School Department
799-5196

Food Allergy Research & Eductation(www.foodallergy.org)
Food Allergy Initiative (www.faiusa.org)
Sources
Sources cont.
Sicherer SH, Muñoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. 2010.
U.S. Census Bureau.State and County QuickFacts. 2010. Retrieved from
http://quickfacts.census.gov/qfd/states/00000.html
Gupta RS, Springston, MR, Warrier BS, Rajesh K, Pongracic J, Holl JL. The prevalence, severity, and
distribution of childhood food allergy in the United States. J Pediatr.2011; 128.doi: 10.1542/peds.2011-0204
Centers for Disease Control and Prevention. QuickStats: Percentage of children aged <18 years with food, skin,
or hay fever/respiratory allergies --- National health interview survey, United States, 1998—2009. 2011. Retrieved
from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6011a7.htm?s_cid+mm6011a7_w
U.S. Census Bureau. State and County QuickFacts.2010. Retrieved from http://quickfacts.census.gov/qfd/states/00000.html
Sampson HA. Update on food allergy. J Allergy Clin Immunol.2004; 113(5): 805-19.
Steinman HA, Hidden allergens in foods. J Allergy Clin Immunol. 1996;98(2): 241-250.
www.schoolnutrtion.org/foodallergies. Podcasts: Legal and regulatory requirements for managing food allergies in schools. Guidance for managing food allergies in schools. Teamwork is key to successful food allergy management in schools. Food safety considerations and food allergy management best practices for school food service. 2010.
USDA. Accommodating children with special dietary needs in the school nutrition programs. Fall 2001
















![Food & Formula Reference Guide [FFRG] · 8. Severe food allergies requiring an elemental formula 9. Life threatening disorders, disease and medical conditions that impair ingestion,](https://img.pdfslide.us/doc/110x75/5f68600c00640326c54dd526/food-formula-reference-guide-ffrg-8-severe-food-allergies-requiring-an.jpg)