Embed Size (px)
Citation preview

Left Main Revascularization

Dr. Md.Toufiqur Rahman MBBS, FCPS, MD, FACC, FESC, FRCP, FSCAI,
FCCP,FAPSC, FAPSIC, FAHA
Associate Professor of CardiologyNational Institute of Cardiovascular Diseases
Sher-e-Bangla Nagar, Dhaka-1207
Consultant, Medinova, Malbagh branchHonorary Consultant, Apollo Hospitals, Dhaka and
Life Care Centre, Dhanmondi
Left Main Revascularization

Coronary RevascularizationPCI vs CABG
CABG PCI• POBA• Atherectomy• Extraction Devices• Distal Protection Devices• Intracoronary Stenting
– BMS and DES
• Arterial conduits• Off-pump• Minimally invasive• Vein harvest• Robotics• Hybrid Procedures

ESC guidelines 2010 – CABG vs. PCI • Left main (isolated or 1VD ,ostium/shaft)
- CABG = IA, PCI = IIa B • Left main (isolated or 1VD, distal bifurcation)
- CABG = IA, PCI = IIb B • Left main + 2VD or 3VD,SYNTAX score < 32
- CABG = IA, PCI = IIb B• Left main + 2VD or 3VD,SYNTAX score 33
- CABG = IA, PCI = III B* I/IIb/III = recommendation class, A/B = level of evidence

Guidelines summary• CABG gold standard but PCI good option in
ostial/shaft disease or when SYNTAX ≤ 22 and risk of surgical complications is relatively high
• PCI also acceptable in high surgical risk patients with distal LM disease or when SYNTAX ≤ 32
• PCI should not be performed in patients who can undergo CABG and have unfavourable anatomy (SYNTAX > 33)

PCI and CABG do not work by intention to treat
The most important issue is long term results
In PCI success is “WRONGLY” defined as successful stent placement
Optimal: IVUS confirmed stent placement, should be the gold standard

1. Occlusion of the LAD or of the RCA which cannot be opened by PCI and with viable myocardium. Chronic occlusion of the RCA and sometimes even of the LAD can left untreated in elderly people with reduced physical activity.
2. Complex and calcific distal left main bifurcation and the PCI operator does not feel confident to treat or she/he does not expect to obtain a good final result
3. Long diffuse disease in the proximal LAD (needs a stent longer than 30-35 mm) in a patient with diabetes mellitus
4. A patient who has or may have problems with dual antiplatelet therapy
Conditions were CABG may be a better choice compared to PCI in patients with Left Main Stenosis

Revascularization Spectrum of CareHigh
Restonotic Risk
High Thrombotic / Safety Risk
Multi-Vessel Disease, etc.
DAPT concerns, etc.
Bare Metal StentsCABG
ESC 2009 • Two- year Outcomes of the SYNTAX Trial • Kappetein • Slide 12
Repeat Revascularization to 2 YearsRepeat Revascularization to 2 Years
8.6%
17.4%
0 12 24Months Since Allocation
Cum
ulat
ive E
vent
Rat
e (%
)
ITT population
P<0.001
TAXUS (N=903)CABG (N=897)
Cumulative KM Event Rate ±1.5 SE; log- rank P value;*Binary rates
20
40Before 1 year*5.9% vs 13.5%
P<0.001
After 1 year*3.7%vs 5.6%
P=0.06

ARTS II: TLR and ST at 5 years
Patrick W. Serruys, JACC Vol. 55, No. 11, 2010
14.5% TLR and 8% ST rate in multi-vessel disease

BMS Binary Restenosis Rates in DES Randomized Trials
Modified from Granada JF. Stent metal alloys. New DES Platforms Does the metal alloy matter? BARBARA HUIBREGTSE, DVM, AND JUAN F. GRANADA, MDPresented at: 2010 Transcatheter Therapeutics annual meeting; September 21–25, 2010;Washington,DC.

Other Options: Hybrid OR
– CABG-LIMA– Robotic- LIMA– Role of the Hybrid
OR• Define Hybid OR• Define Needs• Define Users• Define Patients

drto
ufiq1
9711
@ya
hoo.
com
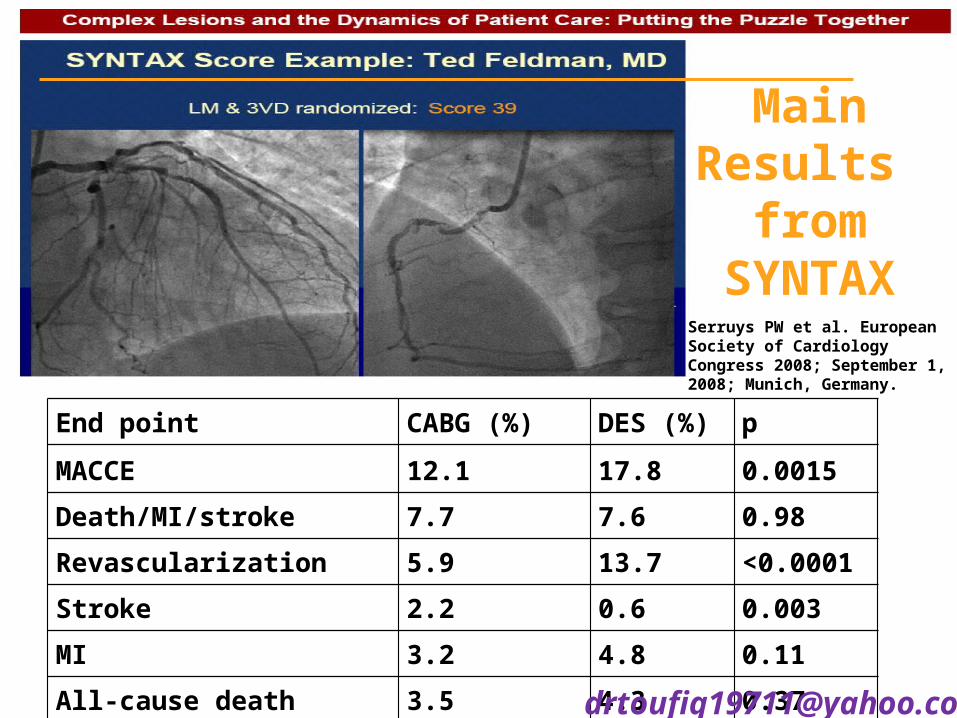
End point CABG (%) DES (%) p
MACCE 12.1 17.8 0.0015Death/MI/stroke 7.7 7.6 0.98Revascularization 5.9 13.7 <0.0001Stroke 2.2 0.6 0.003MI 3.2 4.8 0.11All-cause death 3.5 4.3 0.37
Serruys PW et al. European Society of Cardiology Congress 2008; September 1, 2008; Munich, Germany.
Main Results
from SYNTAX

Functional SYNTAX Score for Risk Assessment in Multivessel Coronary Artery Disease
Chang-Wook Nam MD, PhD⁎, †, Fabio Mangiacapra MD‡, Robert Entjes MD§, In-Sung Chung MD, PhD†, Jan-Willem Sels MD§, Pim A.L. Tonino MD, PhD§, Bernard De
Bruyne MD, PhD‡, Nico H.J. Pijls MD, PhD§, William F. Fearon MD⁎, , and FAME Study Investigators
• Applying the knowledge from FAME with SYNTAX– Anatomy and Physiology
• 497 FAME pts had SYNTAX Score prospectively collected • Only the “physiologic” significant lesions were scored• 32% of pts moved to a lower risk group• Only FSS and procedure time were independent variables of
1-yr MACE
J Am Coll Cardiol. 2011 Sep 13;58(12):1211-8
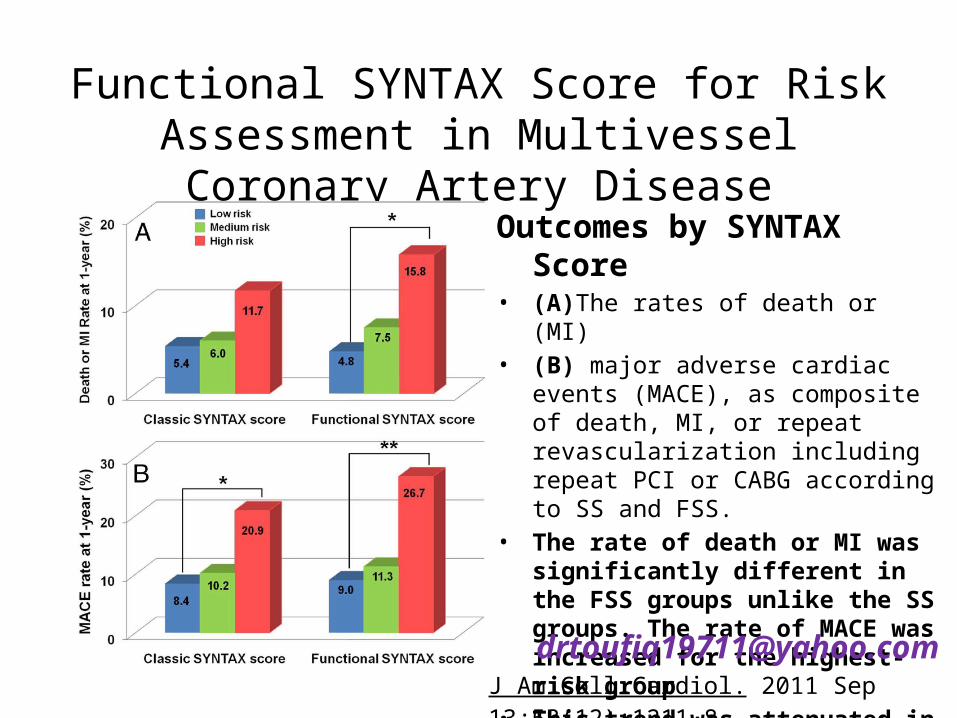
Functional SYNTAX Score for Risk Assessment in Multivessel Coronary Artery Disease
Outcomes by SYNTAX Score• (A)The rates of death or (MI) • (B) major adverse cardiac events (MACE),
as composite of death, MI, or repeat revascularization including repeat PCI or CABG according to SS and FSS.
• The rate of death or MI was significantly different in the FSS groups unlike the SS groups. The rate of MACE was increased for the highest-risk group
• This trend was attenuated in the FSS groups compared with the classic SS groups. *p < 0.01, **p < 0.001.
J Am Coll Cardiol. 2011 Sep 13;58(12):[email protected]

Left Main PCI
• PCI vs CABG Meta-analysis• 1,611 pts from 4 randomized clinical trials; 12 mo MACCE
– LEMANS (2008-52 PCI/35 DES/ 53 CABG)– SYNTAX ( Taxus DES, 357 PCI/348 CABG)– Boudroit, et al. (100 PCI/ 110 CABG-did not report CVA)– PRECOMBAT (Sirolimus DES, 300 PCI/300 CABG)– EXCEL (2,600 pts, Xience DES, 3 yr f/u, SYNTAX <32… ???)
• PCI non-significant 1yr MACCE, death and MI– Lower stroke– Higher rate of revascularization
Capodanno D, et al. JACC2011;58:1426-321-8 [email protected]

One-year outcomes in Left Main Patients Treated with PCI or CABG
End point PCI, n=809 (%) CABG, n=802 (%) p MACCE 14.5 11.8 0.11Death, MI,CVA 5.3 6.8
0.26Death 3.0 4.1
0.29MI 2.8 2.9
0.95CVA 0.1 1.7
0.013TVR 11.4 5.4 <0.001
Capodanno D, et al. JACC2011;58:1426-321-8

LMain• Long-term outcomes of PCI with DES versus CABG
UPLM • Meta-analysis of 24 studies published January
2000 to December 2012, 14,203 patients. No significant difference for all-cause mortality between PCI or CABG at 1 year (odds ratio [OR], 0.792; 95% confidence interval [CI], 0.53 to 1.19), 2 years (OR, 0.92; 95% CI, 0.67 to 1.26), 3 years (OR, 0.94; 95% CI, 0.6 to 1.48), 4 years (OR, 0.84; 95% CI, 0.53 to 1.33), and 5 years (OR, 0.79; 95% CI, 0.57 to 1.08).
Athappan G, Patvardhan E, Tuzcu ME, Ellis S, Whitlow P, Kapadia SR. Left Main CAD Stenosis. A meta-analysis of DES vs. CABG. JACC INT Dec 2013 6: 1219-30.
LMain• TVR was significantly higher for PCI and stroke
was significantly lower. Nonfatal MI showed a statistically significant lower trend in CABG patients at 1 year (OR, 1.62; 95% CI, 1.05 to 2.50), 2 years (OR, 1.6; 95% CI, 1.09 to 2.35), and 3 years (OR, 2.06; 95% CI, 1.36 to 3.1). There was no significant difference in combined major adverse cardiovascular and cerebrovascular events between the two groups.
• Conclusions: PCI with DES is a safe and durable alternative to CABG for UPLM stenosis in select patients at long-term follow-up.
Athappan G, Patvardhan E, Tuzcu ME, Ellis S, Whitlow P, Kapadia SR. Left Main CAD Stenosis. A meta-analysis of DES vs. CABG. JACC INT Dec 2013 6: 1219-30.

Consideration for Left Main PCI
• NERS Score/NERS Score II– More complicated but potentially more predictive
with reduction of variable from 54 to 16 (Chen, JACCINTV. 2013; 6:1233-41.
• Guidelines recommendation• Anatomic Location may be Key• Heart Team Approach• EXCEL Trial (2,600 pts, 3 yrs follow-up, DES vs
CABG for [email protected]

Figure 1. IVUS classification for LMCA bifurcation plaque distribution.
Oviedo C et al. Circ Cardiovasc Interv. 2010;3:105-112
Copyright © American Heart Association, Inc. All rights reserved.