Embed Size (px)
Citation preview
604
Diabetes Mellitus Lecture 22 Overview Diabetes mellitus is a disorder of carbohydrate, fat, and protein metabolism brought
about by impaired beta cell synthesis or release of insulin, or the inability of tissues to use glucose, connected by raised plasma glucose concentration and disturbance of glucose metabolism.
The term diabetes is derived from a Greek word meaning “going through” (Polyuria) and mellitus from the Latin word for “honey” or “sweet.” (Glucosuria)
Glucose is the end product involving the breakdown of carbohydrates Diabetes mellitus is a disorder quite distinct from the similarly-named diabetes
insipidus (DI). They both result in the production of large amounts of urine (diabetes), but in DM the urine is sweet while in DI (caused by ADH deficiency) it is not. (ADH is released from posterior Pituitary)
Before the days of laboratory tests, a simple taste test ("mellitus" or "insipidus") enabled the doctor to make the correct diagnosis.
Basic concept of glucose metabolism Glucose is the primary source of energy for the human body. Glucose is absorbed from the intestine and it is metabolized in nearly all body cells. Glucose enters the cell by facilitated diffusion (glucose transport proteins). This facilitated transport is stimulated very rapidly and effectively by an insulin signal
(glucose transport into muscle and adipose cells is increased up to twenty fold).
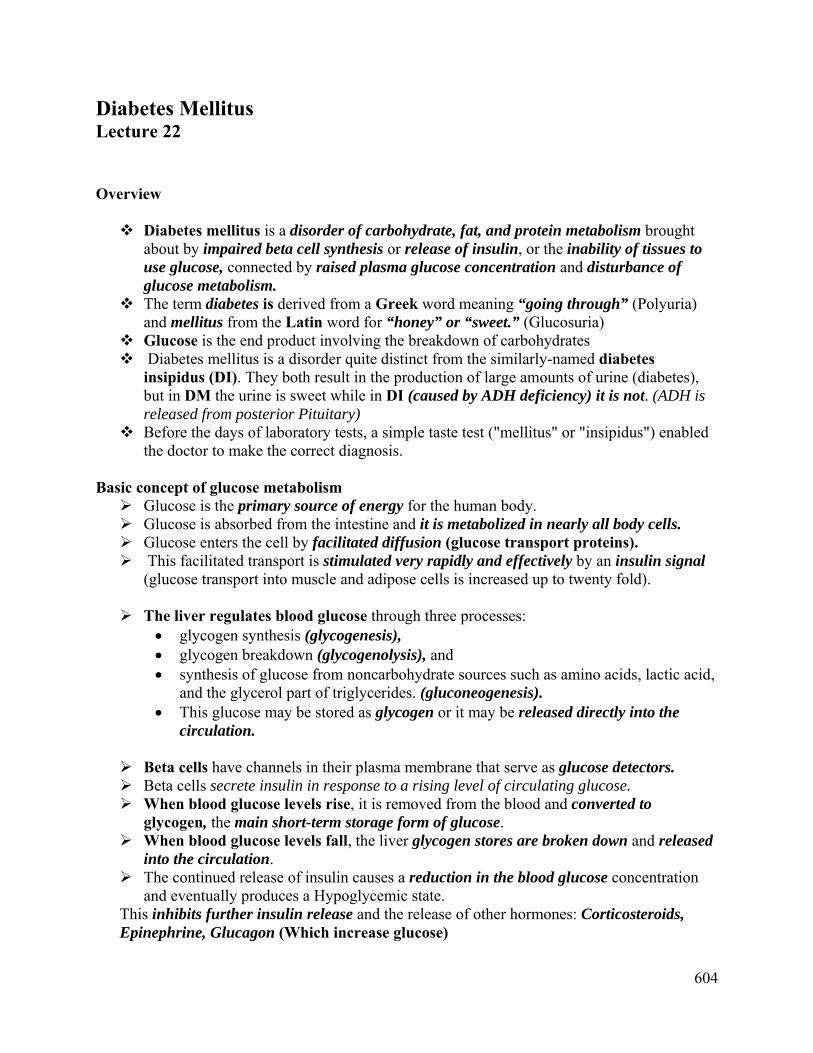
The liver regulates blood glucose through three processes: glycogen synthesis (glycogenesis), glycogen breakdown (glycogenolysis), and synthesis of glucose from noncarbohydrate sources such as amino acids, lactic acid,
and the glycerol part of triglycerides. (gluconeogenesis). This glucose may be stored as glycogen or it may be released directly into the
circulation.
Beta cells have channels in their plasma membrane that serve as glucose detectors. Beta cells secrete insulin in response to a rising level of circulating glucose. When blood glucose levels rise, it is removed from the blood and converted to
glycogen, the main short-term storage form of glucose. When blood glucose levels fall, the liver glycogen stores are broken down and released
into the circulation. The continued release of insulin causes a reduction in the blood glucose concentration
and eventually produces a Hypoglycemic state. This inhibits further insulin release and the release of other hormones: Corticosteroids, Epinephrine, Glucagon (Which increase glucose)
605
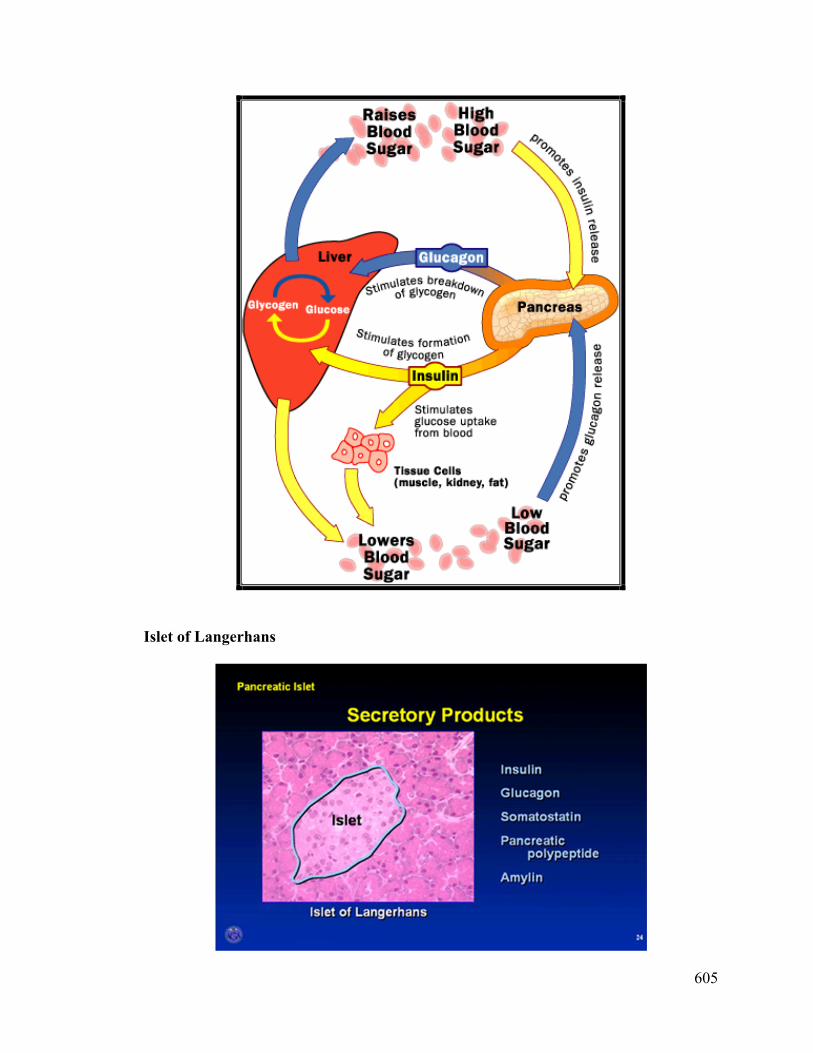
Islet of Langerhans

606
The Islets of Langerhans are commonly referred to as "islets" (pronounced "EYE-lets"). Islets actually are clusters of cells, with each "islet" containing 3,000 to 4,000 cells.
There are 1 million islets in a healthy, adult pancreas. They make up only 1 to 2 percent of the entire organ.
607
Endocrine pancreas
The actions of insulin are: 1) Stimulates skeletal muscle fibers & liver cells to take up glucose and convert it into
glycogen.
2) Increases glucose transport into tissues
3) Inhibiting "gluconeogenesis"; that is, the conversion of fats and proteins into glucose.
4) Increases triglyceride synthesis in adipose tissue and liver 5) Acts on fat (adipose) cells to stimulate the uptake of glucose.
6) Increase amino acids uptake from the blood and convert them into protein.( increases protein synthesis)
Glucagon function 1) Increases glycogen breakdown in liver 2) Increases lipolysis in adipose tissue 3) Increases gluconeogenesis in liver 4) Increases proteolysis in skeletal muscle; liberated amino acids may in turn be
converted to glucose
Somatostatin function 1) Inhibits the release of glucagon 2) Inhibits the release of growth hormone from the anterior pituitary
Amylin Function
1) Slowing gastric emptying, thereby delaying the delivery of nutrients to the circulation.
2) A second effect is to decrease food intake. 3) Amylin potently inhibits postprandial glucagon secretion; this means reducing the
abnormal hyperglucagonemia in the postprandial period, thereby reducing the delivery of glucose from the liver into the circulation in the postprandial state.
So, the net effect of all this is to reduce the rate of glucose appearance in the circulation to minimize the rise in postprandial glucose.
Pancreatic Polypeptide (PP)
1) Secreted from gamma cells(F Cells) 2) It is secreted in response to hypoglycemia, ingestion of food, or "sham" feeding (food
is chewed, but not swallowed), secondary to vagal nerve stimulation. 3) It can inhibit gallbladder contraction and pancreatic exocrine secretion
608
Classification of Diabetes Mellitus
Type 1 - insulin-dependent diabetes mellitus (IDDM) Sometimes called juvenile (or juvenile-onset), ketotic (or ketosis-prone), or brittle
diabetes Affects children or young adults
Type 2 - noninsulin-dependent diabetes mellitus (NIDDM) Also called maturity-onset, non-ketotic, or stable diabetes May be asymptomatic for many years Affects people over 40
MODY- Mature Onset Diabetes of the Youth early form of DM type 2 (2-6% of all DM type 2 patients) onset between late adolescence and age 40
Type 3 - gestational diabetes mellitus (GDM) Occurs during pregnancy then disappears after childbirth May be a marker of susceptibility to type 2 later in life
Type 4 - other types of diabetes linked to diseases of the pancreas, hormonal changes, side effects of drugs, or genetic defects
Clinical manifestation of DM “The Polys” Diabetes Mellitus is characterized by the polytriad: Polyuria / polydipsia: Glucose spilled into urine, leads to osmotic diuresis (polyuria).
This leads to dehydration, and increased thirst (polydipsia). Polyphagia: without insulin function, glucose cannot be transported into cells. Cells are
“hungry” and hunger sensation is triggered. “Polys” can go unnoticed for years.
609
Type 1 diabetes mellitus Pathophysiology
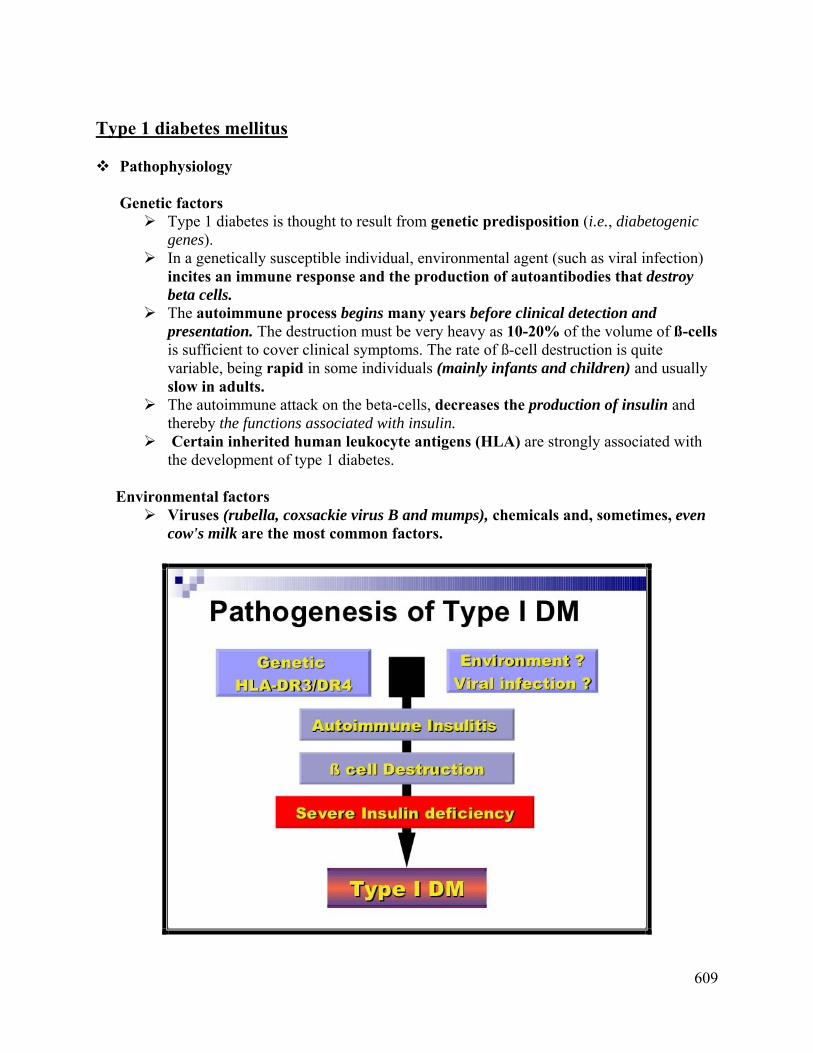
Genetic factors Type 1 diabetes is thought to result from genetic predisposition (i.e., diabetogenic
genes). In a genetically susceptible individual, environmental agent (such as viral infection)
incites an immune response and the production of autoantibodies that destroy beta cells.
The autoimmune process begins many years before clinical detection and presentation. The destruction must be very heavy as 10-20% of the volume of ß-cells is sufficient to cover clinical symptoms. The rate of ß-cell destruction is quite variable, being rapid in some individuals (mainly infants and children) and usually slow in adults.
The autoimmune attack on the beta-cells, decreases the production of insulin and thereby the functions associated with insulin.
Certain inherited human leukocyte antigens (HLA) are strongly associated with the development of type 1 diabetes.
Environmental factors
Viruses (rubella, coxsackie virus B and mumps), chemicals and, sometimes, even cow's milk are the most common factors.

610
HLA-DR HLA-DR is an MHC class II cell surface receptor encoded by the human leukocyte
antigen complex on chromosome 6. The primary function of HLA-DR is to present peptide antigens, potentially foreign in
origin, to the immune system. The peptide (such as the staphylococcal enterotoxin I peptide) is bound into a DR
molecule and presented to a few of a great many T-cell receptors found on T-helper cells. Antigen presenting cells (macrophages, B-cells and dendritic cells) are the cells in which
DR are typically found.
DR receptor presenting antigen to TCR on T-helper cell
Diseases associated with specific HLA antigens
1) HLA-DR3/DR2 Systemic Lupus Erythematosus 2) HLA-DR4 Rheumatoid Arthritis 3) HLA-B7 and DR2 Multiple Sclerosis 4) HLA-B8, DR3/DR4 Type 1 diabetes 5) HLA-B27 Ankylosing Spondylitis
611
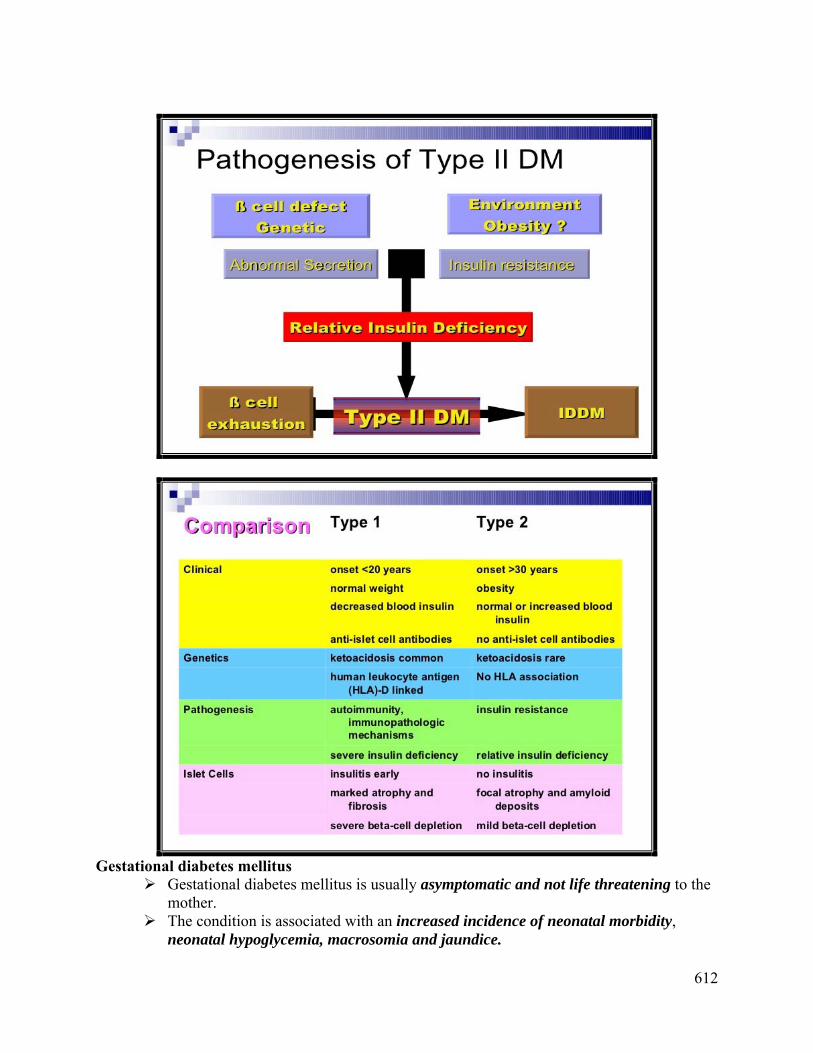
Type 2 diabetes mellitus Type 2 diabetes mellitus was formerly known as non-insulin-dependent diabetes mellitus
(NIDDM), type II, or adult-onset diabetes. It is much more common that type1diabetes and comprises approximately 90% of all
individuals with diabetes. The patients are usually older at the onset of disease, mostly present only minimal
symptoms. Insulin concentrations are mostly increased but they can be normal or decreased.
Obesity is quite common and weight reduction ameliorates the hyperglycemia. The disease usually develops after 40 years of age. Oral hypoglycaemic drugs and dietary manipulation represent the biggest role in
therapy; insulin is sometimes required to correct hyperglycemia. Pathophysiology(Type 2 diabetes mellitus) The groups of disorders, of which two are most common, represent the new
knowledge type 2 diabetes mellitus. The first one is a decreased ability of insulin to act on peripheral tissues. Usually we
call it "insulin resistance". Insulin resistance is defined as a decreased biological response to normal
concentrations of circulating insulin and represents the primary underlying pathological process.
The second is the dysfunction of pancreatic ß-cells, represented by the inability to produce sufficient amount of insulin to overcome insulin resistance in the peripheral tissues.
Later on the insulin production can be insufficient to compensate the insulin resistance due to ß-cells dysfunction.
The common result is the relative deficiency of insulin. The End result is that DM type 2 is characterized by insulin resistance and relative,
not complete insulin deficiency. Data support the concept that insulin resistance is the primary defect, preceding the
derangement of insulin secretion. Insulin resistance usually precedes the clinical signs by as much as 20 years. The basis of insulin resistance and insulin secretion defect results from a
combination of environmental and genetic factors.
Genetic factors There are several genes associated with type 2 diabetes affecting insulin secretion
and action as well as regulate body weight. Environmental factors Body weight and exercise are the most important. The links between obesity and type 2 diabetes are complex: although 60-80% of
those with type 2 diabetes are obese, diabetes develops in fewer than 15% of obese individuals.
The clinical signs and therapy requirement usually go down with weight reduction and body exercise.
612
Gestational diabetes mellitus
Gestational diabetes mellitus is usually asymptomatic and not life threatening to the mother.
The condition is associated with an increased incidence of neonatal morbidity, neonatal hypoglycemia, macrosomia and jaundice.

613
In addition, mothers with GDM have increased rates of cesarean delivery and chronic hypertension.
Even normal pregnancies are associated with increasing insulin resistance, mostly in the second and third trimesters.
Euglycemia is maintained by increasing insulin secretion. In those women who are not able to increase the secretion of insulin, gestational diabetes develops.
The pathophysiology of gestational diabetes mellitus is not well known and includes family history of diabetes mellitus, obesity, complications in previous pregnancy(ies) and advanced maternal age.
It is essential to detect pre-existing diabetes mellitus which has a much worse prognosis for the fetus.
. To screen for GDM, a 50-g glucose screening test should be done at 24-28 weeks of gestation. This is followed by a 100-g, 3-hour oral glucose tolerance test if the patient's plasma glucose concentration at 1 hour after screening is greater than >140 mg/dL.
Screening & Diagnosis of DM: Fasting Plasma Glucose (mg/dL) (FPG)
– Check a fasting glucose level Oral Glucose Tolerance Test (mg/dL) (OGTT)
– Check blood glucose 2 hours after a 75g oral glucose load Hemoglobin A1c
– Shows percentage of glycated hemoglobin. – Reflects glucose control over 6-12 week period. –
Glycated Hemoglobin
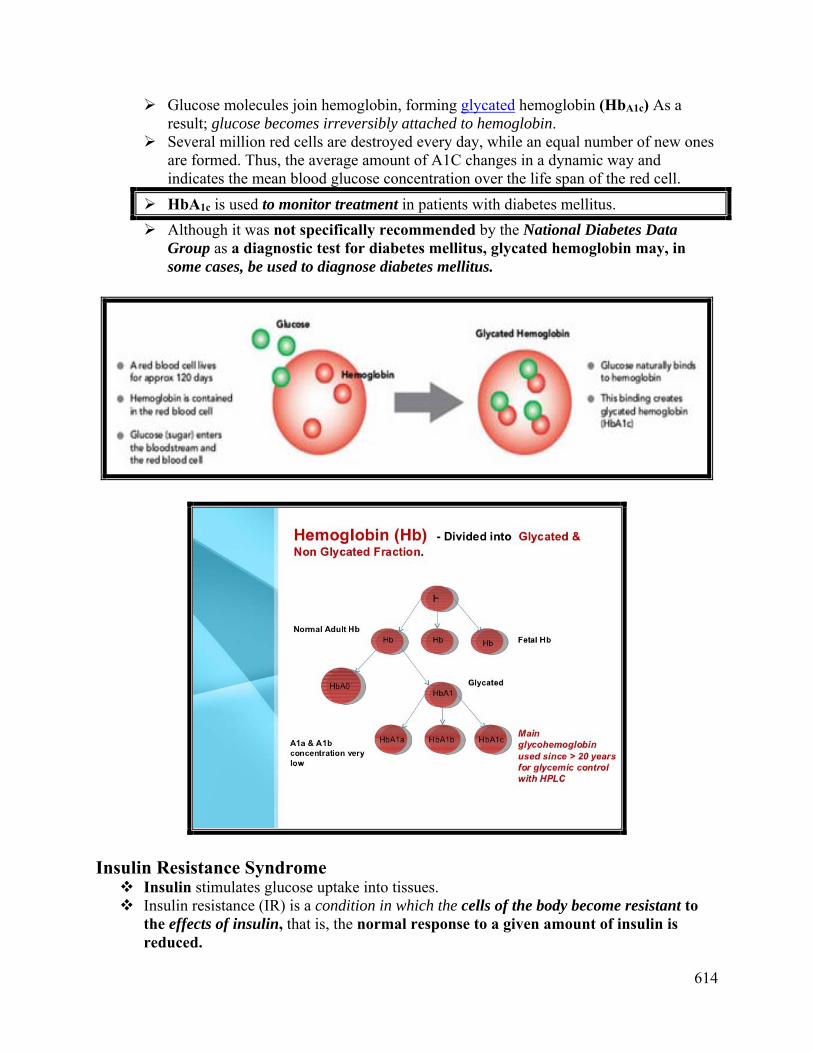
The normal life span of the RBC is 120-days.Hemoglobin formed in new red blood cells enters the circulation without any glucose attached.
RBCs are freely permeable to glucose.
614
Glucose molecules join hemoglobin, forming glycated hemoglobin (HbA1c) As a result; glucose becomes irreversibly attached to hemoglobin.
Several million red cells are destroyed every day, while an equal number of new ones are formed. Thus, the average amount of A1C changes in a dynamic way and indicates the mean blood glucose concentration over the life span of the red cell.
HbA1c is used to monitor treatment in patients with diabetes mellitus.
Although it was not specifically recommended by the National Diabetes Data Group as a diagnostic test for diabetes mellitus, glycated hemoglobin may, in some cases, be used to diagnose diabetes mellitus.
Insulin Resistance Syndrome Insulin stimulates glucose uptake into tissues. Insulin resistance (IR) is a condition in which the cells of the body become resistant to
the effects of insulin, that is, the normal response to a given amount of insulin is reduced.
615
To compensate for resistance, the pancreas secretes more insulin. As a result, higher levels of insulin are needed in order for insulin to have its effects. The resistance is seen with both the body’s own insulin (endogenous) and if insulin is
given through injection (exogenous). Insulin resistance syndrome is characterized by hyperinsulinemia and an increased
prevalence of obesity, hypertension, dyslipemia , Syndrome X (metabolic or dysmetabolic syndrome) and type 2 diabetes mellitus.
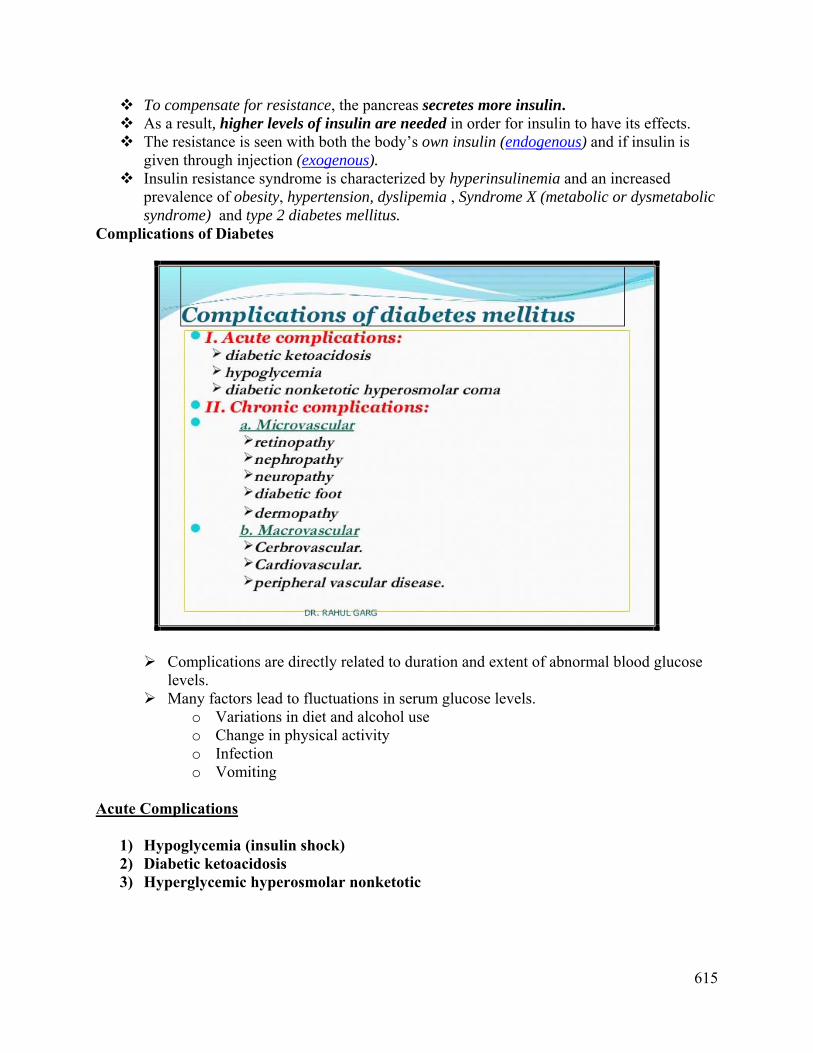
Complications of Diabetes
Complications are directly related to duration and extent of abnormal blood glucose levels.
Many factors lead to fluctuations in serum glucose levels. o Variations in diet and alcohol use o Change in physical activity o Infection o Vomiting
Acute Complications
1) Hypoglycemia (insulin shock) 2) Diabetic ketoacidosis 3) Hyperglycemic hyperosmolar nonketotic

616
1) Hypoglycemia (insulin shock) More common with insulin replacement treatment Can occur because of excess oral hypoglycemic drugs Excess insulin in circulation
o Glucose deficit in blood o Can be life-threatening or cause brain damage if untreated o Often follows strenuous exercise o Dosage error o Vomiting o Skipping meal after taking insulin
Pathophysiology of Hypoglycemic Shock
617
Hypoglycemic Shock: Signs and Symptoms Disorientation and change in behavior May appear impaired Anxiety or decreased responsiveness Decreased blood glucose level Decreased BP, increased heart rate Decreasing level of consciousness
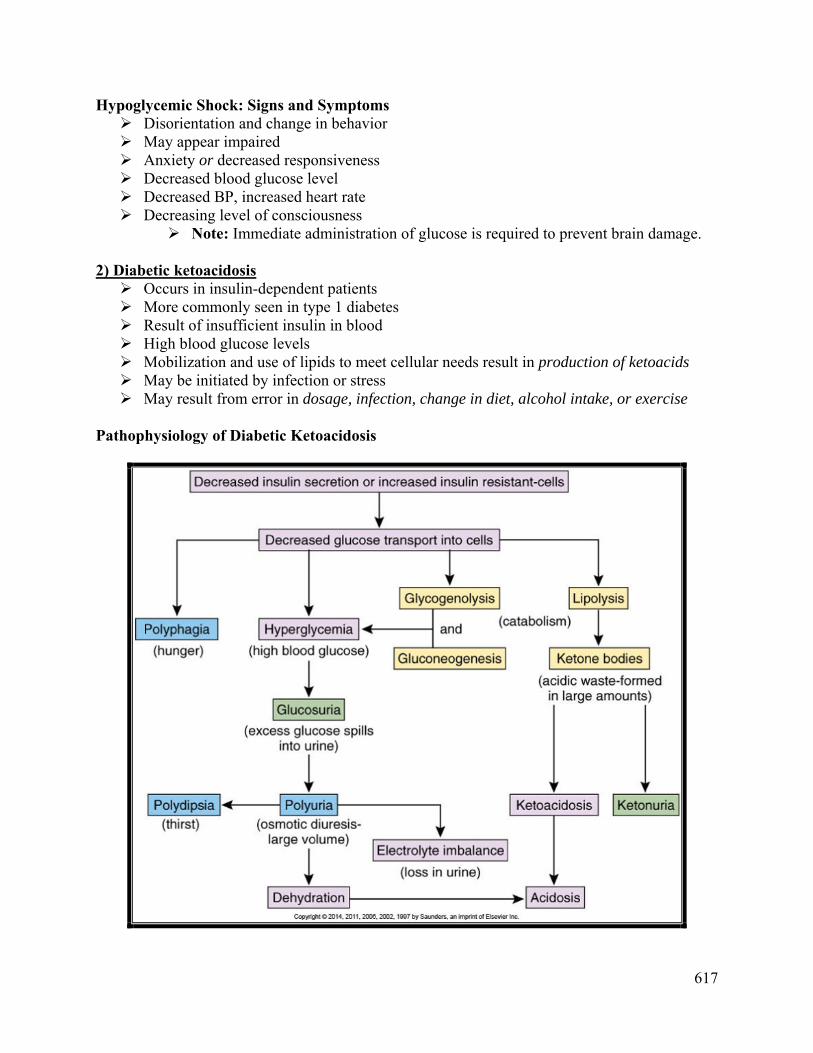
Note: Immediate administration of glucose is required to prevent brain damage. 2) Diabetic ketoacidosis Occurs in insulin-dependent patients More commonly seen in type 1 diabetes Result of insufficient insulin in blood High blood glucose levels Mobilization and use of lipids to meet cellular needs result in production of ketoacids May be initiated by infection or stress May result from error in dosage, infection, change in diet, alcohol intake, or exercise
Pathophysiology of Diabetic Ketoacidosis

618
Diabetic Ketoacidosis: Signs and Symptoms Dehydration : Thirst, dry, rough oral mucosa, warm, dry skin Rapid, deep respiration—acetone breath ,Lethargy, decreased responsiveness Metabolic acidosis : May lead to loss of consciousness Electrolyte imbalances : Abdominal cramps, nausea, vomiting, lethargy, weakness
3) HHNK: Hyperglycemic hyperosmolar nonketotic coma Occurs in type 2 diabetes Insidious in onset and diagnosis may be missed Often occurs in older clients and assumed to be cognitive impairment Results in severe dehydration and electrolyte imbalances Manifestations
Hyperglycemia Severe dehydration
o Increased hematocrit o Loss of turgor o Increased heart rate and respirations
Electrolyte imbalances result in: o Neurologic deficits o Muscle weakness o Difficulties with speech o Abnormal reflexes
Chronic DM Complications

619

620
DM Treatment
Incretins & DDP4 A new class of oral antidiabetic agents known as :
dipeptidyl peptidase-4 (DPP-4) inhibitors (commonly called gliptins) work by :
blocking the action of DPP-4 (an enzyme which destroys the hormone incretin)
& also they improve the β-cell function.
Incretins are a group of gastrointestinal hormones that cause: An increase in the amount of insulin released from the beta cells of the islets of
Langerhans after eating, even before blood glucose levels become elevated. They also slow the rate of absorption of nutrients into the blood stream by
reducing gastric emptying and may directly reduce food intake. As expected, they also inhibit glucagon release from the alpha cells of the Islets
of Langerhans. Treatment with Insulin Type 1 diabetes is controlled by carefully-regulated injections of insulin. (Insulin cannot
be taken by mouth because, being a protein, it would be digested).

621
However, the U.S. FDA has approved [in January 2006] an insulin inhaler that delivers insulin through the lungs and may reduce the number of daily injected doses needed.)
For many years, insulin extracted from the glands of cows and pigs was used. However, pig insulin differs from human insulin by one amino acid; beef insulin by three. Although both work in humans to lower blood sugar, they are seen by the immune system
as "foreign" and induce an antibody response in the patient that blunts their effect and requires higher doses.
Two approaches have been taken to solve this problem: Convert pig insulin into human insulin by removing the one amino acid that
distinguishes them and replacing it with the human version. This approach is expensive. The favored approach is to: Insert the human gene for insulin into E. coli and grow recombinant human insulin in
culture tanks. Insulin is not a glycoprotein so E. coli is able to manufacture a fully-functional molecule
(trade name = Humulin). Yeast is also used (trade name = Novolin).
Recombinant DNA technology has also made it possible to manufacture slightly-modified forms of human insulin that work faster (Humalog® and NovoLog®) or slower (Lantus®) than regular human insulin.
Metabolic Syndrome A combination of metabolic abnormalities which increase the risk of heart disease,
diabetes and other diseases Obesity is a component of met. synd. Signals from adipocytes in obesity cause metabolic abnormalities such as:
o Dyslipidemia o Glucose intolerance o Insulin resistance o Hypertension
Features of metabolic syndrome Obesity High serum triglycerides (TGs) Low HDL cholesterol Hypertension Hyperglycemia Insulin resistance (hyperinsulinemia)

622
Risk factors for metabolic syndrome Obesity Alcoholism Sedentary Lifestyle Smoking Hypercortisolism (Steroid use/Cushing’s disease) Drugs (Rifampicin, isoniazid, etc.) Mutations in insulin receptor
623
Metabolic syndrome is linked to: Heart disease (1.5-3 fold increase in atherosclerosis) Type-2 diabetes mellitus (5-fold increase) Kidney disease Reproductive abnormalities in women
o Polycystic ovarian syndrome o Impaired ovulation and fertility o Irregular menstruation
Nonalcoholic steatohepatitis (fatty liver disease) o Related to impaired lipid metabolism
Cancer o Obesity is a major risk factor for cancer of esophagus, colon and rectum, liver,
gall bladder o Being overweight and obese accounts for 14% of all cancer deaths in men and
20% of those in women NCEP* ATP** III Guideline (2002) Diagnosis: If any 3 or more of these risk factors are present Waist circumference:
o Men >102 cm (>40 in) o Women >88 cm (>35 in)
Triglycerides >150 mg/dL HDL cholesterol:
o Men <40 mg/dL o Women <50 mg/dL
Blood pressure 130/ 85 mm Hg Fasting glucose >100 mg/dL
*National Cholesterol Education Program **Adult Treatment Panel Markers of metabolic syndrome Lipoproteins (LDL, HDL) Adipokines (Leptin, adiponectin) Inflammatory markers
o c-reactive protein, TNF-a, IL-6, IL-8 Hemostatic marker
o Plasminogen activator inhibitor-1

624
Managing Metabolic Syndrome Primary intervention: Lifestyle changes
Weight reduction o Target BMI < 25 o Reduced intake of calories and fats o More physical activity
Smoking cessation Secondary intervention: Medication to treat existing risk factors
Management of o Blood pressure (anti-hypertensive drugs) o Lipids (statins, fibrates) o Blood glucose (metformin, Thiazolidinediones “TZDs”)
Aspirin for CVD prevention o Daily low dose aspirin (81-325mg) for:
o Men > 45 o Postmenopausal women
_________________