Embed Size (px)
Citation preview

INFLAMMATORY BOWEL DISEASESMS 2044

INFLAMMATORY BOWEL DISEASE
IBD is a group of inflammatory conditions of large intestine ,in
some cases small intestine.

Intestines - Pathology
Idiopathic Inflammatory Bowel Diseases
Etiology & Pathogenesis
Crohn’s disease
Ulcerative Colitis

Idiopathic Inflammatory Bowel Diseases
• Etiology & Pathogenesis• Characterized by= A chronic, relapsing
inflammatory conditions • unknown etiology.• speculations involve= Genetic factors, unknown
infectious agents, special susceptibility factors, altered immuno-reactivity to dietary
• or infectious antigens & altered regulatory controls of the inflammatory responses

Idiopathic Inflammatory Bowel Diseases
• Distinguished into two clinicopathologic entities: – Crohn’s disease (CD) – Ulcerative colitis (UC)
Crohn’s disease (CD)• Transmural granulomatous inflammation of the bowel,
with mucosal ulcerations, fissures & fistulas in Young (20s)whites Females
• Skip lesions (cobble stone app.)Ulcerative colitis (UC)• crypt abscesses, psudopolyps & ↑risk of carcinoma
(adenocarcinoma)

Different Clinical, Endoscopic, and Radiographic Features of Crohn’s & Ulcerative Colitis
Ulcerative Colitis Crohn's Disease
CLINICAL
Gross blood in stool Yes Occasionally
Mucus Yes Occasionally
Systemic symptoms Occasionally Frequently
Pain Occasionally Frequently
Abdominal mass Rarely Yes
Significant perineal disease No Frequently
Fistulas No Yes
Small intestinal obstruction No Frequently
Colonic obstruction Rarely Frequently
Response to antibiotics No Yes
Recurrence after surgery No Yes
ANCA-positive Frequently Rarely

Ulcerative Colitis Crohn's Disease
ENDOSCOPIC
Rectal sparing Rarely Frequently
Continuous disease Yes Occasionally
"Cobblestoning" No Yes
Granuloma on biopsy No Occasionally
RADIOGRAPHIC
Small bowel significantly abnormal No Yes
Abnormal terminal ileum Occasionally Yes
Segmental colitis No Yes
Asymmetrical colitis No Yes
Stricture Occasionally Frequently

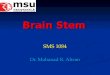
Intestines - Pathology Idiopathic Inflammatory Bowel Diseases
(CD) (UC)
Fissuring Ulcer
noncaseating granulomas

Pathogenesis The common end pathway is inflammation of the mucosal
lining of the intestinal tract, causing ulceration, edema, bleeding, and fluid and electrolyte loss.
Persons with IBD have a genetic predisposition (or perhaps susceptibility) for the disease.
The triggering event for the activation of the immune response has yet to be identified.
Possible factors related to this event include a pathogenic organism (as yet unidentified), an immune response to an intraluminal antigen (eg, protein from cow milk), or an autoimmune process whereby an appropriate immune response to an intraluminal antigen and an inappropriate response to a similar antigen is present on intestinal epithelial cells (ie, alteration in barrier function).

ULCERATIVE COLITISUlcerative colitis (Colitis ulcerosa, UC) is a form of
inflammatory bowel disease (IBD). Ulcerative colitis is a form of colitis, a disease of the
intestine, specifically the large intestine or colon, that includes characteristic ulcers, or open sores, in the colon.
The main symptom of active disease is usually diarrhea mixed with blood, of gradual onset.
however, a systemic disease that affects many parts of the body outside the intestine


AETILOGY• Exact cause is unknown.• Several causes have been suggested .it
includes
1. Genetic Factors
2. Environmental Factors
3. Auto Immune Disease
4. Several Other Theories

Genetic factors • A genetic component to the etiology of
ulcerative colitis can be hypothesized based on the following
1. Aggregation of ulcerative colitis in families. 2. Diet: as the colon is exposed to many different
dietary substances which may encourage inflammation, dietary factors have been hypothesized to play a role in the pathogenesis
3. Breastfeeding: There have been conflicting reports of the protection of breastfeeding in the development of inflammatory bowel disease.
3. Other childhood exposures, or infections

Autoimmune disease Some sources list ulcerative colitis as an
autoimmune disease Disease in which immune system malfunctions,
attacking some parts of body. But it is seen that surgical removal of large
intestine cures disease, including manifestations outside digestive system.
This suggests cause of disease is in colon itself, not in immune system.

Ulcerative colitis involves only the mucosa; it is characterized by the formation of crypt abscesses and a coexisting depletion of goblet cell mucin.
In severe cases, the submucosa may be involved; in some cases, the deeper muscular layers of the colonic wall is also affected.
Increased intensity of the cellular infiltrate in the lamina propria with alterations of the composition.
Infiltrate is more extensive and extends diffusely towards the deeper part (transmucosal)
Accumulation of plasma cells near the mucosal base, in-between the crypt base and the muscularis mucosae (basal plasmacytosis
Pathological Feature

An irregular surface or a villiform surface and a disturbed crypt architecture.
Mucosal atrophy characterized by a combination of crypt drop-out and shortening of crypts.
Mucosal ulcerations and erosions, mucin depletion, Paneth-cell metaplasia and diffuse thickening of the
muscularis mucosae


Patients with ulcerative colitis can occasionally have aphthous ulcers involving the tongue, lips, palate and pharynx
Endoscopic image of ulcerative colitis showing loss of vascular pattern of the sigmoid colon, granularity and some friability of the mucosa.

Clinical presentation
1. Diarrhoea mixed with blood and mucus.
2. Gradual onset.
3. Signs of weight loss.
4. Different degrees of abdominal pain ranging from mild discomfort to severely painful cramps.

CLASSIFICATIONExtent of involvement• The disease is classified by the extent of involvement,
depending on how far up the colon the disease extends.
1.Distal colitisa. Proctitis: Involvement limited to the rectum.
b. Proctosigmoiditis: Involvement of the rectosigmoid colon, the portion of the colon adjacent to the rectum.
c. Left-sided colitis: Involvement of the descending colon, which runs along the patient's left side, up to the splenic flexure and the beginning of the transverse colon.
2.Extensive colitis, inflammation extending beyond the reach of enemas:
– Pancolitis: Involvement of the entire colon


1. Mild disease : fewer than 4 stools daily,no signs of systemic toxicity,normal ESR,mild abdominal pain.
2. Moderate disease :more than 4 stools daily,minimal signs of toxicity,anaemia,moderate abdominal pain,low grade fever.
3. Severe disease :more than 6 bloody stools,evidence of toxicity with fever,tachycardia,elevated ESR
4. Fulminant disease :more than 10 stools,bleeding,toxicity,abdominal tenderness,blood transfusion requirement.unless treated will lead to death.
Severity of disease

Extraintestinal features
1. Iritis2. Episcleritis3. Aphthous ulcers involving
tongue,lips,palate,pharynx.4. Arthritis5. Ankylosing spondylitis6. Erythema nodusum7. Deep venous thrombosis8. Pulmonary embolism9. Auto immune hemolytic anaemia10. Clubbing of fingers

Diagnosis 1. Complete blood count-
anaemia,thrombocytosis,high platelet count.2. Electrolyte studies-hypokalemia,hypomagnesia3. Renal function tests4. Liver function tests5. X-ray6. Stool culture7. ESR8. C-reactive protein

H&E stain of a colonic biopsy showing a crypt abscess:a classic finding in
ulcerative colitis
[edit] General

Crohn's Disease

Contents
• Introduction and definition of Crohn’s Disease• Classification• Cause • Pathology• Complications• Clinical features• Diagnosis• Investigations• Disease at glance

Definition:Crohn's disease (also known as regional
enteritis) is a chronic, episodic, inflammatory condition of the gastrointestinal tract characterized by
transmural inflammation (affecting the entire wall of the involved bowel) and skip lesions (areas of inflammation with areas of normal lining between).
Crohn's disease is a type of inflammatory bowel disease (IBD) and can affect any part of the gastrointestinal tract from mouth to anus; as a result,
the symptoms of Crohn's disease vary between affected individuals.

Introduction to Crohn’s disease:
This is a chronic inflammatory disease which causes stomach pains, diarrhoea, and weight loss.
The disease is characterised by periods of activity and remissions.
It typically affects the lower part of the small intestine (ileum) or the large intestine (colon), but it can affect any part of the digestive system.

Crohn DiseaseCrohn Disease
any level of alimentary tracta) small intestine alone 40%b) sm. Intestine + colon 30%c) colon alone 30%
“skip” lesions pathological characteristics:
a) mucosal damage (transmural)b) well demarcated regionsc) noncaseating granulomasd) formation of fissures e) narrowed lumen (obstruction)
www.freelivedoctor.com

The affected areas become red and swollen and ulceration may occur.
As the ulcers heal, the formation of scar tissue makes the intestine increasingly narrow, leading to obstruction.
There is no cure for Crohn's disease, but the symptoms can be treated and the periods of remission can be made to last several years.

Classification:• Based on location.

Classification contd..

Classification
• Based on behaviour of disease
Stricturing disease.
Penetrating disease.
Inflammatory disease.

CauseThe exact cause of Crohn's disease is unknown.
However, genetic and environmental factors have been invoked in the pathogenesis of the disease.
Mutations in the CARD15 gene (also known as the NOD2 gene) are associated with Crohn's disease and with susceptibility to certain phenotypes of disease location and activity.
Recently, research has indicated that Crohn's
disease has a strong genetic link.

Cause contd..• Abnormalities in the immune system • Many environmental factors.• Diets • Smoking• Methods of hormonal contraception • Some bacteria:
Eg Mycobacterium avium subsp. Paratuberculosis, mannose, anti saccharomyces cerevisiae antibodies and E. coli

Pathology:
Odeomatous and thickened bowel wall
Cobblestone
Patchy inlammation
Skip lessions
Transmural inflammation
H and E section of colectomy showing transmural inflammation.

www.freelivedoctor.com

Clinical Features
• Ileal Crohn’s Disease Abdominal painDiarrhea Weight loss• Crohn’s colitisBloody diarroheaPassage of mucusLethargyMalaiseAnorexiaWeight loss

f) chronic course may lead to:i) fibrosing strictures
- terminal ileum- fistulas other areas
ii) protein lossiii) Vit B12 lossiv) bile salt loss
- steatorrhea v) linear serpentine ulcers
www.freelivedoctor.com

Complications:
• Intestinal:-Severe, life-threatening inflammation of colon.
Perforation of the small intestine or colon.
Life-threatening acute haemorrhage.
Fistulae and perianal disease.
Cancer.

Differential Diagnosis
• Indium- or technetium- labelled white scanning.

Investigations:
• Endoscopic image of Crohn's colitis showing deep ulceration.

Contd…..BacteriologyBarium studiesOther investigationsX-rayRadio labelled white cell scanUltrasoundMRI scans

Contd..• CT scan showing Crohn's disease in the
fundus of the stomach.

Crohn’s Disease at Glance:
Crohn's disease is a chronic inflammatory disease of the intestines.
The cause of Crohn's disease is unknown. Crohn's disease can cause ulcers in the small
intestine, colon, or both. Abdominal pain, diarrhea, vomiting, fever, and
weight loss are symptoms of Crohn's disease. Crohn's disease of the small intestine may
cause obstruction of the intestine.

Contd.. Crohn's disease can be associated with reddish,
tender skin nodules, and inflammation of the joints, spine, eyes, and liver.
The diagnosis of Crohn's disease is made by barium enema, barium x–ray of the small bowel, and colonoscopy.
The choice of treatment for Crohn's disease depends on the location and severity of the disease.
Treatment of Crohn's disease includes drugs for suppressing inflammation or the immune system, antibiotics, and surgery.

ULCERATIVE COLITIS
CROHN’S
Age Any Any
Sex m=f M=f
Anatomical distribution
Colon only Any part of G.I
Presentation Bloody diarrhoea
Variable; pain diarrhoea,
Weight loss
Risk factors more common in non smokers
More common in smokers
Comparison of UC and CD

Treatment of Inflammatory Bowel Disease

TREATMENT Treatment for IBD may include:
DIETARY CHANGESLIFESTYLE CHANGES
DRUG THERAPY SURGERY

Dietary Changes
• Taking specific nutritional supplements,
• Limiting dairy products, • Eating low-fat foods, • Avoiding foods high in
undigestible fiber • Following doctor-
recommended diets and
• Eating smaller, more frequent meals.

LIFESTYLE CHANGES
.
Taking rest
nonsmoking
Stress reductionDoing exercise

Drug Therapies
• 5-Aminosalicylates (5-ASA)
• Glucocorticoids (steroids)
• Antibiotics
• Immunosuppressants
• Biological Therapy

Aminosalicylates
Sulfasalazine (5-aminosalicylic acid and sulfapyridine as carrier substance)
Mesalazine (5-ASA), e.g. Asacol, Pentasa Balsalazide (prodrug of 5-ASA) Olsalazine (5-ASA dimer cleaves in colon)
Oral, rectal preparation