Embed Size (px)
Citation preview

ORIGINAL RESEARCH
The Relationship Between Anterior Glenohumeral Laxityand Proprioception in Collegiate Baseball Players
Kevin G. Laudner, PhD, ATC,*† Keith Meister, MD,† Satoshi Kajiyama, MS, ATC,*and Bria Noel, ATC*
Objective: To determine if a relationship exists between anteriorglenohumeral (GH) laxity and proprioception.
Design: Cross-sectional study.
Setting: University biomechanics laboratory.
Participants: Thirty asymptomatic collegiate baseball players.
Independent Variables: Anterior GH laxity.
Main Outcome Measures: Proprioception (active joint positionsense) at positions of 75 degrees of external rotation, 30 degrees ofexternal rotation, and 30 degrees of internal rotation were measuredusing an isokinetic dynomometer. Anterior GH laxity was measuredusing an instrumented arthrometer.
Results: Linear regression analyses showed that there were norelationships between anterior GH laxity and active joint positionsense at 30 degrees of GH internal rotation and 30 degrees of GHexternal rotation (r = 0.21, P = 0.13). However, there was a moderatepositive relationship between anterior GH laxity and joint positionsense at 75 degrees of shoulder external rotation (r = 0.56, P = 0.001).
Conclusions: These results suggest that shoulder proprioception in 75degrees of external rotation decreases as anterior GH laxity increases.These results may prove beneficial in the prevention, evaluation, andtreatment of various shoulder injuries associated with GH laxity.
Key Words: shoulder, throwing athlete, instability, sensorimotor
(Clin J Sport Med 2012;22:478–482)
INTRODUCTIONDuring the late cocking phase of the throwing motion,
the glenohumeral (GH) joint has been shown to produce up to310 N of anterior force.1 These large forces are believed toresult in microtrauma that over time may cause adaptivechanges, such as increased laxity of the anterior GH soft tissue
restraints.2,3 This increased laxity may partially explain theincreased GH external rotation repeatedly seen in the throwingarm of baseball players compared with the nonthrowing arm.4,5
Although this increased laxity among baseball players is com-mon, excessive laxity may have several detrimental effects inregard to shoulder dysfunction and injury.6,7 Furthermore, thisincrease in GH laxity is hypothesized to affect the propriocep-tive abilities, such as active joint position sense, of the athlete.8,9
As stated previously, the throwing motion placesa tremendous amount of force on the shoulder joint. Therefore,it is imperative that both the dynamic and static restraints forma synergistic phenomenon to provide the appropriate amount offunctional stability. More specifically, baseball players requireoptimal joint position sense in an effort to repetitively maintainproper throwing mechanics over the course of a game, season,and career. As this joint position sense decreases, so doesthe body’s ability to maintain correct biomechanics duringthe throwing motion placing various structures, including theshoulder, at an increased risk of injury.
Several studies have reported that patients diagnosedwith shoulder instability also present with decreased pro-prioception.8–11 Other studies have noted similar deficienciesin the dominant shoulder of various asymptomatic overheadathletes.12–14 However, no data are currently available detail-ing the effect of adaptive GH laxity among asymptomaticbaseball players and proprioceptive alterations. Therefore,the purpose of this study was to determine the strength ofthe relationship between anterior GH laxity and active jointposition sense in the throwing arm of asymptomatic baseballplayers. Identifying such a relationship may be beneficial forclinicians in the prevention, evaluation, and treatment of var-ious shoulder injuries associated with increased GH laxity.
METHODS
ParticipantsThirty collegiate baseball players (age = 20.2 ± 1.4
years, height = 185.0 ± 5.0 cm, mass = 88.9 ± 9.7 kg) par-ticipated in this study. This group consisted of 13 pitchers and17 position players. At the time of testing, no subjects pre-sented with any recent upper extremity pain or discomfortwithin the past 2 years and no subject had any history ofupper extremity surgery or neurological disorder that mayhave affected their proprioceptive sense.
Each subject voluntarily attended 1 testing session inthe biomechanics laboratory at Illinois State University. Allparticipants provided informed consent as mandated by the
Submitted for publication March 21, 2012; accepted June 26, 2012.From the *School of Kinesiology and Recreation, Illinois State University,
Normal, Illinois; and †Texas Metroplex Institute for Sports Medicine andOrthopedics, Arlington, Texas.
Supported by a grant from the Illinois Association for Health, PhysicalEducation, Recreation and Dance.
Investigation was performed at Illinois State University, Normal, Illinois.Corresponding Author: Kevin G. Laudner, PhD, ATC, Illinois State
University, School of Kinesiology and Recreation, Campus Box 5120,Normal, IL 61790 ([email protected]).
Copyright © 2012 by Lippincott Williams & Wilkins
478 | www.cjsportmed.com Clin J Sport Med � Volume 22, Number 6, November 2012

Illinois State University Institutional Review Board beforetesting (IRB number: 2009-0279). All testing was performedby the same investigators, and no testing was performed afteran extensive throwing session.
InstrumentationThe Biodex System 4 Quick Set (Biodex Medical, Inc,
Shirley, New York) was used to measure shoulder proprio-ception. This device uses a specialized software package,combined with a dynamometer containing strain gauges,potentiometer, and remote range of motion set switches, alongwith several limb attachments, for testing, rehabilitation, anddiagnostic purposes of a variety of joints and muscle groups.
The LigMaster arthrometer (Sport Tech, Inc, Charlottes-ville, Virginia) was used to measure anterior GH laxity. Thisdevice uses a modified Telos GA-II/E stress system andspecialized software to calculate a force–response curve, whichprovides the total amount of soft tissue compression and stiff-ness of the joint restraints. The software is then capable ofcalculating the amount of joint displacement (in millimeters).Previous studies have shown the LigMaster to have both excel-lent within-session reliability [intraclass correlation coefficient(ICC) = 0.84, standard error of the mean (SEM) = 0.53 mm]and between-session reliability (ICC = 0.83, SEM = 0.43 mm)when measuring anterior GH laxity.15
ProceduresShoulder proprioception was assessed by measuring
active joint position sense of the throwing shoulder. Eachsubject was seated in an upright position on the Biodexsystem with their shoulder in approximately 90 degrees ofabduction and the elbow in 90 degrees of flexion. Thedynamometer axis was aligned with the GH joint axis usingan imaginary line running up through the humerus toward thecenter of the shoulder (Figure 1). The shoulder was randomlypositioned in target positions of 75 degrees of external rota-tion, 30 degrees of external rotation, and 30 degrees of inter-nal rotation.16 For these positions, the subject was blindfolded
and passively placed in the appropriate amounts of rotation,as determined by the Biodex software. The subject wasthen asked to concentrate on this target position for 10seconds.13,16,17 After the 10-second concentration period, thetest arm was passively moved away from the target position.Each subject was then asked to actively move their shoulderback to the target position. Practice trials were providedbefore data collection to ensure all subjects were comfortablewith these testing procedures. The absolute amount of errorbetween the target position and the replicated position wasused to determine accuracy of active joint position sense.A total of 3 repetitions for each target position were collected,with the average of these trials used for data analyses.
Anterior GH laxity was measured with the throwingarm in an externally rotated position. For this measurement,each subject was seated with the shoulder in 90 degrees ofabduction and 90 degrees of external rotation, while theelbow was positioned in 90 degrees of flexion and fullpronation. Twelve decanewtons of anterior force was thenapplied to the posterior proximal humerus (Figure 2) at a rateof approximately 1 daN/s. Glenohumeral laxity was deter-mined by taking the difference in displacement between theinflection point, which is calculated by the LigMaster soft-ware as the end of soft tissue compression and the initiation ofhumeral head translation, and the final amount of displace-ment recorded at 12 daN of anterior force.15
Statistical AnalysisA linear regression analysis using SPSS (Version 18.0;
SPSS, Inc, Chicago, Illinois) was used to determine if a relation-ship existed between anterior GH laxity (independent variable)and the 3 proprioception shoulder positions (dependent varia-bles). An alpha level of 0.05 was set before all analyses.
RESULTSThe mean and standard deviation for anterior GH laxity
was 14.1 ± 6.0 mm. The means and standard deviations foramount of error from the target position for 30 degrees of
FIGURE 1. Shoulder proprioception measurement. FIGURE 2. Anterior GH laxity measurement.
Clin J Sport Med � Volume 22, Number 6, November 2012 Relationship Between Laxity and Proprioception
� 2012 Lippincott Williams & Wilkins www.cjsportmed.com | 479

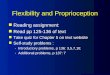
internal rotation, 30 degrees of external rotation, and 75degrees of external rotation are shown in the Table. Indepen-dent t tests showed that there were no differences in propri-oception or GH anterior laxity between pitchers and positionplayers (P . 0.36). There were no relationships betweenanterior GH laxity and active joint position sense at 30degrees of shoulder internal rotation (r = 0.21, P = 0.13)and 30 degrees of shoulder external rotation (r = 0.12, P =0.26) (Table 1). However, there was a moderate positive rela-tionship between anterior GH laxity and joint position senseat 75 degrees of shoulder external rotation (r = 0.56, P =0.001) (Figure 3). Post hoc statistical power was calculatedand showed that external rotation at 75 degrees was shown tohave strong power (0.51), suggesting the clinical usefulnessof this finding.
DISCUSSIONThrowing athletes may present with increased anterior
GH laxity as a result of microtrauma accumulated during thelate cocked position of the throwing motion, which primarilyconsists of GH abduction and external rotation.1 Bothincreased anterior GH laxity and decreased proprioceptionhave been associated with several shoulder injuries.6–10 Theresults of this study suggest that as anterior laxity increases,active joint position sense diminishes when at the largerdegrees of shoulder external rotation.
Active joint position sense is a critical function duringthe throwing motion. This ability allows the athlete toaccurately replicate various positions, like the late cockedposition, throughout the throwing motion in an attempt tomaximize performance and minimize the risk of injury.However, previous research has shown that the shoulderexternal rotators of the throwing arm among baseball playershave neuromuscular imbalances.18 The relationship shown inthe current study between decreased active joint position senseat 75 degrees of shoulder external rotation and increased GHlaxity support these previous findings. However, the findingsof this study did not show a significant relationship when at 30degrees of shoulder external rotation. This is most likely due tothe increased tension placed on the static restraints and poten-tially increased activity of the mechanoreceptors at the higherrange of shoulder external rotation.19 Previous investigationshave shown that mechanoreceptors are not sufficiently stimu-lated during the early ranges of motion.19,20
Our results did not show a significant relationshipbetween anterior GH laxity and joint position sense at 30degrees of shoulder internal rotation. This was not surprising,considering our laxity test position of 90 degrees of shoulderabduction and external rotation followed by an anteriorlydirected force has been shown to stress the anterior inferiorGH ligament21,22 while internal rotation stresses the posteriorcapsule and ligaments.21,22 Future research should investigatethe effect of both increased and decreased laxity of the pos-terior soft tissue restraints and their effect on internal rotationjoint position sense.
These findings may be extremely important in theprevention, evaluation, and treatment of shoulder injuriesrelated to anterior GH laxity among baseball players.Decreased joint position sense during the later degrees ofshoulder external rotation among players with increasedanterior GH laxity could result in a pathological cycleultimately resulting in injury. Lephart et al11 described thispathological cycle between excessive shoulder laxity anddecreased proprioception and neuromuscular control. Theseauthors proposed that as laxity increases, proprioception andthe resulting neuromuscular control are diminished, resultingin a vicious cycle until instability develops. In the case ofthrowing athletes, such as baseball players, if joint positionsense is decreased due to increased anterior GH laxity, thenthe ability to accurately externally rotate the shoulder duringthe late cocking phase of the throwing motion may bereduced. If shoulder external rotation is excessive during thislate cock position, the amount of microtrauma to the anteriorinferior GH ligament may be increased, leading to anincreased risk of instability and injury.
These findings may also be clinically significant amongother overhead athletes who present with increased anteriorGH laxity, such as tennis, volleyball, and softball players.These athletes perform similar motions to the baseball throw,often requiring a large amount of shoulder external rotationbefore ballistic internal rotation resulting in powerful throws,
TABLE. Descriptive Statistics for Absolute Joint Position SenseError
Shoulder TestPosition
Mean ± StandardDeviation, Degrees r
ConfidenceInterval P
Internal rotationat 30 degrees
4.8 ± 2.1 0.21 20.06-0.21 0.13
External rotationat 30 degrees
5.6 ± 2.5 0.12 20.11-0.22 0.26
External rotationat 75 degrees
5.4 ± 2.7 0.56* 0.09-0.32 0.001
*Statistically significant correlation (P , 0.05).
FIGURE 3. Linear relationship between GH laxity and pro-prioception at 75 degrees of external rotation.
Laudner et al Clin J Sport Med � Volume 22, Number 6, November 2012
480 | www.cjsportmed.com � 2012 Lippincott Williams & Wilkins

serves, or spikes of the ball. Swimmers may also present withincreased anterior GH laxity,23 which may be accentuatedduring the recovery phase of the swimming motion as thehand and arm leave the water in preparation for internal rota-tion back to the catch phase.
It is also worth noting that although a moderaterelationship did exist between anterior GH laxity anddecreased proprioception at 75 degrees of shoulder externalrotation, we cannot definitively conclude that increased laxitycauses decreased joint position sense nor vice versa. How-ever, based on previous research that has shown increasedattenuation of the soft tissue restraints, which house themechanoreceptors, to diminish sensory output and ultimatelydecreased propriocption,8–11 it is reasonable to conclude thatthe increased GH laxity most likely lead to the decreasedactive joint position sense in the current study.
As with any study, this investigation has severallimitations. Firstly, although the regression analysis showedthat 56% of the error variance in active joint position sense at75 degrees of shoulder external rotation was explained byanterior GH laxity, there is still a large percent of errorvariance not explained by this laxity. The target positions formeasuring active joint position sense were at 30 degrees ofshoulder internal rotation and 30 degrees and 75 degrees ofexternal rotation. These positions most likely created variousamounts of tension to the GH soft tissue restraints betweenparticipants. For example, 75 degrees of shoulder externalrotation for one subject may be near their end range ofmotion, while this may be in the mid-range of motion foranother. Therefore, we cannot conclude that this positionstressed the ligament equally among all subjects. As such,some subjects may have had more mechanoreceptor activa-tion and thus increased active joint position sense than others.Future research should look at the relationship between GHlaxity and joint position sense with the shoulder at theindividual end range of motion for each subject. Otherpotential causes of this variance may be due to thecontribution of proprioceptive input from other staticrestraints, such as the superior and middle GH ligaments,and dynamic restraints, such as the pectoralis major and longhead of the biceps brachii. Most likely, there were alsoindividual differences in proprioceptive ability betweensubjects adding to variance. Secondly, we only tested thethrowing shoulders of each subject. There may be differencesin proprioception among dominant and nondominant limbs,although we are unaware of any research to date that hasinvestigated this possibility. Thirdly, our active joint positionsense task was conducted in a slow and controlled mannerand cannot be compared with the ballistic rotational speedscreated during the throwing motion. Finally, we testedproprioception in a seated position, which may have affectedthe baseball players’ proprioception. These athletes typicallyare neuromuscularly trained to perform the throwing motionthrough a creation of forces in the lower extremity, which areultimately transferred to the upper extremity and more spe-cifically the throwing arm. It is also worth mentioning thatalthough the use of an arthrometer to measure laxity was nota limitation of our study, clinicians may not have access tosuch equipment. In this situation, the clinician must rely on
their training and experience to measure laxity using standardspecial tests to determine laxity.
CONCLUSIONSThe results of this study show that there is a moderate
relationship between increased anterior GH laxity anddecreased active joint position sense at 75 degrees of shoulderexternal rotation. Therefore, clinicians may use anterior GHlaxity measurements as a partial predictor of active jointposition sense. However, because the subjects used in thisstudy were asymptomatic, a pathologic laxity threshold fordetermining insufficient proprioception was not appropriate.Regardless, these results suggest that it may be important torecognize those players with increasing laxity and incorporateproprioceptive training before the development of injury. Assuch, these results may prove beneficial in the prevention,evaluation, and treatment of various upper extremity injuriesassociated with anterior GH laxity.
REFERENCES1. Fleisig GS, Andrews JR, Dillman CJ, et al. Kinetics of baseball pitching
with implications about injury mechanisms. Am J Sports Med. 1995;23:233–239.
2. Garth WP Jr, Allman FL Jr, Armstrong WS. Occult anterior subluxationsof the shoulder in noncontact sports. Am J Sports Med. 1987;15:579–585.
3. Jobe FW, Giangarra CE, Kvitne RS, et al. Anterior capsulolabral recon-struction of the shoulder in athletes in overhand sports. Am J Sports Med.1991;19:428–434.
4. Sethi PM, Tibone JE, Lee TQ. Quantitative assessment of glenohumeraltranslation in baseball players: a comparison of pitchers versus nonpitch-ing athletes. Am J Sports Med. 2004;32:1711–1715.
5. Laudner KG, Stanek JM, Meister K. Assessing posterior shoulder con-tracture: the reliability and validity of measuring glenohumeral jointhorizontal adduction. J Athl Train. 2006;41:375–380.
6. Greiwe MR, Ahmad CS. Management of the throwing shoulder: cuff,labrum, and internal impingement. Orthop Clin North Am. 2010;41:309–323.
7. Jobe CM. Superior glenoid impingement. Orthop Clin North Am. 1997;28:137–143.
8. Forwell LA, Carnahan H. Proprioception during manual aiming in indi-viduals with shoulder instability and controls. J Orthop Sports Phys Ther.1996;23:111–119.
9. Barden JM, Balyk R, Raso VJ, et al. Dynamic upper limb proprioceptionin multidirectional shoulder instability. Clin Orthop Relat Res. 2004;420:181–189.
10. Zuckerman JD, Gallagher MA, Cuomo F, et al. The effect of instabilityand subsequent anterior shoulder repair on proprioceptive ability.J Shoulder Elbow Surg. 2003;12:105–109.
11. Lephart SM, Warner JP, Borsa PA, et al. Proprioception of the shoulderjoint in healthy, unstable, and surgically repaired shoulders. J ShoulderElbow Surg. 1994;3:371–380.
12. Allegrucci M, Whitney SL, Lephart SM, et al. Shoulder kinesthesia inhealthy unilateral athletes participating in upper extremity sports. JOrthop Sports Phys Ther. 1995;21:220–226.
13. Safran MR, Borsa PA, Lephart SM, et al. Shoulder proprioception inbaseball pitchers. J Shoulder Elbow Surg. 2001;10:438–444.
14. Dover GC, Kaminski TW, Meister K, et al. Assessment of shoulderproprioception in the female softball athlete. Am J Sports Med. 2003;31:431–437.
15. Crawford SD, Sauers EL. Glenohumeral joint laxity and stiffness in thefunctional throwing position of high school baseball pitchers. J AthlTrain. 2006;41:52–59.
16. Chu JC, Kane EJ, Arnold BL, et al. The effect of a neoprene shoulderstabilizer on active joint-reposition sense in subjects with stable andunstable shoulders. J Athl Train. 2002;37:141–145.
Clin J Sport Med � Volume 22, Number 6, November 2012 Relationship Between Laxity and Proprioception
� 2012 Lippincott Williams & Wilkins www.cjsportmed.com | 481

17. Brindle TJ, Uhl TL, Nitz AJ, et al. The influence of external loads onmovement precision during active shoulder internal rotation movementsas measured by 3 indices of accuracy. J Athl Train. 2006;41:60–66.
18. Brindle TJ, Nyland J, Shapiro R, et al. Shoulder proprioception: latentmuscle reaction times. Med Sci Sports Exerc. 1999;31:1394–1398.
19. Clark FJ, Grigg P, Chapin JW. The contribution of articular receptors toproprioception with the fingers in humans. J Neurophysiol. 1989;61:186–193.
20. Burke D, Gandevia SC, Macefield G. Responses to passive movement ofreceptors in joint, skin and muscle of the human hand. J Physiol. 1988;402:347–361.
21. Warner JP, Caborn DN, Berger R, et al. Dynamic capsuloligamentousanatomy of the glenohumeral joint. J Shoulder Elbow Surg. 1993;2:115–133.
22. Urayama M, Itoi E, Hatakeyama Y, et al. Function of the 3 portions ofthe inferior glenohumeral ligament: a cadaveric study. J Shoulder ElbowSurg. 2001;10:589–594.
23. Jansson A, Saartok T, Werner S, et al. Evaluation of general jointlaxity, shoulder laxity and mobility in competitive swimmers duringgrowth and in normal controls. Scand J Med Sci Sports. 2005;15:169–176.
Laudner et al Clin J Sport Med � Volume 22, Number 6, November 2012
482 | www.cjsportmed.com � 2012 Lippincott Williams & Wilkins