Embed Size (px)
Citation preview

Latest news in MS Treatment and Research
(Helicopter / Hot Air Balloon View)
Gavin GiovannoniBarts-MS

DisclosuresProfessor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that no personal identifiers were collected as part of these surveys and that by completing the surveys participants consented for their anonymous data to be analysed and presented by Professor Giovannoni.
Professor Giovannoni would like to acknowledge and thank Biogen, Genzyme and Roche for making available data slides on natalizumab, daclizumab, alemtuzumab and ocrelizumab for this presentation.
Please note that Professor Giovannoni trip to Aarhus has been kindly sponsored by Novartis, Denmark.

24th
Jun
e 20
16
Apologies from a Bremain supporter!



Grayson Perry

Themes
1. Disruptive technologies
2. Challenging the current dogma
3. A changing worldview of MS
4. Preventing MS

24th
Jun
e 20
16
Disruptive Technologies

Changing Worldview of Healthcare

Democratization of Knowledge and Healthcare
www.ms-res.org


24th
Jun
e 20
16
Field Hypothesis

Predictors of long-term outcome in MSers treated with interferon beta-1a
Bermel RA, et al. Ann Neurol 2013;73:95-103.

Predictors of long-term outcome in MSers treated with interferon beta-1a
Treatment vs. Natural HistoryBermel RA, et al. Ann Neurol 2013;73:95-103.


MS Field Hypothesis
Barnett & Prineas. Ann Neurol 2004;55:458–468 Filippi et al. Ann Neurol 1998;43:809-814

24th
Jun
e 20
16
Politics



20
0 20 40 60 80 100
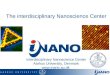
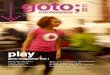
Large disparities exist in access to disease-modifying therapies
DMT, disease-modifying therapy. 1. Hollingworth S et al. J Clin Neurosci 2014;21:2083–7; 2. World Bank, 2015. http://data.worldbank.org/indicator/SP.POP.TOTL; 3. MSIF, 2013. http://www.atlasofms.org; 4. Wilsdon T et al. 2013. http://crai.com/sites/default/files/publications/CRA-Biogen-Access-to-MS-Treatment-Final-Report.pdf. Figure reproduced from Giovannoni G et al. Brain health: time matters in multiple sclerosis. Available at: www.msbrainhealth.org
Newer DMTEstablished DMTNo DMT
All people with MS (%)
All data are from 2013
4
4
4
4
4
4
4
4
4
4
4
4
4
1–3
Established DMTsDMTs approved for relapsing forms of MS during the 1990s and reformulations or generic versions of these substances
Newer DMTsDMTs approved for relapsing forms of MS that have a different mechanism of action from established DMTs



Anti-ageing
• Smoking• Exercise• Diet• Alcohol• Sleep• Co-morbidities• Infections• Concomitant medications
• ? Menopause / HRT
Brain Health

24th
Jun
e 20
16
Progressive MS

25
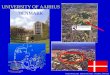
Window of therapeutic efficacy

Disability progression in two phases
In RRMS, gender, age at onset, residual deficit after the first relapse, and relapses during the first 2 years are independent predictors of disability progression only in phase 1
DSS
Sco
re
Years from clinical onset of MS
65432100 5 10 15 20 25 30
7
Phase 2
Phase 1
Natural History
Leray E et al. Brain 2010;133:1-14.

Therapeutic lag hypothesis
therapeutic lag

nalysis between year 2 versus year 3
Biogen Idec data on file.


30
n=140 n=93 n=80n=143
Prop
ortio
n of
pa
tient
s (%
)
PlaceboNatalizumab
**P=0.0088 **P=0.0019 P=0.8259
n=47 n=63 n=140 n=93 n=80n=143Pr
opor
tion
of
patie
nts
(%)
*P=0.0349 **P=0.0048 P=0.5976
n=47 n=63
Lublin F. et al. ECTRIMS 2013, Copenhagen October 3rd , Poster P524.
Disabling Magnitude of Relapses in AFFIRM EDSS change from pre-relapse to at relapse


32
…









n=130
www.ms-res.org
96%

www.ms-res.org

24th
Jun
e 20
16
Emerging DMTs&
‘New hypotheses’

Highly-effective DMTs

Ocrelizumab in PPMS TrialReduction in confirmed disability progression for ≥12 WeeksPrimary Endpoint
nPlacebo 244 232 212 199 189 180 172 162 153 145 136 120 85 66 46 30 20 7 2Ocrelizumab 487 462 450 431 414 391 376 355 338 319 304 281 207 166 136 80 47 20 7
45
Time to CDP for ≥12 weeks
Analysis based on ITT population; p-value based on log-rank test stratified by geographic region and agePatients with initial disability progression who discontinued treatment early with no confirmatory EDSS assessment were considered as having confirmed disability progression



Daclizumab High-Yield Process (DAC HYP): First in Class IL-2 Immunomodulator
IL2Rβ(CD122) γcommon
(CD132)
αIL-2
βγ
α IL-2
βγ
High AffinityIL-2 ReceptorIL2Rα
(CD25)
CD, cluster of differentiation; IL, interleukin; NK, natural killer.1. Depper JM et al. J Immunol. 1983;131:690-696; 2. McDyer JF et al. J Immunol. 2002;169:2736-2746; 3. Wuest SC et al. Nat Med. 2011;17:604-610; 4. Bielekova B. Proc Natl Acad Sci. 2006;103:5941-5946; 5. Martin JF et al. J Immunol. 2010;185:1311-1320; 6. Perry JSA et al. Sci Transl Med. 2012;4:145ra106.
Intermediate AffinityIL-2 Receptor
•DAC HYP selectively blocks the high-affinity IL2R by binding the α subunit (CD25)
•Promotes a shift of IL-2 signaling towards the intermediate-affinity IL-2R
Biological impact of DAC HYP
• Inhibition of activated T cell responses1−3
•Expansion of CD56bright NK cells4,5
•Normalization of lymphoid tissue inducer cell numbers6

DECIDE: daclizumab HYP vs. interferon β-1a in RRMS Annualized Relapse Rate (ARR)
45% Reduction (95% CI: 35.5%, 53.1%)
p<0.0001
(n=922) (n=919)
A R R
Estimated from a negative binomial regression model adjusted for baseline relapse rate, history of prior IFN beta use, baseline EDSS (≤2.5 vs > 2.5) and baseline age (≤35 vs >35). Patients were censored at the earliest of the following events: 1) start of alternative MS medication, 2) 180 days post treatment discontinuation or 3) end of treatment period. CI, confidence interval.
Kappos et al. AECTRIMS 2014

• Reductions in lesions (T2, Gd+, and T1) were observed as early as 24 weeks for DAC HYP vs IFN beta-1a (p<0.001 for all comparisons)
DECIDE: daclizumab HYP vs. interferon β-1a in RRMS Effect on MRI-defined lesions at Week 96
*Adjusted mean for T2 and T1 lesions. †The number of new/newly enlarging T2 lesions at 96 weeks was a secondary endpoint. Data were adjusted for baseline lesion volume, history of prior IFN beta-1a use and baseline age (≤35 v >35). Missing data were not imputed and patients with no post baseline MRI were excluded from analysis of new/newly enlarging T2 lesions at 96 weeks. Missing data were imputed for all other analyses.
New T1 Hypointense Lesions‘black holes’
52% Reductionp<0.0001
New Gd+ Lesions
65% Reductionp<0.0001
IFN beta-1a 30 mcg DAC HYP 150 mg
n=908n=841 n=864 n=909 n=900 n=899
Mea
n* n
umbe
r of
lesi
ons
New/Newly Enlarging T2 Lesions†
54% Reductionp<0.0001
n=864n=841
Kappos et al. AECTRIMS 2014

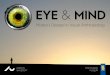
DECIDE: daclizumab HYP vs. interferon β-1a in RRMS 3-Month and 6-Month Confirmed Disability Progression
Risk reduction: 16%; p=0.16
Proportion with progressionWeek 48: 6% vs. 8% Week 96: 12% vs. 14% Week 144: 16% vs. 20%
BL 12 24 36 48 60 72 84 96 108 120 132 144Time on study (weeks)
BL 12 24 36 48 60 72 84 96 108 120 132 144Time on study (weeks)
Risk reduction: 27%; p=0.0332
Proportion with progressionWeek 48: 4% vs. 7% Week 96: 9% vs. 12% Week 144: 13% vs. 18%
3-month* 6-month†
Prop
ortio
n of
pat
ient
s w
ith
conf
irmed
pro
gres
sion
of
dis
abili
ty
*3-month confirmed: Patients censored after tentative progression (n=67) analyzed per primary method in the statistical analysis plan: all imputed as non-progressors; †6-month confirmed: Patients censored after tentative progression (n=108) imputed per observed rate in trial; tertiary endpoint. Estimated proportions are the average over imputed datasets. For both endpoints risk reductions based on Cox proportional hazards model adjusted for baseline EDSS, history of prior IFN use, and age. Kappos et al. AECTRIMS 2014

Effect of Anti-CD25 Antibody Daclizumabin the Inhibition of Inflammation and
Stabilization of Disease Progression in MS
Bielikova et al. Arch Neurol. 2009;66(4):483-489

Monoclonal antibody blockade of IL-2 receptor during lymphopenia selectively depletes regulatory T cells in mice and humans
Kappos et al. Blood 2011;118(11):3003-3012.

24th
Jun
e 20
16
Prevention



→
≥




Questions• Need a vaccine
– GSK / Medimmune gp350– NIH new initiative
• Age group– Childhood, adolescence, early adulthood
• Vaccine programme– Piggy-back on HPV programme
• Comparator– Placebo
• Primary outcome– IM
• Secondary outcome– Population surveillance (autoimmune / oncology)


Conclusions∙ Technology is disrupting MS Services∙ Old insights, new hypothesis∙ Field hypothesis
∙ Brain Health & Politics∙ Progressive MS ∙ Length-dependent axonopathy
∙ Emerging DMTs∙ Anti-CD20 (ocrelizumab & ofatumumab)∙ Anti-CD25 (daclizumab)
∙ Prevention∙ vD∙ EBV∙ Smoking

24th
Jun
e 20
16
Questions

Biology
Clinical outcomes
Biomarkers