Embed Size (px)
Citation preview

Laboratory Tests in psychiatry
Presented by Dr.Monirul Islam
Resident,MD(Phase-B) Dept.of psychiatry
BSMMU

A medical laboratory is a place where tests are done on clinical specimens and samples in order to get information about the health of a patient as pertaining to the diagnosis, treatment, and prevention of disease
Laboratory Services include testing of materials, tissues or fluids obtained from a patient or clinical studies to determine the cause and nature of disease

Medical Laboratories
Clinical Pathology Clinical Microbiology Clinical Biochemistry
Haematology
Histopathology
Cytology
Routine Pathology
Bacteriology
Mycobacteriology
Virology Mycology
Parasitology
Immunology
Serology
Biochemical analysis
Hormonal assays

What are Laboratory Services all about?
Laboratory Services play a critical role in the detection, diagnosis and treatment of disease. Samples are collected and examination and analysis of body fluids, tissue and cells are carried out. Main services are:
To Perform diagnostic tests To Identify organisms To Count and classify blood cells to identify
infection or disease To Perform immunological tests to check for
antibodies To Type and cross-match blood samples for
transfusions To Analyze DNA

Health Screening
• Programs to detect
important (and treatable)
disease in apparently
healthy individuals

Types of Screening
• Population
• Risk group
• Opportunistic

Principles for Screening Programs
1. There should be a recognizable early or latent stage
2. There should be an accepted treatment for the condition
3. The screening test is valid, reliable
4. The test must be acceptable to population to be screened
5. Cost of screening and case finding should be economically balanced in relation to medical care as a whole

Attributes of Test
Sensitivity
Specificity
Safety
Cost-effectiveness

Check-Up for a 50-Yr Woman
• BP measurement
• Fasting blood glucose
• Fasting lipid profile
• Pap’s smear
• Mammography
• FOBT
– Colonoscopy: F/H of colon Ca
• Vision & hearing
Ref: Harrison's
Internal Medicine

Check-Up for a 50-Yr Man
• BP measurement
• Fasting blood glucose
• Fasting lipid profile
• DRE/PSA
• FOBT
– Colonoscopy: F/H of colon Ca
• Vision & hearing
Ref: Harrison's Internal
Medicine

Benefits
• A primary goal of screening is the early
detection of a risk factor or disease at a
stage when it can be corrected or cured
• More effective treatment
– Improved quality of life
– Prolongation of survival

Adverse Consequences of Screening
• Not all are evidence-based
• Generates a number of false positive results
– Require further expensive & risky
investigations
– Anxiety in patient & family
– Dilemmas in the clinician

BASIC SCREENING TESTSCBCECGLiver function testRenal function testThyroid function testElectrolytesBlood sugarAim: ruling out organicity Ref: Kaplan & Sadock's Synopsis of
Psychiatry

Principles of endocrine tests
Timing of measurement: Release of many hormones is rhythmical(pulsatile, circadian, monthly)random test may be invalid, sequential/dynamic test may be required.
Choice of dynamic tests: -If deficiency suspected: stimulation test -If excess suspected: suppression test -Avoid interpreting one result in isolationImaging,Biopsy: may be needed

Thyroid Function TestsIndications:-MDD,BMD -Hypothyroidism -Hyperthyroidism -Lithium-induced hypothyroidism TFTs : First-line: S.TSH,T3,T4 Second-line: TSH receptor
antibody Isotope scanningSensitivity : T4>T3

Interpretation of TFTs TSH T4 T3 Interpretation
U.D. (Undetectable)
Raised Raised Primary thyrotoxicosis
U.D. Normal Raised Primary T3-toxicosis
U.D. Normal Normal Subclinical thyrotoxicosis
U.D. Raised Low,normal or raised
Sick euthyroidism
Elevated >20 mu/L
Low Low Primary hypothyroidism
Mildly5-20 mu/L
Normal Normal Subclinical hypothyroidism
20-500 mu/L
Normal Normal Artefact

Non-specific laboratory abnormalities in thyroid dysfunction
Thyrotoxicosis: • Alanine aminotransferase, γ-glutamyl transferase
(GGT), and alkaline phosphatase from liver and bone • bilirubin • Mild hypercalcaemia • Glycosuria
Hypothyroidism: • Creatine kinase, aspartate aminotransferase, LDH • Hypercholesterolaemia • Anaemia
– Normochromic normocytic or macrocytic • Hyponatraemia

Dexamethasone-suppression test
• Indication: Supporting Dx of MDD.• Procedure: pt is given 1mg of D.methasone
by mouth at 11pm & plasma cortisol is measured at 8am,4pm,11pm.
• Result: -Nonsuppression:cortisol>5mg/dl -Suppression: HPA-axis is normal• Nonsuppression is associated with stress.• Limitation: False +ve & -ve, Low sensitivity

Dexamethasone-suppression test
Importance: 1.+ve DST,Good response to ECT or TCA 2.To differentiate MDD from minor
dysphoria 3.Predicting outcome of treatment 4.Predicting relapse:Persistent
nonsuppression 5.Differenting delusional from
nondelusional MDD 6.High abnormal cortisol >10µg/dl are
more significant than mildly elevated level

Hyperprolactinaemia• Causes: A.Physiological:-stress –pregnancy -
exercise -Lactation –sleep -coitus B.Drug-induced: Dopamine antagonists -antipsychotics -antiematics:Domperidone Dopamine-depleting drugs -methyldopa
C.Pathological:Prolactinoma,PCOS,primary hypothyroidism,renal failure

Hyperprolactinaemia• C/F: Male:sex.dysfunction,infertility,breast
growth,bone mineral density. Female:Amenorrhoea,galactorrhoea• Monitoring: -ask prolactin-related
symptoms - prolactin level:at prescribing at 3 months yearly• Avoid prolacting-elevating drugs: -pt under 25yrs –pt with osteoporosis -pt with H/O breast cancer

Hyperprolactinaemia Prolactin concentration interpretation: Take blood sample at least one hour
after waking or eating Minimise stress during venepuncture
(stress elevates plasma prolactin) Normal : Women :0–25 ng/ml
Men :0–20 ng/mlRe-test: if prolactin concentration 25–100
ng/ml ( 530–2120 mIU/l)Referral :to rule out prolactinoma if
prolactin concentration>150 ng/ml (>3180 mIU/l)

Hyperprolactinaemia
Established antipsychotics not usually associated with hyperprolactinaemia
• Aripiprazole• Clozapine• Olanzapine• Quetiapine• Ziprasidone

HyperprolactinaemiaTreatment: Switch to a non prolactin-elevating
drug is the first choice An alternative is to add aripiprazole
to existing treatment For patients who need to remain on a
prolactin-elevating antipsychotic,dopamine agonists may be effective Amantadine, carbergoline and bromocriptine,but each has the potential to worsen psychosis.

Psychiatric Disorders No laboratory tests in psychiatry can confirm or
rule out diagnoses Psychiatrists depend more on the history, clinical
examination and MSE to make a diagnosis • Investigations: 1.Routine: -FBC, U&Es, LFTs, TFTs,RFTs, RBS,CXR, ECG 2.Special: (if indicated by history or physical
signs) -Urine toxicology -Antinuclear antibody(SLE) -Syphilis serology -CT/MRI, EEG, LP -HIV testing

DM & AntipsychoticsSchizophrenia: Associated with
Insulin resistance & Diabetes mellitus.
Mechanism: -Not clear -5HT antagonism -increase plasma lipids -Wt gain -Leptin resistance

A1C ≥6.5%OR
Fasting plasma glucose (FPG)≥126 mg/dL (7.0 mmol/L)
OR
2-h plasma glucose ≥200 mg/dL(11.1 mmol/L) during an OGTT
OR
A random plasma glucose ≥200 mg/dL (11.1 mmol/L)
Criteria for the Diagnosis of Diabetes
ADA. I. Classification and Diagnosis. Diabetes Care 2012;35(suppl 1):S12. Table 2.

Criteria for Testing for Diabetes in Asymptomatic Adult Individuals (1)
•Physical inactivity• First-degree relative with diabetes• High-risk race/ethnicity (e.g., African
American, Latino, Native American, Asian American, Pacific Islander)• Women who delivered a baby weighing >9 lb
or were diagnosed with GDM• Hypertension (≥140/90 mmHg or on therapy
for hypertension)*At-risk BMI may be lower in some ethnic groups.
Testing should be considered in all adults who are overweight (BMI ≥25 kg/m2*) and who have one or more additional risk factors:

Criteria for Testing for Diabetes in Asymptomatic Adult Individuals (1)
• HDL cholesterol level<35 mg/dL (0.90 mmol/L) and/or a triglyceride level >250 mg/dL (2.82 mmol/L)• Women with polycystic ovarian syndrome (PCOS)• A1C ≥5.7%, IGT, or IFG on previous testing• Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans)• History of CVD
*At-risk BMI may be lower in some ethnic groups.

1. In the absence of risk factors testing for diabetes should begin at age 45 years
2. If results are normal, testing should be repeated at least at 3-year intervals, with consideration of more frequent testing depending on initial results (e.g., those with prediabetes should be tested yearly), and risk status
ADA. Testing in Asymptomatic Patients. Diabetes Care 2012;35(suppl 1):S14. Table 4.
Criteria for Testing for Diabetes in Asymptomatic Adult Individuals (2)

Categories of increased risk fordiabetes (prediabetes)
A1C: 5.7%-6.4%
Impaired Fasting Glucose(IFG) FPG: 5.6-6.9 mmol/L (100-125mg/dl)
Impaired Glucose Tolerance (IGT) 2-h value in OGTT: 7.8-11.0 mmol/L (140-199mg/dl)

Monitoring:Pt receiving antipsychotics
TIME IDEAL TEST MINIMUM TEST
Base lineOGTT or FPGHBA1C if fasting not possible(+RBS)
Urine glucoseRBS
Continuation All Drugs:OGTT or FPG or HBA1C every 12months (+RBS)
Olanzapine,Clozapine: OGTT or FPG after 1 month,then every 4-6 months
Urinary glucose or RPG every 12 months + symptoms monitoring

Risk of DM with antipsychotics
Degree of risk Antipsychotics
High Clozapine,Olanapine
Moderate Quetiapine,Risperidone,Phenothiazines
Low High potency FGAs: Haloperidole
Minimal Aripiprazole,Amisulpride,AsenapineZiprasidone

DyslipidaemiaCAUSES OF SECONDARY HYPERLIPIDAEMIA Secondary hypercholesterolaemia - Hypothyroidism -Pregnancy -Drugs (antipsychotics, corticosteroids) -Nephrotic syndrome -Anorexia nervosa Secondary hypertriglyceridaemia -Diabetes mellitus (type 2) -Abdominal obesity -Excess alcohol -Drugs (β-blockers, retinoids, corticosteroids)

Antipsychotics & Dyslipidaemia
FGAs: -Phenothiazines: TG, LDL,HDL
-Haloperidole: minimal effects
SGAs: -Mild: Aripiprazole,Ziprasidone
May even reverse -
Moderate:Risperidone,Quetiapine -Severe: Olanzapine,Clozapine

Monitoring
Antipsychotics drugs
Suggested monitoring
Clozapine and Olanzapine
Fasting lipid at baseline,then every 3 months for a year,then annually.
Other antipsychotics Fasting lipid at baseline,then at 3 months, then annually.

HyponatraemiaCauses of hyponatraemia Treatment
Water intoxication Monitor serum sodium( as day progress)Fluid restrictionCareful use of IVsaline:RhabdomyolysisConsider treatment with clozapineRefer if Na<125 mmol/L
SIADH: Associated with all antipsychotics
Monitor serum sodiumFluid restrictionSwitch to different antipsychoticsRefer if Na<125 mmol/L
Severe hyperlipidaemia and/or hyperglycaemia
PseudohyponatraemiaTreat the cause

Antidepressant-induced hyponatraemia
• Most antidepressants have been associated with hyponatraemia
• Onset:is usually within 30 days of starting treatment
• not dose-related • The mechanism:probably the
syndrome of inappropriate secretion of antidiuretic hormone (SIADH); serotonin is thought to be involved in the regulation of ADH release

Antidepressant-induced hyponatraemia
MONITORING: • pt taking antidepressants:observe signs of
hyponatraemia Serum sodium should be determined :at
baseline 2 & 4 wks
• and then 3-monthly those at high risk The high-risk factors are as follows: - extreme old age (>80 years) - history of hyponatraemia - co-therapy with drugs associated with
hyponatraemia - reduced renal function (GFR <50 ml/min) - medical co-morbidity common in elderly patients so monitoring is
essential

Anorexia nervosaEndocrine: -LH,FSH,T3,RBS -GH,CortisolHaematological: -Normocytic normochromic
anaemia -Thrombocytopenia -Leucopenia with
rel.LymphocytosisMetabolic: -Hypercholesterolaemia -HypophosphataemiaOthers: -Electrolytes imbalance

Sexual dysfunction
• Should be arranged according to cause ED: -FBS -Testosterone -SHBG -LH/FSH
-Prolactin -Thyroid Function -PSA
-S. Lipid profile

Lab Test: FSAD• Depends on relevent symptoms• If low desire suspected along with
arousal: S.Testosterone, SHBG• If menopausal (vaginal dryness) state – S. Estrogen
• If comorbid with marked oligomenorrhoea– S. Prolactin
• Thyriod Status if clinical history suggest

NMS
NMS is rare,even fatal outcome of antipsychotics
Incidence:0.2% of pt taking antipsychotics
Onset: often first 10 days of treatmentLab findings: - Creatinine
phosphokinase - WBC - Alter LFT

Pre-anaesthetic check prior to ECT
ECT work-up:-CBC -ECG -Liver function test -Renal function test -Electrolytes -Blood sugar -Vital signs:pulse,BP,tem,RR -Check no medication or seizure threshold

Rapid tranquillisation
The clinical practice of RT is used to de-escalate acutely disturbed
behaviour
The aims of RT are : 1. To reduce suffering for the patient 2. To reduce risk of harm to others 3. To do no harm

RT:monitoring After any parenteral drug administration,
monitor as follows: Pulse Blood pressure Temperature Respiratory rate Time: Every 5–10 min for 1 hour, and then half-
hourly until patient is ambulatory. If pt is asleep or unconscious :use pulse
oximetry ECG and haematological monitoring:strongly
recommended when parenteral antipsychotics are given
Hypokalaemia, stress and agitation place the patient at risk of cardiac arrhythmia
ECG monitoring :for all patients who receive haloperidol.

Substances of Abuse That Can Be Tested in Urine
Substance Length of Time Detected in Urine
Alcohol 7-12 hours
Amphetamine 2 days
Barbiturate 1 day (short-acting) 3 weeks (long-acting)
Benzodiazepine 3 days
Cannabis 3 days to 4 weeks (depending on use)
Cocaine 6-8 hours (metabolites 2-4 days)
Codeine 2 days
Heroin 36-72 hours
Methadone 3 days
Morphine 2-3 days

Plasma level monitoring of psychotropics
Is there a clinically useful assay method available? Is the drug at ‘steady state’? Is the timing of the sample correct? Is there a target range of plasma levels? Is there a clear reason for plasma level
determination? Only the following reasons are valid: – to confirm compliance – if toxicity is suspected – if drug interaction is suspected – if clinical response is difficult to assess directly – if the drug has a narrow therapeutic index and
toxicity concerns are considerable.

Interpreting sample results
Drug Target range Sample timing Time to steady state
Aripiprazole
150–210 µg/L Trough 15–16 days
Clozapine
350–500 µg/L Trough 2–3days
Lithium 0.6–1.0 mmol/L(may be >1.0 mmol/L in mania)
12 hours post-dose
5-7 days
Olanzapine
20–40 µg/L 12 hours post-dose
1 week
Tricyclics Nortriptyline :50–150 µg/LAmitriptyline: 100–200 µg/L
Trough 2–3 days
Valproate 50–100 mg/L Trough 2–3 days

TCAIndication for plasma
monitoring: 1.To check compliance 2.Toxic side effect at low dose 3.Lack of therapeutic response
4.Doses>200mg 5Coexisting medical
illness(e.g.Epilepsy) 6.Possibility of drug interaction

Clozapine Many adverse effects are dose-dependent & more
common at beginning of treatment Target dose: Average dose is around 450mg/day Response seen in the range 150–900 mg/day Plasma levels : Response is in range 350–420 µg/L Mandatory blood monitoring and registration - Register with the relevant monitoring service. -Perform baseline blood tests (WCC and
differentialcount) before starting clozapine. -first 18 weeks=Weekly -remainder of the year=2 weekly -After that= monthly Stop cloapine: WBC<3000 OR Neutrophil<1500 per
mm3

Clozapine Additional monitoring: -Wt -Lipid profile -LFTs -Plasma glucose -BMI -Waist
Timing: at 1,3,6 and 12 months.

Clozapine:MyocarditisTime/condition Monitor
Baseline Pulse,tem,RR,CRP,Troponin,Echo
Daily Pulse,tem,RR
Days 7,14,28 CRP,Troponin
If CRP>100mg/L,Troponin>twice upper limit
Stop cloapine,repeat Echo
If fever+tachycardia+CRP OR Troponin
CRP and Troponin daily

LithiumPre-Lithium work-up: 1.Physical examination: BP,
Wt 2.RFT: eGFR,Creatinine or
CCr 3.TFT 4.CBC 5.ECG 6.Pregnancy test-if indicated

LithiumOn treatment monitoring: 1.Plasma lithium: -First after 7 days -Then weekly=3weeks -Once every 6 week -Then 2-3 months. 2.e-GFR & TFTs : every 6 months 3.BMIPlasma level: Acute mania: 0.8-1 mmol/L Prophylactic: 0.5-0.8 mmol/L Toxicity: >1.5 mmol/LNarrow therapeutic index: Lithium toxicity

Lithium Toxicity1.Mild to moderate intoxication (lithium level = 1.5 to 2.0 mEq/
GI Vomiting,Abdominal pain
Neurologic Ataxia,Dizziness,Slurred speechNystagmus,Lethargy or excitementMuscle weakness
2,Moderate to severe intoxication (lithium level = 2.0 to 2.5 mEq/L)
GI AnorexiaPersistent nausea and vomiting
Neurologic Blurred vision,Muscle fasciculationsClonic limb movementstendonreflexes,Convulsions,Delirium,SyncopeStupor,Coma,Circulatory failure
3.Severe lithium intoxication (lithium level >2.5 mEq/L)
Generalized convulsions , Oliguria renal failure, Death

Management of Lithium Toxicity
Lithium must be stoped at onceHigh intake of fluid,maintenance of
electrolyte balanceExamination :vital signs,neuro. Exam, MSELab:Lithium level,serum
electrolytes,RFTs,ECG Acute ingestion:gastric lavage,activated
charcoalOsmotic or forced alkaline diuresis should be
used . NEVER thiazide or loop diuretics Lithium level >3.0 mEq/L: haemodialysis Repeat dialysis :every 6 to 10 hours, until
the lithium level is within nontoxic range

Instructions to Pt Taking Lithium
DosingTake lithium exactly as directed by your doctore.Do not stop taking without speaking to your doctor.If you miss a dose, take it as soon as is possible. If it is within 4 hours of the next dose, skip the missed dose. Never double up doses.
Blood TestsComply with the schedule of recommended regular blood tests.you should have taken your last lithium dose 12 hours earlier.
Use of Other MedicationsDo not start any prescription without telling your doctor
Diet and Fluid IntakeAvoid sudden changes in your diet or fluid intake. If you do go on a diet, inform your doctor.Caffeine and alcohol act as diuretics and can lower your lithium concentrations.it is recommended that you drink about 2 or 3 quarts of fluid daily, and use normal amounts of salt.
Recognizing Potential ProblemsIf you engage in vigorous exercise or have an illness that causes sweating, vomiting, or diarrhea, consult your doctor.Pt is educated about early signs of lithium toxicity

Lithium & eGFR• Indication for referral to specialist in pt
taking Lithium: 1.eGFR is decreased by >4 ml/min
annually 2.Progressive rise in creatinine in 3 or
more serial test 3.Proteinuria 4.Haematuria 5.Symptoms of CRF(Anaemia,tiredness) 6.e-GFR <30 ml/min

Valproate:MonitoringIndications Mania, hypomania, bipolar depression and
prophylaxis of bipolar affective disorder.Note that sodium valproate is licensed only for epilepsy and semi-sodium valproate only for acute mania
Pre-valproate work up
FBC and LFTs. Baseline measure of weight
Prescribing Loading doses can be used and are generally well tolerated. CR sodium valproate can be given once daily. All other formulations must be administered at least twice dailyPlasma levels can be used to assure adequate dosing and treatment compliance. Blood should be taken immediately before the next dose
Monitoring As a minimum, FBC and LFTs after 6 monthsWeight (or BMI) should also be monitored
Stopping Reduce slowly over at least 1 month
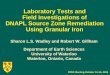
Lab Monitoring:Carbamazepine Test Frequency
Complete blood count (CBC) Before treatment and every 2 weeks for the first 2 months of treatment; thereafter, once every 3 months
Platelet count and reticulocyte count
Before treatment and yearly
Serum electrolytes Before treatment and yearly
Electrocardiogram Before treatment and yearly
SGOT,SGPT,LDH Before treatment and every month for the first 2 months of treatment; thereafter, every 3 months
Pregnancy test for women of childbearing age
Before treatment and as frequently as monthly in noncompliant patients

Other Laboratory TestsTest Major
Psychiatric Indications
Comments
Adrenocorticotropic hormone (ACTH)
Organic workup
Increased in steroid abuse; may be increased in seizures, Cushing's disease, and in response to stressDecreased in Addison's disease
Alanine aminotransferase (ALT)
Organic workup
Increased in hepatitis, cirrhosis, liver metastasesDecreased in pyridoxine (vitamin B6) deficiency
Antinuclear antibodies
Organic workup
Found SLE and drug-induced lupus (e.g., secondary to phenothiazines, anticonvulsants)

Other Laboratory TestsTest Major
Psychiatric Indications
Comments
Calcium (Ca) Organic workupMood disordersPsychosisEating disorders
Increased in hyperparathyroidism,delirium, depression, psychosisDecreased in hypoparathyroidism, long-term laxative use
Catecholamines urinary and plasma
Panic attacksAnxiety disorders
Elevated in pheochromocytoma
Ceruloplasmin, copper, serum
Organic workup Low in Wilson's disease

Other Laboratory TestsTest Major
Psychiatric Indications
Comments
Cortisol Organic workupMood disorders
Excessive level may indicate Cushing's disease associated with anxiety, depression
Estrogen Mood disorder Decreased in menopausal depression and premenstrual syndrome
Glutamyl transaminase, serum
Alcohol abuseOrganic workup
Increased in alcohol abuse, cirrhosis, liver disease
Folate (folic acid), serumVitamin B12, serum
Alcohol abuseDementia
associated with dementia, deliriumalcohol dependence, use of phenytoin, oral contraceptives

Other Laboratory TestsTest Major
Psychiatric Indications
Comments
Holter monitor Panic disorder Evaluation of panic-disorder patients with palpitations and other cardiac symptoms
Nocturnal penile tumescence
Erectile disorder
Helpful in differentiation between organic and functional causes of impotence
Testosterone, serum
ImpotenceHypoactive sexual desire disorder
Increased in anabolic steroid abuseMay be decreased in impotenceDecrease may be seen in hypoactive sexual desire disorder

Take Home MessageNo laboratory tests in psychiatry can
confirm or rule out diagnosesHealth screening should be done in all
psychiatric pt to exclude organicityTFTs are used to rul out hypothyroidism
which can appear as MDDDST:help confirm diagnostic impression
of MDDAlways check for Metabolic syndrome
patient taking psychotropicsLab tests should be arranged according
to cause in sexual dysfunction
Take Home Message• Urine test is an important test for
substance abuser• Be sure that pt is fit biochemically
for giving anaesthesia in ECT• Drug level monitoring help in
optimising treatment & assure adherence
• Treat the patient,not the level• ECG and haematological monitoring:
strongly recommended when parenteral antipsychotics are given

Take Home Message
• Clozapine is associated with myocarditis and cardiomyopathy
• ANC is mandatory blood monitoring for clozapine
• Be aware about psychotropics induced electrolytes imbalance
• RFTs,TFTs are most important Pre-Lithium work-up
• Lithium toxicity is a medical emergency often having fatal outcome