Embed Size (px)
Citation preview

July 4th, 2008
Multi Sectoral SAA ConsultationCommunity Support Services

Overview
• Multi Sectoral SAA Consultation - The Approach
• Roles and Responsibilities
• M-SAA an Overview • Performance Indicators
• Timelines
• Discussion

The Approach

Multi Sectoral SAAs• Requirement under LHSIA and MLAA
• Vehicle to delineate accountabilities and performance expectations
• Tool to support the health care transformation agenda
• Build on existing agreements where possible
• Consistent template agreement for all Sectors supported by schedules
• To be developed through consultation on the template and schedules with the various sectors
• Negotiation of the performance indicators in the schedules by the individual LHIN-HSP
• Multi year

Principles
• Mutuality• Openness, transparency • Flexibility• Realism, pragmatism, achievable• Streamlined, simplified• Conformity with LHSIA, MOHLTC-LHIN MOU, MLAA• Compatibility with the spirit and intent of the LHIN and
HSPs role in the health care change agenda• Conformity of style and terminology with all sector SAAs

The Consultation Structure
Operating Plan Guidelines Team
Indicator Reference Team
CSS MH &A
CCAC
CHC
Communication Team
Steering Committee
LHIN Leadership (Chairs and CEOs)

Roles and Responsibilities

Steering Committee• Accountable to the LHIN Leadership (Chairs and
CEOs)• Responsible for:
• providing oversight for the consultation process • making final recommendations regarding changes to
the template documents and schedules• Providing support as necessary to the Sector specific
consultation teams• Providing oversight for the communication and
education plan for LHINs• Providing oversight of the LHIN final approval process

Sector Teams
• One team for each sector• Provide input to the Steering Committee• Responsible for:
• Carrying out the sector specific consultation process
• Suggesting items to be included in the communiques
• making recommendations regarding changes (if any) to the template documents and schedules

Multi Sectoral Service Accountability Agreement (M-SAA) – Overview

M-SAA Development Principles
M-SAAs:• Reflect the principles in the Ministry –LHIN
Accountability Agreement (MLAA) • Support MLAA direction to strengthen accountability for
results.• Clearly articulate expectations of both parties • Ensure consistency to support alignment with provincial
strategic directions, streamline processes, minimize burden and provide clarity and equity for HSPs and LHINs
• Promote fairness and equitable treatment of health service providers
• Reflect a clear line of accountability for health service providers and “a new world of accountability” in the relationship between LHINs and their HSPs

M-SAAIndex to Agreement• Article 1 Definitions & Interpretation• Article 2 Term & Nature of the Agreement• Article 3 Provision of Services • Article 4 Funding• Article 5 Repayment and Recovery of Funding• Article 6 Planning & Integration• Article 7 Performance• Article 8 Reporting, Accounting and Review• Article 9 Acknowledgement of LHIN Support• Article 10 Representations, Warranties and Covenants• Article 11 Limitation of Liability, Indemnity & Insurance
Article 12 Termination • Article 13 Notice• Article 14 Additional provisions• Article 15 Entire Agreement

M-SAA• SCHEDULE A - DESCRIPTION OF SERVICES
• SCHEDULE B- SERVICE PLAN
• SCHEDULE C - REPORTS
• SCHEDULE D – DIRECTIVES, GUIDELINES, POLICIES
• SCHEDULE E – PERFORMANCE
• SCHEDULE F - TEMPLATE FOR PROJECT FUNDING

Performance Indicators

SAA Indicator Process• Inventory of measures generated from existing agreements and
scorecards• Oct. 2007 Framework for Indicators selected• 2 day working meeting LHINs and MOHLTC staff with sector
and measurement expertise• Objectives:
– select indicators that apply to all sectors– Include program and/or sector specifics indicators (i.e.,
sectors will have unique volumes and outcomes) as required• Results:
– Performance (able to measure and est. targets now), Monitoring (keep ‘an eye on’ targets not relevant), and Development Indicators (need definition, development)
– Core measures (all LHINs and sectors)– Sector and / or LHIN-specific measures

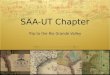
Indicator Framework
Financial Fiscal Health
High QualityHealth
Services
SystemPerspective
OrganizationalCapacity
Patient/ClientPerspective

Measurement FrameworksMLAA indicator
domainsSustainability Access Quality Integration
Productivity and fiscal health Health Resources
Efficiency Sound business practices
HHRCapital infrastructure Accessible Safety Continuity
Effective / evidence-
based Patient centred IT capacity Innovation
Efficient
Appropriately resourced (capacity) Accessible Appropriate
Integrated Continuity
Effective = evidence-
based, outcome focused Patient centred
Recommended
Framework for
SAAs
Fiscal / financial health / results
Organizational capacity
Patient Centered
HAA Financial Health
Organizational Health Patient Access and
System Coordination and Integration Outcomes
Mental Health
Strategy Map Sustainability
System capacity and organization Utilization Equity
Evidence Use Outcomes
CHC SAAsOrganizational
HealthService integration Client Outcomes
CHC strategy mapFinancial (resourced,
efficient)Sustainable /
equitableHealth status and
outcomes Learning and GrowthSystem performance
High Quality Health Services
Strengthening community capacity
MOHLTC starting
point domains
Provision of high quality health services Evidence and
innovation
Innovation
LHI N Blueprint
Core I ndicator
Domains

Indicators—All SectorsCORE PERFORMANCEFinancial Fiscal Health
– Total margin– Current ratio– Cost per unit service– Cost per individual served
Organizational Health– Variance budget and forecast $ – Variance budget and forecast units of
service – % spent on direct care
HQHS– service activity / volumes (sector specific)
System Measures– ALC (CCAC; CSSl)– ED Visits (MH and A; CHC; CSS)– ACSC (MH and A; CHC)– LTC waits (CCAC; CSS)
TO BE ASSESSED FOR MEASURABILITY / To Develop
Organizational Health– Vacancy rate– Turnover rate
HQHS– Wait time from referral to assessment– Wait times from assessment to service
initiation– High risk occurrences– Client achieves goals on discharge /
readmissionsPatient Perspective
– Patient experience

Sector Specific MeasuresCommunity Support Services
• Units served and individuals served by service type or functional centre e.g., number of meals served and number individuals served
• Currently no provincial approach to collecting ‘clinical’ data for sector or programs with the exception of the PFA and OHRS information collected on service volumes

Review Criteria used to Evaluate Indicators
Indicator Criteria
Definition Description
Measures one or more of the dimensions in the SAA framework
LHINs would track the provider’s performance on the indicator and expect a performance report or performance improvement plan if the provider was over or under performing on a measure Important to
achieving HSP accountability
Indicator is a meaningful measure of LHIN priorities, system priority or health service providers’ mandate
e.g., CSS agency provides transportation services; CHCs provide primary care in one on one and group settings and they are also about engaging community and community capacity building; supports chronic disease management strategy

Review Criteria Indicator Criteria
Definition Description
Feasible
Data required for the indicator are readily available for the areas and time periods required; there are no unreasonable obstacles or constraints on access and the information can be used without restrictions
III. Currently reported in Ontario at HSP level
Indicator currently available, defined and reported at the HSP level (e.g., HIT indicators) Note where the data are not presently available for all sectors.
II. Currently reported in Ontario
Indicator used in Ontario now; could be adapted for use at the HSP level (with some specifics still to be determined: i.e., are numbers large enough for reporting; are data reliable, valid and meaningful at HSP level) Note where the data are not presently available for all sectors.
I. Existing indicator Data are available at HSP level and indicator is defined, could be calculated for use and can feasibly be reported in the near future (with some specifics still to be determined: numbers large enough for reporting; reliable, valid and meaningful at HSP level) Note where the data are not presently available for all sectors.
Data available / indicator would require development
Data is currently collected by health service providers; Indicator could be developed from existing data / no major data quality issues or data quality unknown
Measurable
Not reportable Indicators not currently defined, data not reported consistently across the province e.g., patient satisfaction measures

Review Criteria
Indicator Criteria Definition Description
Locus of Control Within providers control
Understandable Indicator can be readily understood and interpreted Actionability
Actionable Indicator provides information that can be acted upon by health service providers (clinicians and/or policy makers where relevant)
Linkable Cascading Would indicator roll up to LHIN / system level be meaningful?
Meets technical requirement:
Valid at HSP level
Consensus by users and experts that this measure is related to the dimension it is supposed to assess (face validity); covers the whole dimension of what it is supposed to assess (content validity); related to other indicators measuring the same dimension (construct validity); and has predictive power (criterion validity)
Reliable (potential) Consistent data collection and quality supported
Clear direction for change
Change in the value of an indicator in a single direction is interpretable as being favorable or unfavorable.

Consultation Questions

Consultation Questions re Template• Is it missing anything? If so, is the missing element something that is
common to all HSPs or is it something that is common to a particular sector of HSPs.
• Do you understand all the provisions? Do they make sense?• Are all the provisions necessary? Are any redundant? Not needed in
an SAA?For example, 3.1(e) may not be appropriate for a CCAC.
• Does the order in which they are set out in the agreement flow logically? make sense?
• Will these schedules apply to all this sector?• Is there something that is particular to this sector that should be in the
schedules?• Do any of this sector require more schedules than the ones that have
been identified in this template?• •

Consultation Questions re Indicators• How does the framework align with the sector’s strategy maps,
scorecards and frameworks?• Will individual health service providers be able to link their internal
quality monitoring and reporting to their accountability as captured through this framework and the measures?
• Is the categorization of the existing measures as core performance (can measure now) , monitoring and developmental (need some or a great deal of work) clear?
• How many measures should we strive for as core performance measures?
• Are the dimensions of performance all adequately balanced in the proposed framework and with the measures we currently have?
• • • •

Time Lines and Next Steps

Timelines and Next Steps
•Sector specific consultations (June/July)•Recommendations from sector Teams to Steering Committee (July 31)•Operating Guidelines to Steering Committee (July 31)•Finalize Template and Schedules (July/August)•Operating Plan Guidelines Released to Sectors (Late August)•LHIN Board approval on Template and Schedules (Sept)• HSP Operating Plans due to LHINs (to be confirmed)• LHIN Negotiations with HSPs (Nov – March)

Discussion