Embed Size (px)
Citation preview
UNIVERSITY OF TABUKFACULTY OF APPLIED MEDICAL SCIENCE
NURSING DEPARTMENT
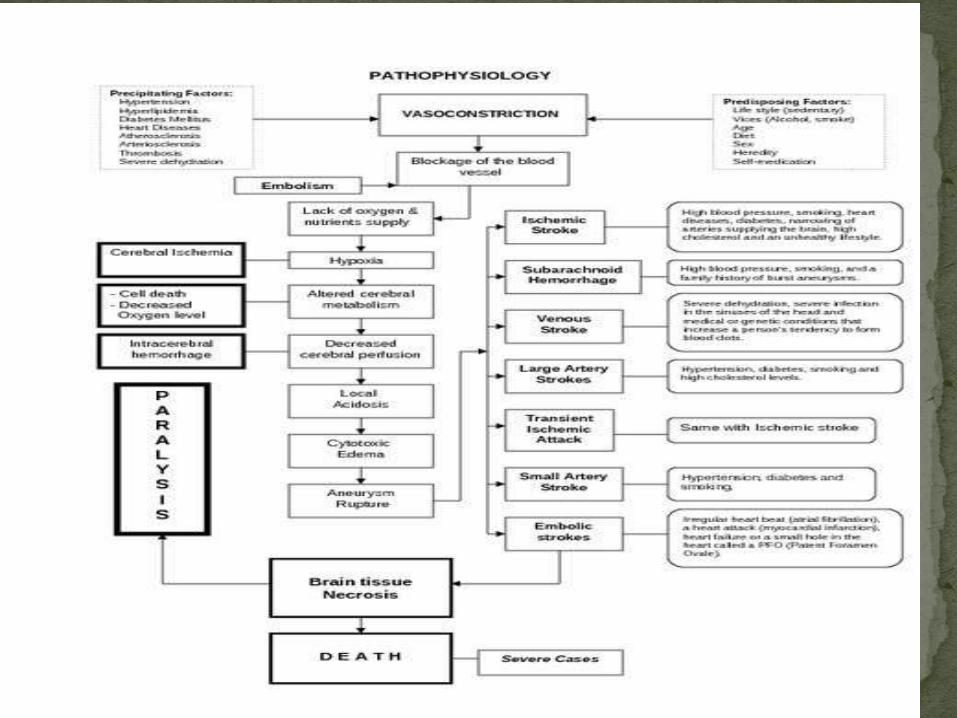
Stroke occurs when the supply of blood to the brain is either interrupted or reduced. When this happens, the brain does not get enough oxygen or nutrients which causes brain cells to die.
There are three main kinds of stroke; ischemic, hemorrhagic and TIA.
Causes of stroke vary, however can be classified strokes to infarcts result clots or emboli or hemorrhagic infarcts.
About 80-87% of strokes are caused by blockage of an artery in the brain due to clots or emboli, and infestations include most cases of hemorrhagic strokes remaining, and with a small number of cases that occur as a result of subarachnoid hemorrhage from expansions of vascular “aneurysmalsubarachnoid hemorrhage.”
About 20-40% of cases of ischemic infestations occur with hemorrhagic transformation within a week from the beginning of their occurrence.
Differentiate between different types of strokes is an essential part of the evaluation of cases where strokes that subsequent treatment is different in each case, to a large extent.
In the US, approximately 40% of stroke deaths are in males, with 60% in females. According to the American Heart Association (AHA), in 2006, the stroke death rates per 100,00 population could be split into specific social groups at 41.7% for white males, 41.1% for white females, 67.7% for black males and 57.0% for black females.3
Stroke is also more likely to affect people if they are overweight, aged 55 or older, have a personal or family history of stroke, do not exercise much, drink heavily or use illicit drugs.5
Prevalence of strokes in the world vary from one country to another. For example, there is an increase incidence of hemorrhagic strokes among Chinese and Japanese, and the prevalence of acute strokes generally declined over recent decades in the world.
Every year happens about 795 000 new cases of stroke or recurrent stroke in the United States, of whom about 610,000 state for the first time, and about 185,000 frequent case.
About 87% of cases in the United States are ischemic and 10% of the cases as a result of bleeding inside the brain, and 3% are due to subarachnoid hemorrhage.
Prevalence of strokes associated with the age and sex of the patient, race and socioeconomic status, for example, be injuries strokes Aljobeh among black people in the United States three times the injuries to these strokes among white people.
The different forms of stroke have different specific causes.
Ischemic strokes Ischemic strokes are the most common form of stroke, with
around 85% of strokes being of this type. They are caused by the arteries that connect to the brain becoming blocked or narrowed, resulting in ischemia - severely reduced blood flow.
These blockages are often caused by blood clots, which can form either in the arteries connecting to the brain, or further away before being swept through the bloodstream and into narrower arteries within the brain. Clots can be caused by fatty deposits within the arteries called plaque.
Hemorrhagic strokes Hemorrhagic strokes are caused by arteries in the
brain either leaking blood or bursting open. The hemorrhaged blood puts pressure on brain cells and damages them. Blood vessels can burst or spill blood in the middle of the brain or near the surface of the brain, sending blood into the space between the brain and the skull.
The ruptures can be caused by conditions such as hypertension, trauma, blood-thinning medications and aneurysms (weaknesses in blood vessel walls).
Transient ischemic attack (TIA) TIAs are different from the aforementioned kinds of
stroke because the flow of blood to the brain is only disrupted temporarily for a short time. They are similar to ischemic strokes in that they are often caused by blood clots or other debris.
TIAs should be regarded as medical emergencies just like the other kinds of stroke, even if the blockage of the artery is temporary. They serve as warning signs for future strokes and indicate that there is a partially blocked artery or clot source in the heart.
According to the Centers for Disease Control and Prevention (CDC), over a third of people who experience a TIA go on to have a major stroke within a year if they have not received any treatment. Between 10-15% will have a major stroke within 3 months.
Strokes occur quickly, and as such their symptoms often appear suddenly without warning. The main symptoms are as follows:
Confusion, including trouble with speaking and understanding
Headache, possibly with altered consciousness or vomiting
Numbness of the face, arm or leg, particularly on one side of the body
Trouble with seeing, in one or both eyes
Trouble with walking, including dizziness and lack of co-ordination.
Strokes can lead to long-term problems. Depending on how quickly it is diagnosed and treated, the patient can experience temporary or permanent disabilities in the aftermath of a stroke. In addition to the problems listed above continuing, patients may also experience the following:
Bladder or bowel control problems
Depression
Pain in the hands and feet that gets worse with movement and temperature changes
Paralysis or weakness on one or both sides of the body
Trouble controlling or expressing emotions.
Strokes occur quickly, so that often a stroke diagnosis will have to be made before an individual can be seen by a doctor. The acronym FAST is a way to remember the signs of stroke, and can help toward identifying the onset of stroke in someone:
Face drooping: if the person tries to smile does one side of the face droop?
Arm weakness: if the person tries to raise both their arms does one arm drift downward?
Speech difficulty: if the person tries to repeat a simple phrase is their speech slurred or strange?
Time to call 911: if any of these signs are observed, contact the emergency services.
It is important that strokes are diagnosed as quickly as possible. The quicker that treatment can be administered, the less damage that will be done to the brain. In order for a stroke patient to get the best diagnosis and treatment possible, they will need to be treated at a hospital within 3 hours of their symptoms first appearing.
Both ischemic strokes and hemorrhagic strokes require different kinds of treatment. Unfortunately, it is only possible to be sure of what type of stroke someone has had by giving them a brain scan in a hospital environment.
Physical examination: a doctor will ask about the patient's symptoms and medical history. They may check blood pressure, listen to the carotid arteries in the neck and examine the blood vessels at the back of the eyes, all to check for indications of clotting
Blood tests: a doctor may perform blood tests in order to find out how quickly the patient's blood clots, what the levels of chemicals within it are like and whether or not the patient has an infection
CT scan: a series of X-rays that can show hemorrhages, strokes, tumors and other conditions within the brain
MRI scan: radio waves and magnets create an image of the brain to detect damaged brain tissue
CT scans of the brain are one of the only ways to diagnose what type of stroke a person has had
MRI scan: radio waves and magnets create an image of the brain to detect damaged brain tissue
Carotid ultrasound: an ultrasound scan to check the blood flow of the carotid arteries and to see if there is any plaque present
Cerebral angiogram: dyes are injected into the brain's blood vessels to make them visible under X-ray, in order to give a detailed view of the brain and neck arteries
Echocardiogram: a detailed image of the heart is created to check for any sources of clots that could have traveled to the brain to cause a stroke.
As the two main different kinds of stroke, ischemic and hemorrhagic, are caused by different factors, both require different forms of treatment. It is particularly important that the type of stroke is diagnosed quickly, not just to reduce the damage done to the brain but because treatment for one kind of stroke may be harmful to someone who has had a different kind.
Ischemic stroke Ischemic strokes are caused by arteries being blocked
or narrowed and so treatment focuses on restoring an adequate flow of blood to the brain.
Treatment can begin with drugs to break down clots and prevent further ones from forming. Aspirin can be given, as can an injection of a tissue plasminogen activator (TPA). TPA is very effective at dissolving clots but needs to be injected within 4.5 hours of stroke symptoms manifesting themselves.
Surgeons are able to remove plaque and any other obstructions from the carotid artery through surgery.
Emergency procedures include administering TPA via catheter directly into an artery in the brain or using a catheter to physically remove the clot from its obstructive position. Recent studies have cast doubt as to the effectiveness of these methods, and so research is still ongoing as to how beneficial these procedures are.

Surgeons are able to remove plaque and any other obstructions from the carotid artery through surgery
There are other procedures that can be carried out to decrease the risk of future strokes or TIAs. A carotid endarterectomy involves a surgeon opening the carotid artery and removing any plaque that might be blocking it.
Alternatively, an angioplasty involves a surgeon inflating a small balloon in a narrowed artery via catheter and then inserting a stent (a mesh tube) into the opening in order to prevent the artery from narrowing again.
The best way to prevent a stroke is to address the underlying causes. This is best done by living healthily. Here is a list of simple measures that can be followed:
Avoid illicit drugs
Eat a diet rich in fruit and vegetables and low in cholesterol and saturated fat
Exercise regularly
Keep blood pressure under control
Keep diabetes under control
Maintain a healthy weight
Moderate alcohol consumption (or quit drinking)
Quit smoking
Treat obstructive sleep apnea (if present).
As well as these lifestyle changes, a health care provider can help to reduce the risk of future strokes through prescribing anti-coagulant and anti-platelet medication. In addition to this, the arterial surgery previously mentioned can also be used to lower the risk of repeat strokes.
anatomy
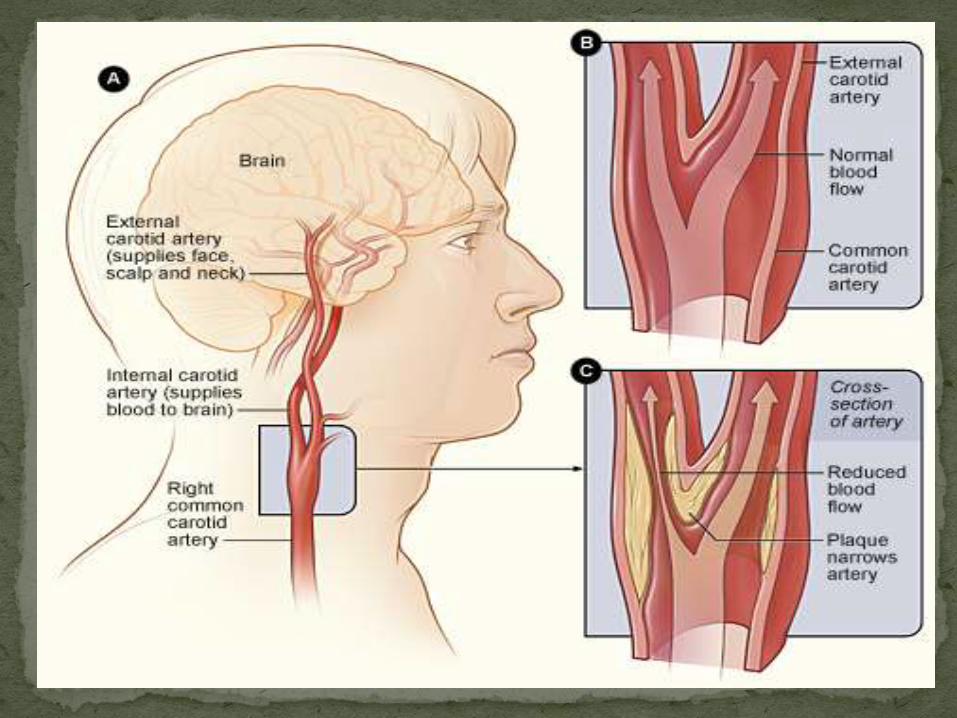
Controllable risk factors: High blood pressure (hypertension): Atherosclerosis: With this major risk factor for stroke,
fatty plaques that build up inside the artery walls will block or narrow the vessels, which can lead to stroke.
Heart disease High cholesterol Smoking or tobacco use Atrial fibrillation Diabetes Overweight or obesity Blood disorders Excessive alcohol Drugs: Certain medications, such as anticoagulants, can
raise stroke risk.
Uncontrollable risk factors:
Age.
Gender: Strokes are more common in men.
Race:African-Americans are much more likely to die from strokes than whites, partly because African-Americans have a higher risk of hypertension, diabetes, and obesity.
Family history.
Previous stroke or heart attack
Artery abnormalities
Fibromuscular dysplasia:With this medical disorder, some arteries develop improperly. Fibrous tissue grows in artery walls, making them narrower. As a result, blood flow through the arteries is reduced, which can lead to stroke.
Patent foramen ovale ( hole in the heart
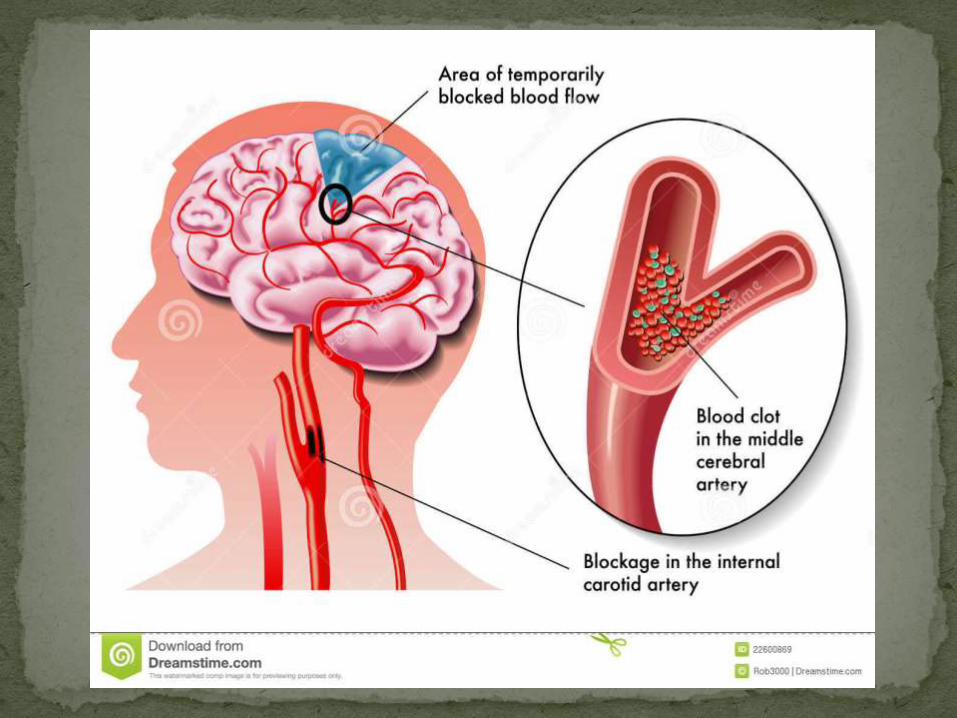
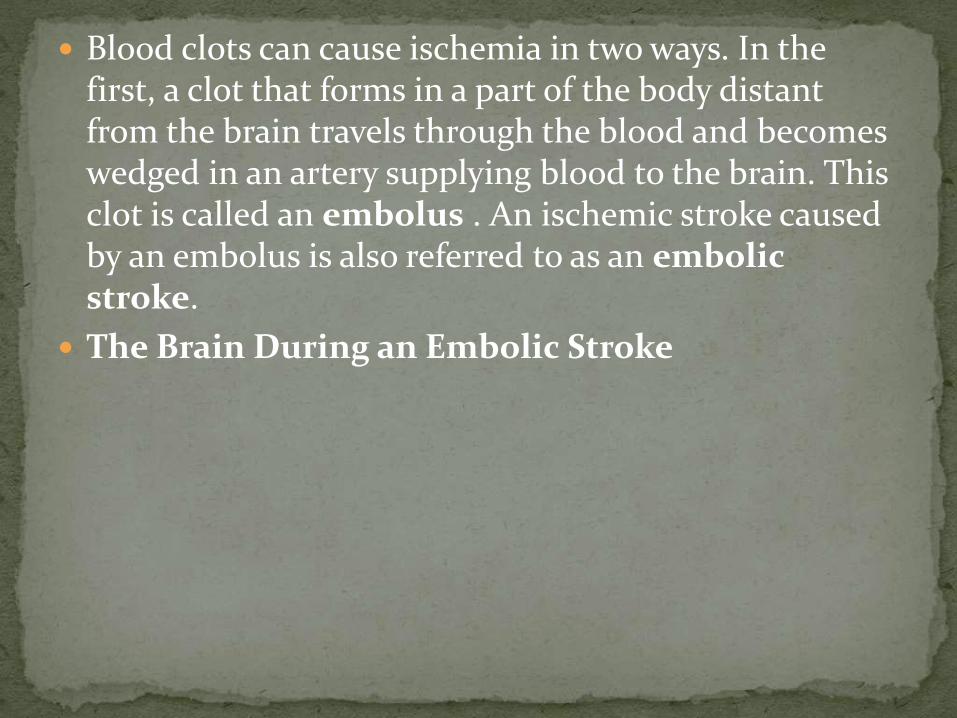
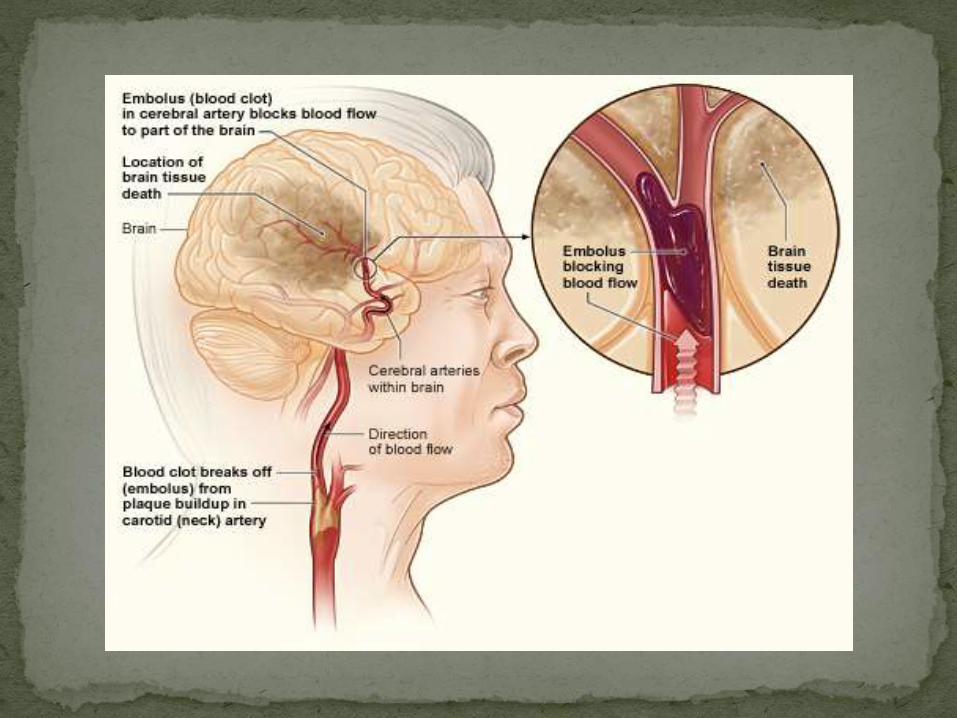
Blood clots can cause ischemia in two ways. In the first, a clot that forms in a part of the body distant from the brain travels through the blood and becomes wedged in an artery supplying blood to the brain. This clot is called an embolus . An ischemic stroke caused by an embolus is also referred to as an embolic stroke.
The Brain During an Embolic Stroke
The second kind of ischemic stroke, called a thrombotic stroke, is caused by thrombosis, the formation of a blood clot in one of the cerebral arteries that stays attached to the artery wall until it grows large enough to block blood flow .
Ischemic strokes can also be caused by stenosis, a narrowing of an artery due to the buildup of plaque and blood clots along the arterial wall.
Stenosis in a Section of an Artery
Demographic
Name: M.alshamryDate of birth: 3-2-1926Age:89 yearsGender: malemarital status : married
Admission Date: 03/03/2015Diagnosis:new stroke-DM –HPN-CVA-prostatic hypertrophyChief complaint:came through ER with complaint fall down in his home due to known case of cva with left hemiplegia
Family history :no family history
Medical history: Hypertension Diabetes mellitus
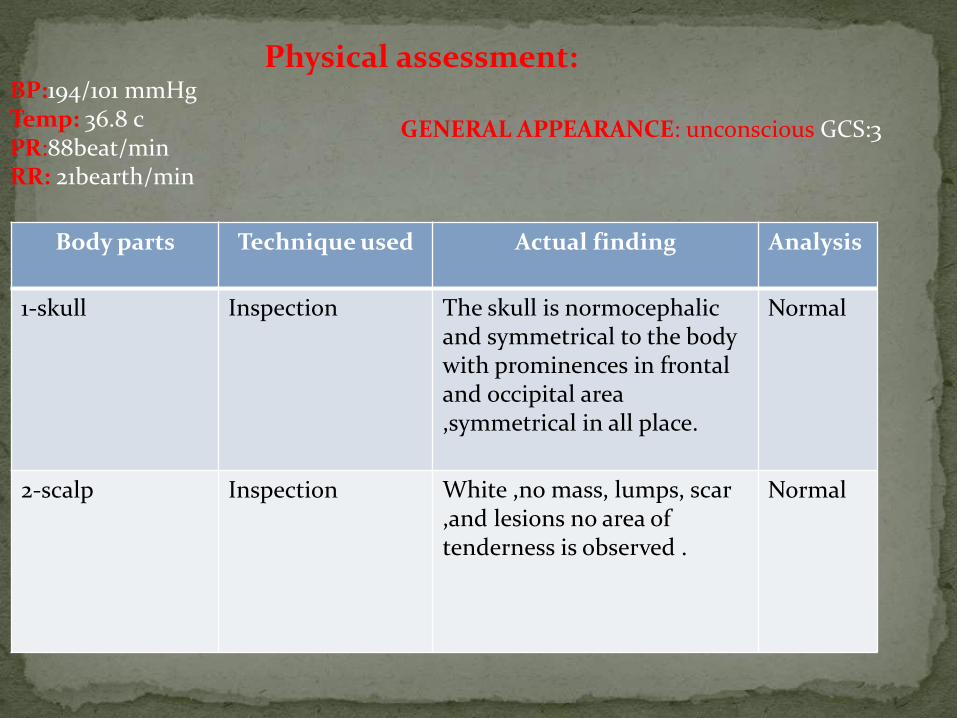
Physical assessment:BP:194/101 mmHg Temp: 36.8 cPR:88beat/minRR: 21bearth/min
AnalysisActual findingTechnique usedBody parts
Normal The skull is normocephalicand symmetrical to the body with prominences in frontal and occipital area ,symmetrical in all place.
Inspection1-skull
Normal White ,no mass, lumps, scar ,and lesions no area of tenderness is observed .
Inspection 2-scalp
GENERAL APPEARANCE: unconscious GCS:3
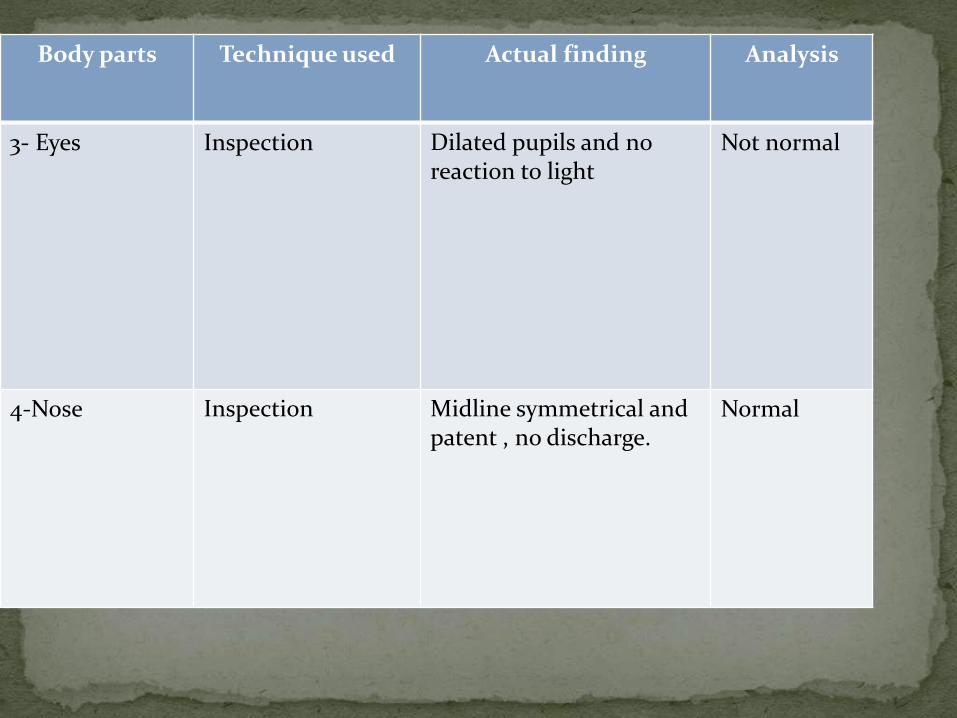
AnalysisActual findingTechnique usedBody parts
Not normalDilated pupils and no reaction to light
Inspection 3- Eyes
Normal Midline symmetrical and patent , no discharge.
Inspection 4-Nose
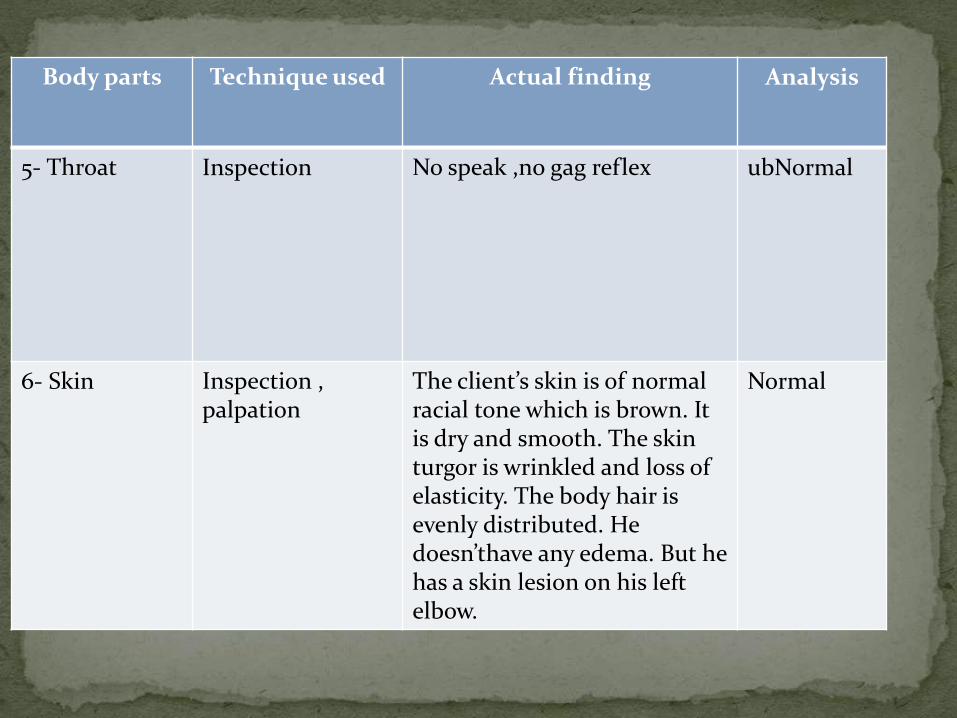
AnalysisActual findingTechnique usedBody parts
ubNormalNo speak ,no gag reflexInspection 5- Throat
Normal The client’s skin is of normal racial tone which is brown. It is dry and smooth. The skin turgor is wrinkled and loss of elasticity. The body hair is evenly distributed. He doesn’thave any edema. But he has a skin lesion on his left elbow.
Inspection ,palpation
6- Skin
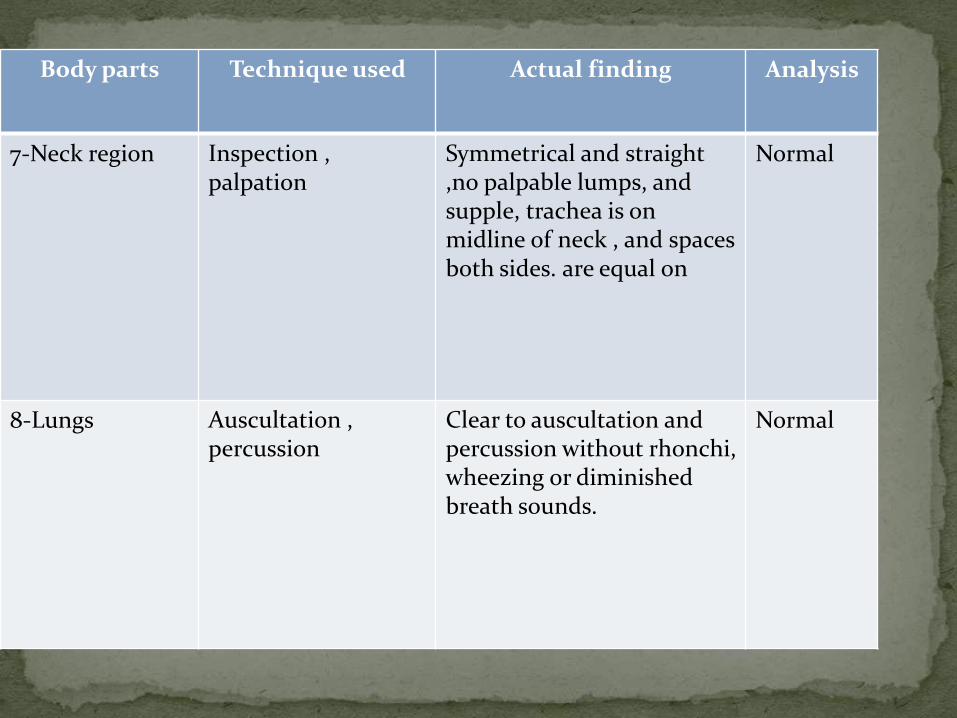
AnalysisActual findingTechnique usedBody parts
Normal Symmetrical and straight,no palpable lumps, and supple, trachea is on midline of neck , and spaces
are equal on both sides.
Inspection ,palpation
7-Neck region
NormalClear to auscultation and percussion without rhonchi, wheezing or diminished breath sounds.
Auscultation ,percussion
8-Lungs
AnalysisActual findingTechnique usedBody parts
Normal No tenderness,Masses,Nodules and discharge.
Inspection ,Palpation
10-Breast
AnalysisActual findingTechnique used
Body parts
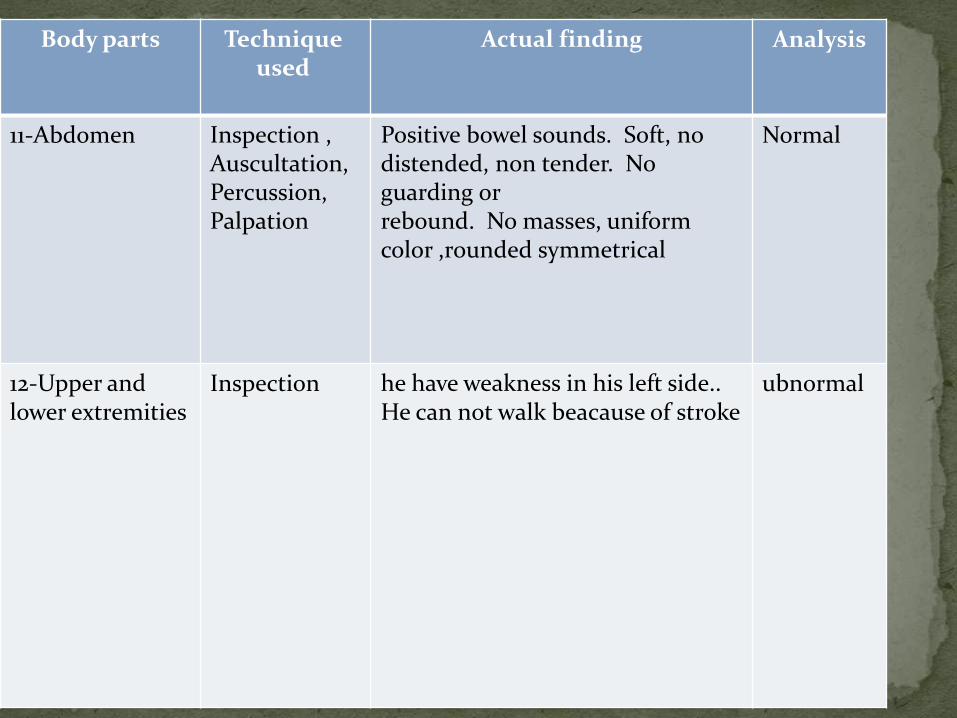
Normal Positive bowel sounds. Soft, no distended, non tender. No guarding or rebound. No masses, uniform color ,rounded symmetrical
Inspection ,Auscultation,Percussion,Palpation
11-Abdomen
ubnormalhe have weakness in his left side.. He can not walk beacause of stroke
Inspection 12-Upper and lower extremities
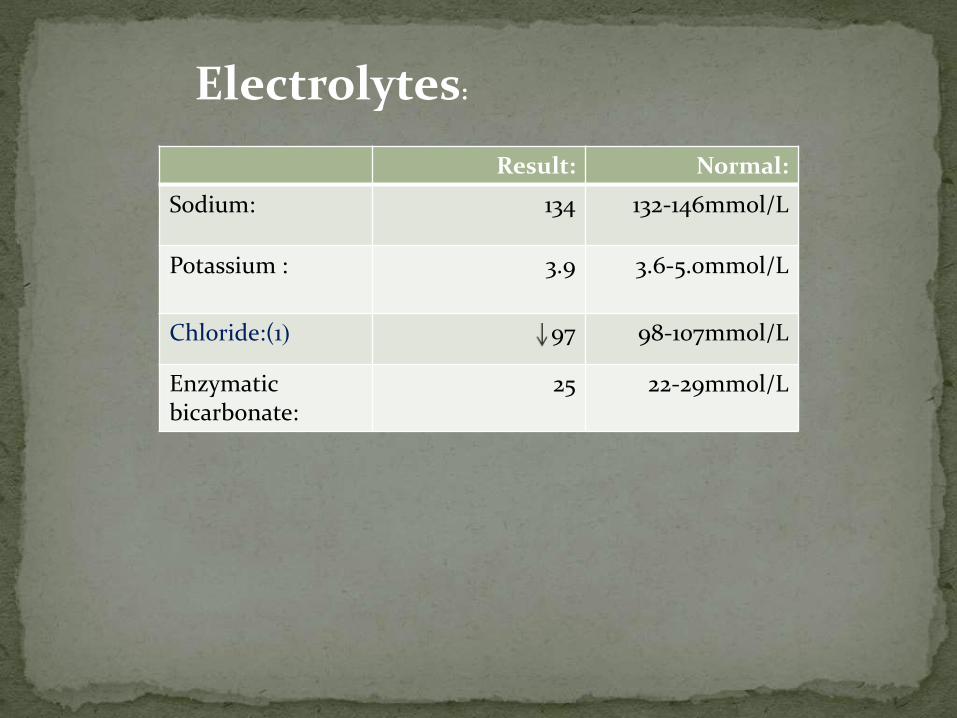
Electrolytes:
Normal:Result:
132-146mmol/L134Sodium:
3.6-5.0mmol/L3.9Potassium :
98-107mmol/L97(Chloride:(1
22-29mmol/L25Enzymaticbicarbonate:
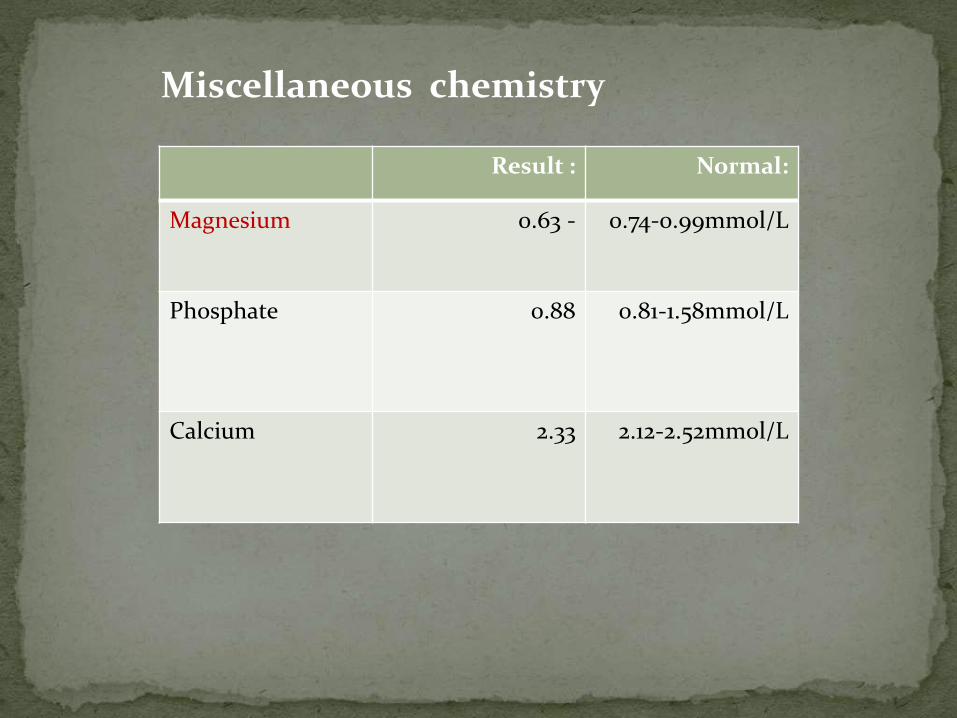
Miscellaneous chemistry
Normal:Result :
0.74-0.99mmol/L0.63 -Magnesium
0.81-1.58mmol/L0.88Phosphate
2.12-2.52mmol/L2.33Calcium

Hematology
Normal: Result:
4.0-11.0 10^3/Ml6.33WBC
3.8-4.8 10^6/Ml4.27RBC
12.0-16.0g/dl10.2 -Hemoglobin
41.0-50.0%29.4 -HCT
82.7-89.485.2MCV
31.5-34.5g/dl34.4MCHC
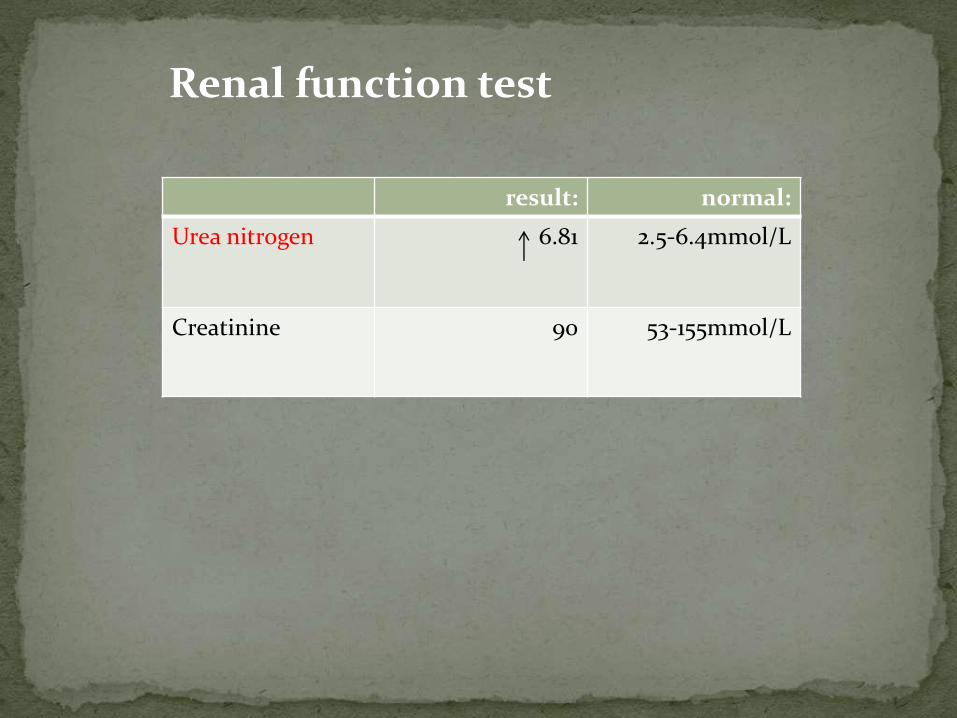
Renal function test
normal:result:
2.5-6.4mmol/L6.81Urea nitrogen
53-155mmol/L90Creatinine

Medical management
Critical treatment decisions focus on the The following need for airway management
Optimal blood pressure control
Identifying potential reperfusion therapies (eg, intravenous fibrinolysis with rt-PA or intra-arterial approach
Fibrinolytic therapy
Antiplatelet agents [4, 5]
Mechanical thrombectomy
Reduce fever
Correct hypotension/significant hypertension
Correct hypoxia
Correct hypoglycemia
Manage cardiac arrhythmias
Manage myocardial ischemia
Supplemental oxygen as required
Antiplatelet therapy
Glycemic control
Optimal blood pressure control
Prevention of hyperthermia
Oxygen therapy; give supplemental oxygen only if oxygen saturation drops below 95%.
Blood sugar control; maintain blood glucose concentration between 4 and 11 mmol/L. Provide optimal insulin therapy with intravenous insulin and glucose, for people with diabetes.
Hypertensive encephalopathy.
Hypertensive nephropathy.
Hypertensive cardiac failure/myocardial infarction.
Aortic dissection.
Pre-eclampsia/eclampsia.
Intracerebral haemorrhage with systolic blood pressure >200 mm Hg.
People with acute stroke should have their swallowing screened before being given any oral food, fluid or medication.[7] Also screen for malnutrition.
Aspirin (300 mg) should be given as soon as possible after the onset of stroke symptoms once a diagnosis of primary haemorrhage has been excluded.[8]Antiplatelet therapy should then be continued indefinitely. Therapy should be delayed for 24 hours following thrombolysis. Clopidogrel 75mg daily is recommended.[7]
Thrombolytic treatment: see separate article Thrombolytic Treatment of Acute Ischaemic Stroke. Unless there are contra-indications, thrombolytic treatment appears to be effective in improving prognosis after an acute stroke.[9] Treatment withalteplase should only be given provided that:
It is administered within four and a half hours of onset of stroke Anticoagulants should not be started until brain imaging has excluded haemorrhage. In patients with acute ischaemic strokesymptoms(unless as part of a clinical trial).
The type of surgery recommended by your physician depends on various
factors. Some surgical methodologies include
CaroEndarterectomy tid
This surgery involves removing plaque from the carotid artery that leads to the blood flow within the brain.
This may reduce the risk of ischemic stroke
Microsurgical Techniques: Brain Bypass Surgery
This microsurgery creates a new path for blood to flow through the brain, particularly in areas that have been depleted of blood.
Another vessel usually is grafted to the cerebral artery to create this new path.
Microsurgical techniques allow Emory's experienced neurosurgeons to perform with optimal precision, resulting in less risk and better outcomes for the patient.
Critical treatment decisions focus on the The following need for airway management
Optimal blood pressure control
Identifying potential reperfusion therapies (eg, intravenous fibrinolysis with rt-PA or intra-arterial approach
Endovascular Thrombolysis
In this procedure, a neuro-interventionist threads a microcatheter from an artery in the groin to a blocked artery in the brain.
Clot-busting medications are injected into the artery to dissolve the clot and restore blood flow to the brain faster than many other medications.
Cerebral Angioplasty and Stenting
This procedure helps widen a blocked artery.
A catheter with a balloon at the end is inserted into the obstructed artery and the balloon is inflated, pushing the plaque against the walls.
A stent, or a mesh steel brace, then is inserted to keep fatty buildup from clogging the vessel.
Endovascular Procedures (Interventional Neuroradiology)
Interventional neuroradiological procedures are a less-invasive means of treating neurovascular disorders.
They use very small catheters, called microcatheters, to treat problems inside blood vessels.
The microcatheter is inserted into the vessels through a tiny puncture in the groin, where an interventional neuroradiologist can reach almost any vessel in the brain or spinal cord.
These endovascular approaches can be used to open narrowed or blocked arteries, dissolve clots in brain arteries, repair certain aneurysms, and close abnormal blood vessels that are at risk of bleeding.
These methods often avoid the need for more invasive surgery
ECG
X-RayCardiac EnzymeProceduresCVPLINE
CHEST DRAIN N/G TUBE URINE CATH CT BRAIN
CAROTIO DOPPLER CREQNESTE
DOSAGE/ ROUTE/ FREQUENCYCLASSIFICATION/ MECHANISM OF
ACTION
DRUG NAME
80 mgIV
CLASSIFICATION
Loop diuretic
MECHANISM OF ACTION
Furosemide inhibits reabsorption of Na and
chloride mainly in the medullary portion of
the ascending Loop of Henle. Excretion of
potassium and ammonia is also increased
while uric acid excretion is reduced. It
increases plasma-renin levels and secondary
hyperaldosteronism may result. Furosemide
reduces BP in hypertensives as well as in
normotensives. It also reduces pulmonary
oedema
GENERIC NAME:
furosemide
BRAND NAME:
Lasix
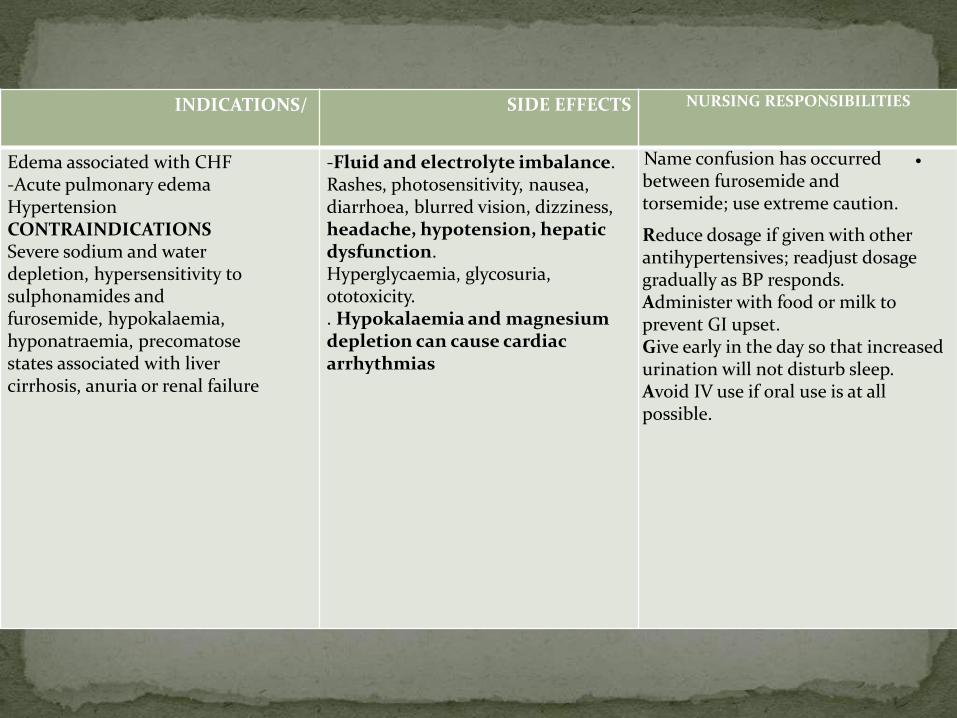
NURSING RESPONSIBILITIESSIDE EFFECTSINDICATIONS/
Name confusion has occurred between furosemide and torsemide; use extreme caution.
Reduce dosage if given with other antihypertensives; readjust dosage gradually as BP responds.Administer with food or milk to prevent GI upset.Give early in the day so that increased urination will not disturb sleep.Avoid IV use if oral use is at all possible.
-Fluid and electrolyte imbalance.Rashes, photosensitivity, nausea, diarrhoea, blurred vision, dizziness, headache, hypotension, hepatic dysfunction.Hyperglycaemia, glycosuria, ototoxicity.. Hypokalaemia and magnesium depletion can cause cardiac arrhythmias
Edema associated with CHF-Acute pulmonary edemaHypertensionCONTRAINDICATIONSSevere sodium and water depletion, hypersensitivity to sulphonamides and furosemide, hypokalaemia, hyponatraemia, precomatosestates associated with liver cirrhosis, anuria or renal failure
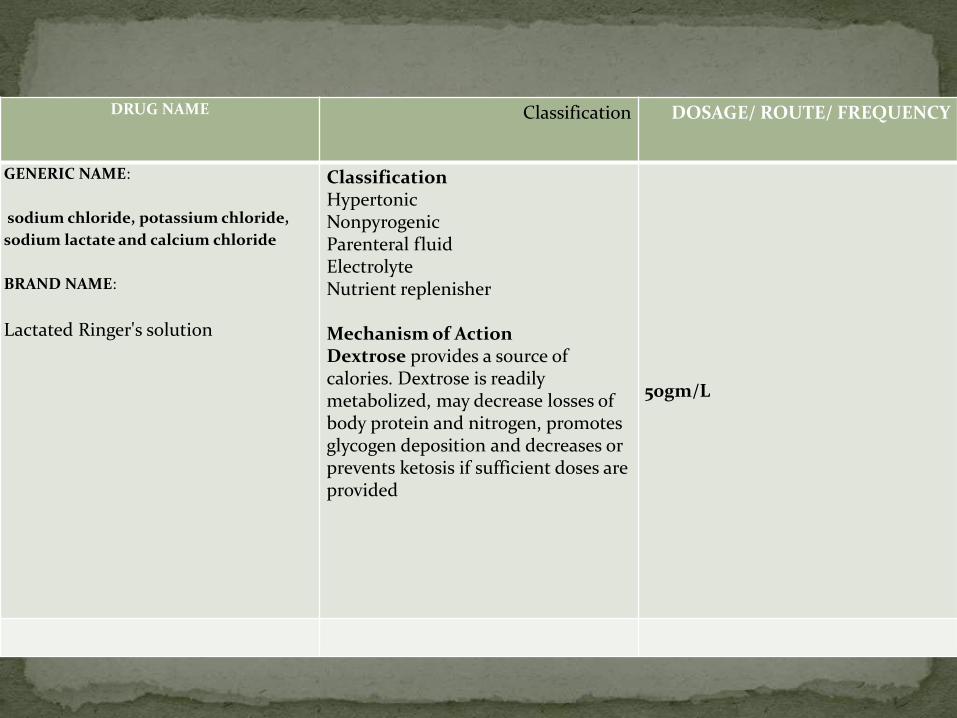
DOSAGE/ ROUTE/ FREQUENCYClassificationDRUG NAME
50gm/L
ClassificationHypertonicNonpyrogenicParenteral fluidElectrolyteNutrient replenisher
Mechanism of ActionDextrose provides a source of calories. Dextrose is readily metabolized, may decrease losses of body protein and nitrogen, promotes glycogen deposition and decreases or prevents ketosis if sufficient doses are provided
GENERIC NAME:
sodium chloride, potassium chloride,
sodium lactate and calcium chloride
BRAND NAME:
Lactated Ringer's solution
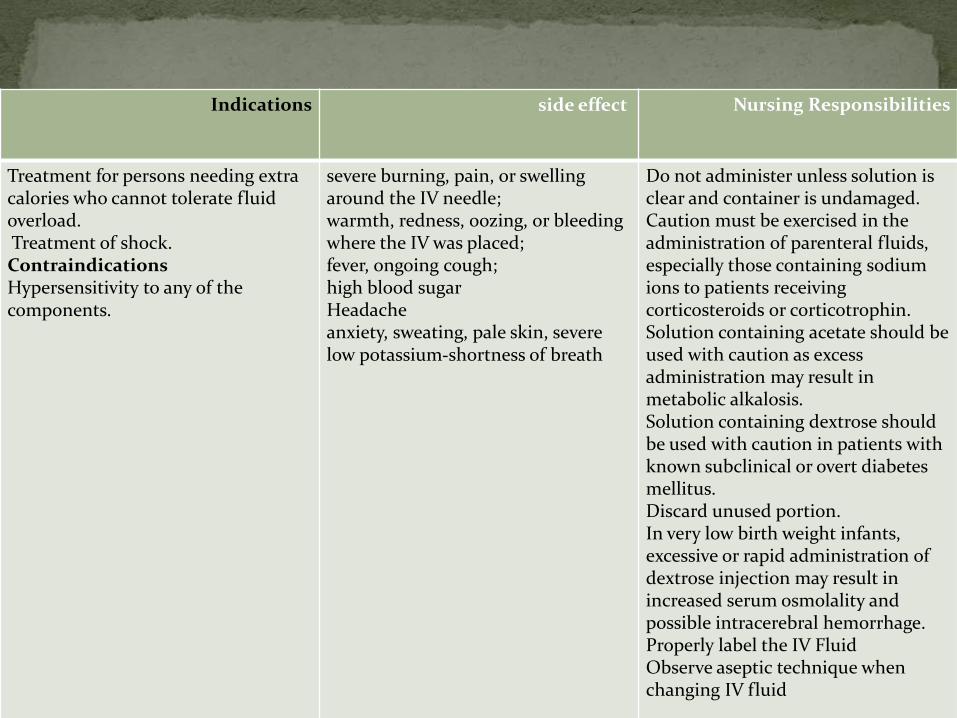
Nursing Responsibilitiesside effectIndications
Do not administer unless solution is clear and container is undamaged.Caution must be exercised in the administration of parenteral fluids, especially those containing sodium ions to patients receiving corticosteroids or corticotrophin.Solution containing acetate should be used with caution as excess administration may result in metabolic alkalosis.Solution containing dextrose should be used with caution in patients with known subclinical or overt diabetes mellitus.Discard unused portion.In very low birth weight infants, excessive or rapid administration of dextrose injection may result in increased serum osmolality and possible intracerebral hemorrhage.Properly label the IV FluidObserve aseptic technique when changing IV fluid
severe burning, pain, or swelling around the IV needle;warmth, redness, oozing, or bleeding where the IV was placed;fever, ongoing cough;high blood sugarHeadacheanxiety, sweating, pale skin, severe
shortness of breath-low potassium
Treatment for persons needing extra calories who cannot tolerate fluid overload.Treatment of shock.ContraindicationsHypersensitivity to any of the components.
Nursing care plan
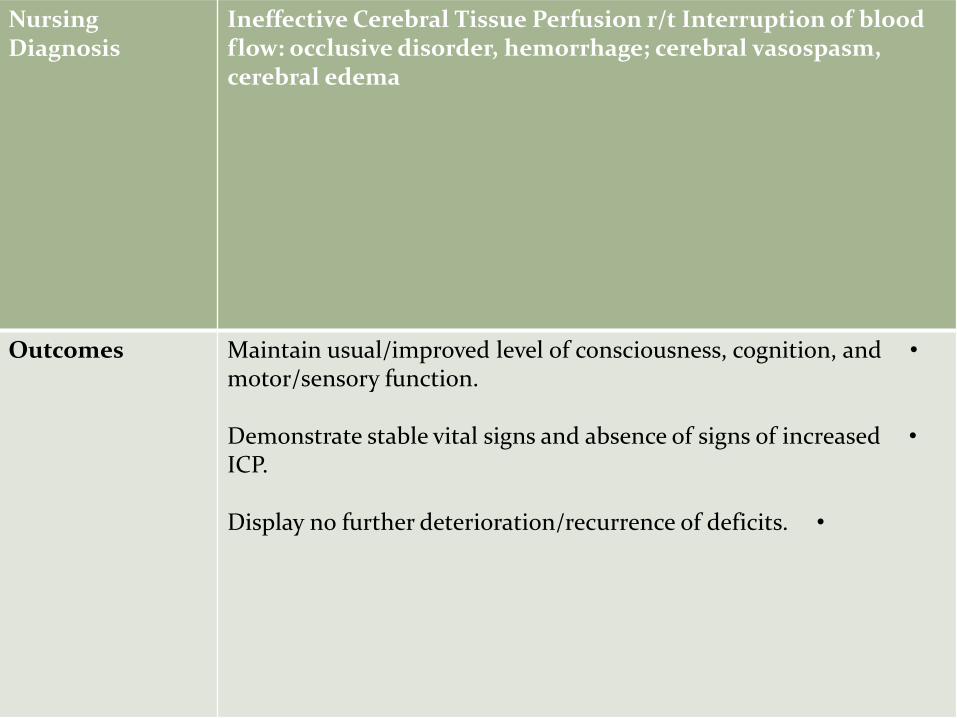
Ineffective Cerebral Tissue Perfusion r/t Interruption of blood flow: occlusive disorder, hemorrhage; cerebral vasospasm, cerebral edema
Nursing Diagnosis
•Maintain usual/improved level of consciousness, cognition, and motor/sensory function.
•Demonstrate stable vital signs and absence of signs of increased ICP.
•Display no further deterioration/recurrence of deficits.
Outcomes
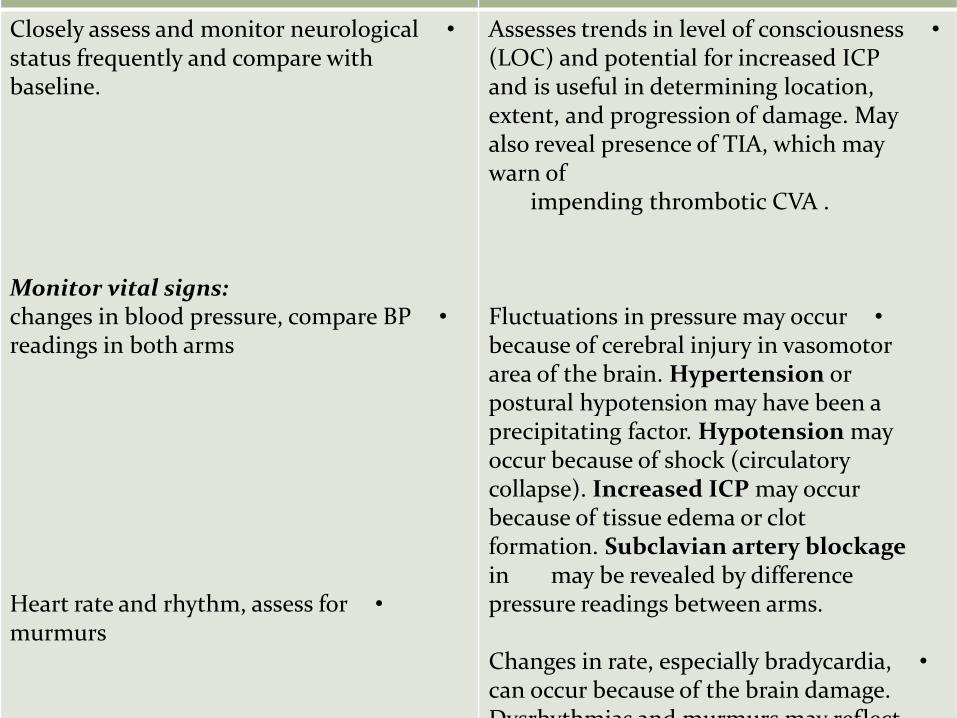
RationaleNursing Interventions
•Assesses trends in level of consciousness (LOC) and potential for increased ICP and is useful in determining location, extent, and progression of damage. May also reveal presence of TIA, which may warn of
impending thrombotic CVA .
•Fluctuations in pressure may occur because of cerebral injury in vasomotor area of the brain. Hypertension or postural hypotension may have been a precipitating factor. Hypotension may occur because of shock (circulatory collapse). Increased ICP may occur because of tissue edema or clot formation. Subclavian artery blockage
may be revealed by difference in pressure readings between arms.
•Changes in rate, especially bradycardia, can occur because of the brain damage. Dysrhythmias and murmurs may reflect
•Closely assess and monitor neurological status frequently and compare with baseline.
Monitor vital signs:•changes in blood pressure, compare BP
readings in both arms
•Heart rate and rhythm, assess for murmurs
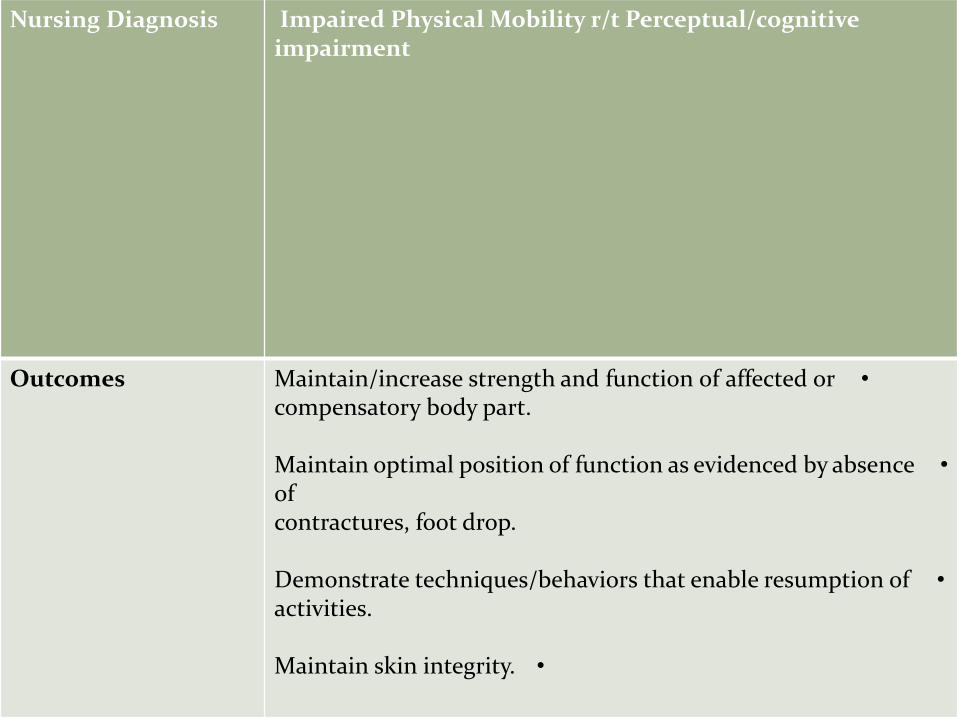
Impaired Physical Mobility r/t Perceptual/cognitive impairment
Nursing Diagnosis
•Maintain/increase strength and function of affected or compensatory body part.
•Maintain optimal position of function as evidenced by absence of contractures, foot drop.
•Demonstrate techniques/behaviors that enable resumption of activities.
•Maintain skin integrity.
Outcomes
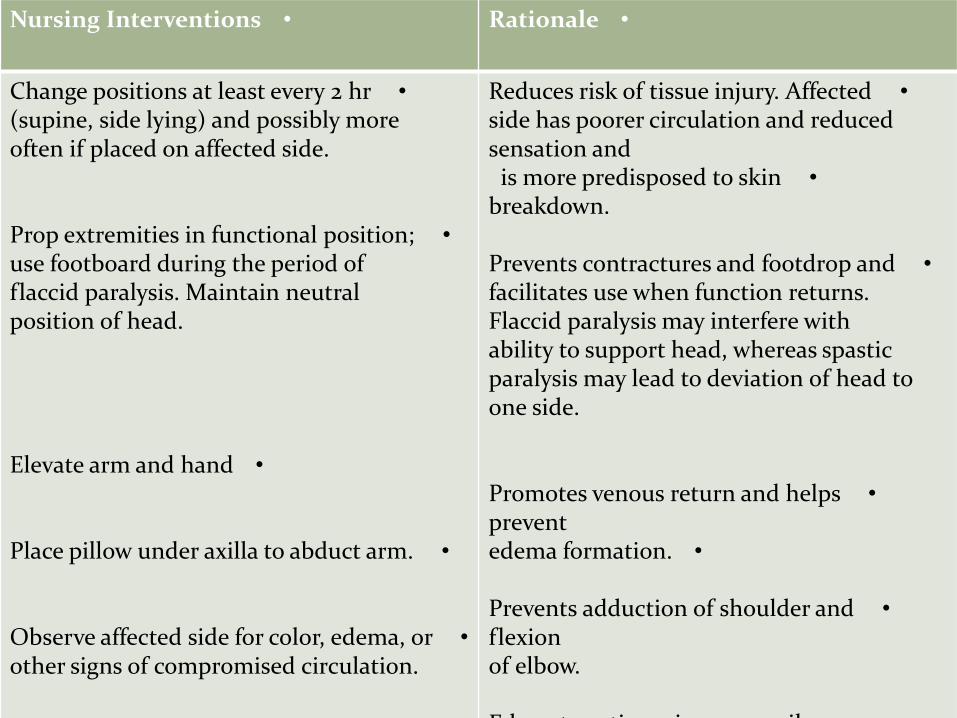
•Rationale•Nursing Interventions
•Reduces risk of tissue injury. Affected side has poorer circulation and reduced sensation and
•is more predisposed to skin breakdown.
•Prevents contractures and footdrop and facilitates use when function returns. Flaccid paralysis may interfere with ability to support head, whereas spastic paralysis may lead to deviation of head to one side.
•Promotes venous return and helps prevent
•edema formation.
•Prevents adduction of shoulder and flexion of elbow.
•Edematous tissue is more easily
•Change positions at least every 2 hr(supine, side lying) and possibly more often if placed on affected side.
•Prop extremities in functional position; use footboard during the period of flaccid paralysis. Maintain neutral position of head.
•Elevate arm and hand
•Place pillow under axilla to abduct arm.
•Observe affected side for color, edema, or other signs of compromised circulation.
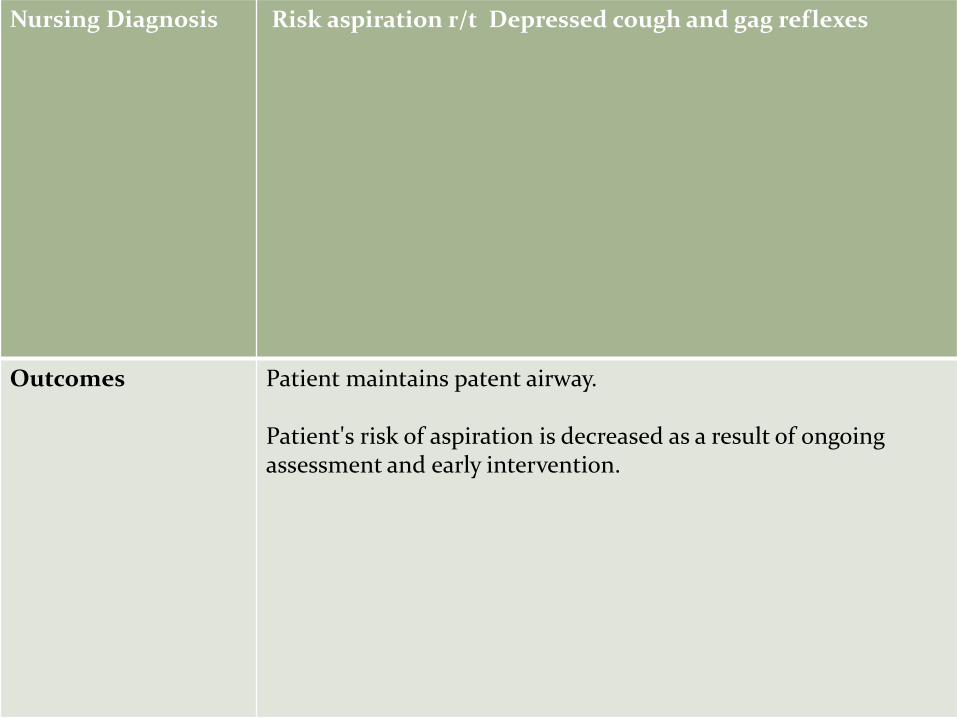
Depressed cough and gag reflexes Risk aspiration r/t Nursing Diagnosis
Patient maintains patent airway.
Patient's risk of aspiration is decreased as a result of ongoingassessment and early intervention.
Outcomes
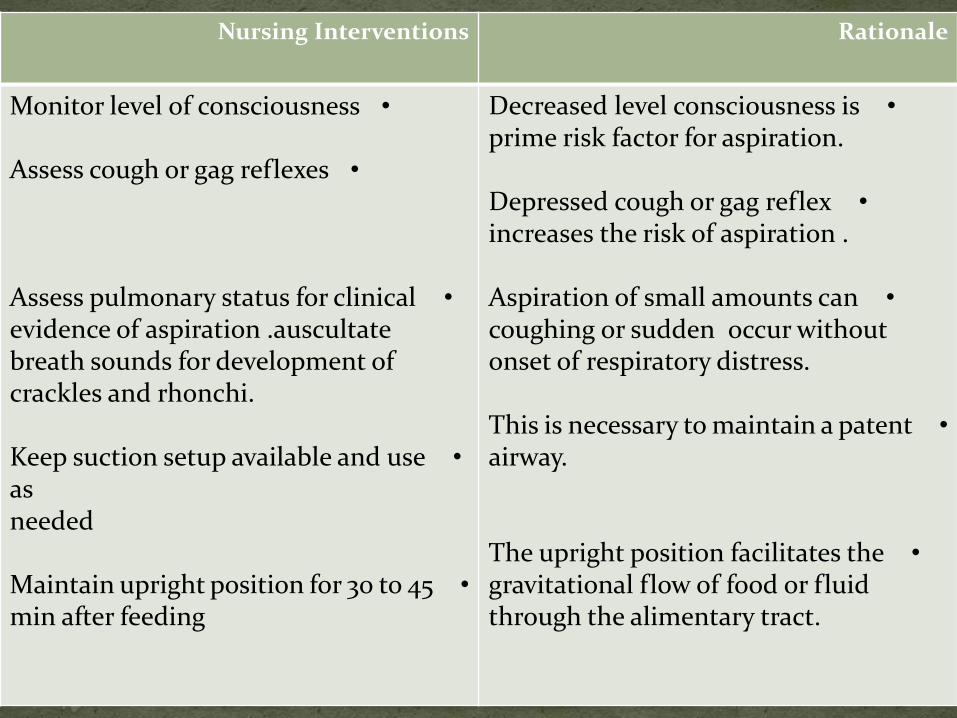
RationaleNursing Interventions
•Decreased level consciousness is prime risk factor for aspiration.
•Depressed cough or gag reflex increases the risk of aspiration .
•Aspiration of small amounts can occur without coughing or sudden
onset of respiratory distress.
•This is necessary to maintain a patent airway.
•The upright position facilitates the gravitational flow of food or fluid through the alimentary tract.
•Monitor level of consciousness
•Assess cough or gag reflexes
•Assess pulmonary status for clinical evidence of aspiration .auscultate breath sounds for development of crackles and rhonchi.
•Keep suction setup available and use as needed
•Maintain upright position for 30 to 45 min after feeding
Recommendation..
Community rehabilitation and follow-up services
a) health services with a stroke unit should provide comprehensive, experienced multidisciplinary community rehabilitation and adequately resourced support services for stroke survivors and their families/carers. If services such as the multidisciplinary community rehabilitation services and carersupport services are available, then early supported discharge should be offered for all stroke patients with mild to moderate disability.
b) rehabilitation delivered in the home setting should be offered to all stroke survivors as needed. Where home rehabilitation is unavailable, patients requiring rehabilitation should receive centre- based care.
c) Contact with and education by trained staff should be offered to all stroke survivors andfamilies/carers after discharge.
d) Stroke survivors can be managed using a case management model after discharge. If used, case managers should be able to recognise and manage depression and help to coordinate appropriate interventions via a medical practitioner.
e) Stroke survivors should have regular and ongoing review by a member of a stroke team, including at least one specialist medical review. the first review should occur within 3 months, then again at 6 and 12 months post-discharge.
f) Stroke survivors and their carers/families should be provided with contact information for the specialist stroke service and a contact person (in the hospital or community) for any post-discharge queries for at least the first year following discharge.
g) every stroke patient should be assessed and informed of their risk factors for a further stroke and possible strategies to modify identified risk factors.
• stopping smoking and avoiding excessive alcohol .• improving diet: a diet low in fat (especially saturated fat) and sodium but high in fruit andvegetables• increasing regular exercise• Control high Blood Pressure• Manage stress
Conclusion...
• The results of a stroke vary depending on the size and location, the presence of any associated medical problems, the likelihood of recurrent strokes.
• correspond to the area in Dysfunctions the brain that had been damaged.
http://www.medicalnewstoday.com/articles/7624.php
THANK YOU