Embed Size (px)
Citation preview

Introduction to
Cardiovascular
Disorders

Introduction
Cardiovascular disease is the most frequent cause
of adult death in the Western world
Incidence of ischaemic heart disease is rising Asia
Valvular heart disease is common, but the aetiology
varies in different parts of the world
Indian subcontinent and in Africa, it is predominantly
due to rheumatic fever, whereas calcific aortic
valve disease is the most common problem in
developed countries

Functional Anatomy
and Physiology

Anatomy
heart acts as two serial pumps
right heart circulates blood to the lungs where it
is oxygenated
left heart receives this and circulates it to the rest
of the body
atria - thin-walled structures that act as priming
pumps for the ventricles
The interatrial septum separates the two atria
20% of adults a patent foramen ovale is found


RA receives blood from the superior and inferior venae cavae and
the coronary sinus
LA receives blood from four pulmonary veins
ventricles - thick-walled structures, adapted to circulating blood
through large vascular beds under pressure
atria and ventricles are separated by the annulus fibrosus,
forms the skeleton for the atrioventricular (AV) valves
Electrically insulates the atria from the ventricles
LV myocardium is normally around 10 mm thick (c.f. RV thickness of 2–3 mm) because it pumps blood at a higher pressure


normal heart occupies less than 50% of the
transthoracic diameter in the frontal plane, as
seen on a chest X-ray
In disease states or congenital cardiac
abnormalities, the silhouette may change as a
result of hypertrophy or dilatation.

The coronary circulation
left main and right coronary arteries arise from the left and right
coronary sinuses of the aortic root
left main coronary artery divides into LAD, which runs in the anterior interventricular groove, and the LCX, which runs posteriorly in the
atrioventricular groove
LAD - anterior part of the septum (septal perforators) and the
anterior, lateral and apical walls of the LV
LCX - lateral, posterior and inferior segments of LV


RCA runs in the right atrioventricular groove
Supply RA, RV and inferoposterior aspects of the LV
PDA runs in the posterior interventricular groove
supplies the inferior part of the interventricular septum
branch of the RCA in approximately 90% of people (dominant right system)
supplied by the LCX in the remainder (dominant left system).
RCA supplies the SA node in about 60% of and the AV node in about 90%.

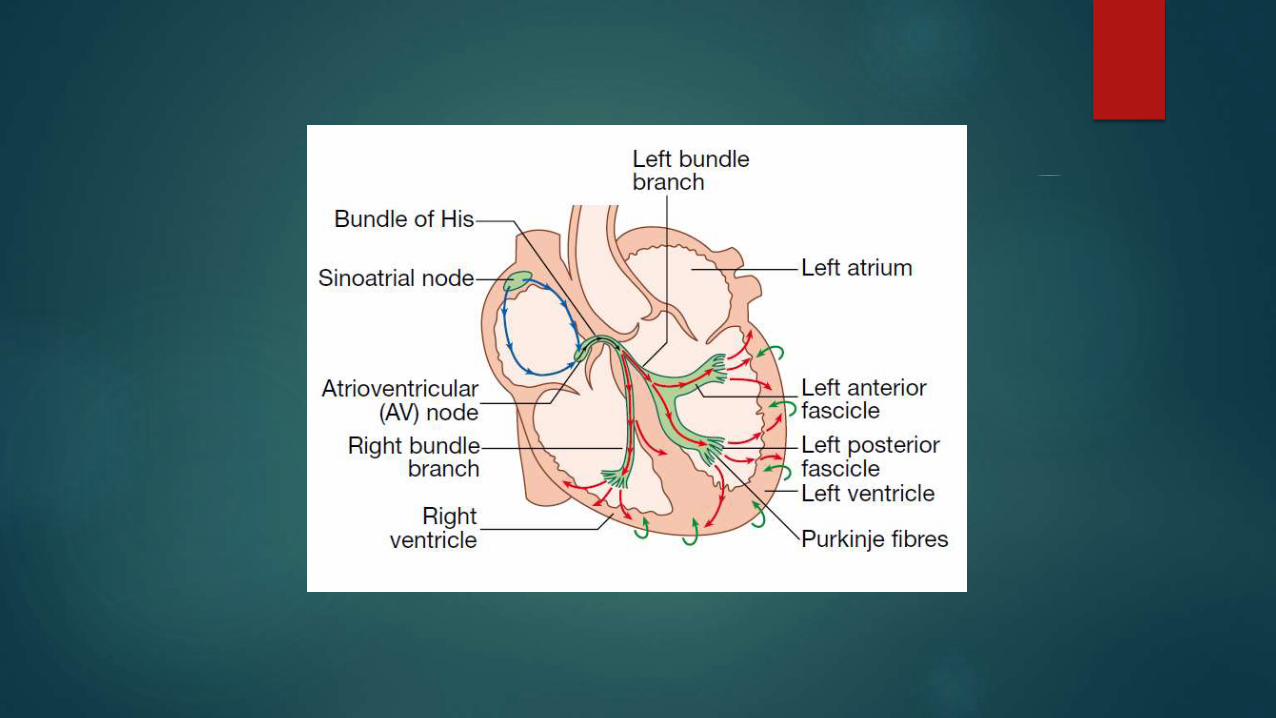
Conducting system of the heart
SA node is situated at the junction of the superior vena cava and RA
Specialised atrial cells that depolarise at a rate influenced by the
autonomic nervous system and by circulating catecholamines
annulus fibrosus forms a conduction barrier between atria and
ventricles
Only pathway through it is the AV node - conducts relatively slowly,
producing a necessary time delay between atrial and ventricular
contraction.
His–Purkinje system – comprised of the bundle of His, the right and left bundle branches, anterior and posterior fascicles of the left
bundle branch, and the smaller Purkinje fibres

Nerve supply of the heart
innervated by both sympathetic and parasympathetic fibres
Adrenergic nerves from the cervical sympathetic chain supply
muscle fibres in the atria and ventricles and the electrical conducting system
Positive inotropic and chronotropic effects are mediated by β1-
adrenoceptors
Parasympathetic pre-ganglionic fibres and sensory fibres reach the
heart through the vagus nerves
Cholinergic nerves supply the AV and SA nodes via muscarinic (M2) receptors

Cardiac Ultrastructure
three-fourths of the ventricular mass is
composed of cardiomyocytes
60–140 m in length and 17–25 m in diameter
each cell branches and interdigitates with
adjacent cells.

intercalated disc permits electrical conduction via gap junctions,
and mechanical conduction via the fascia adherens, to adjacent
cells
basic unit of contraction is the sarcomere
striated appearance due to the Z-lines
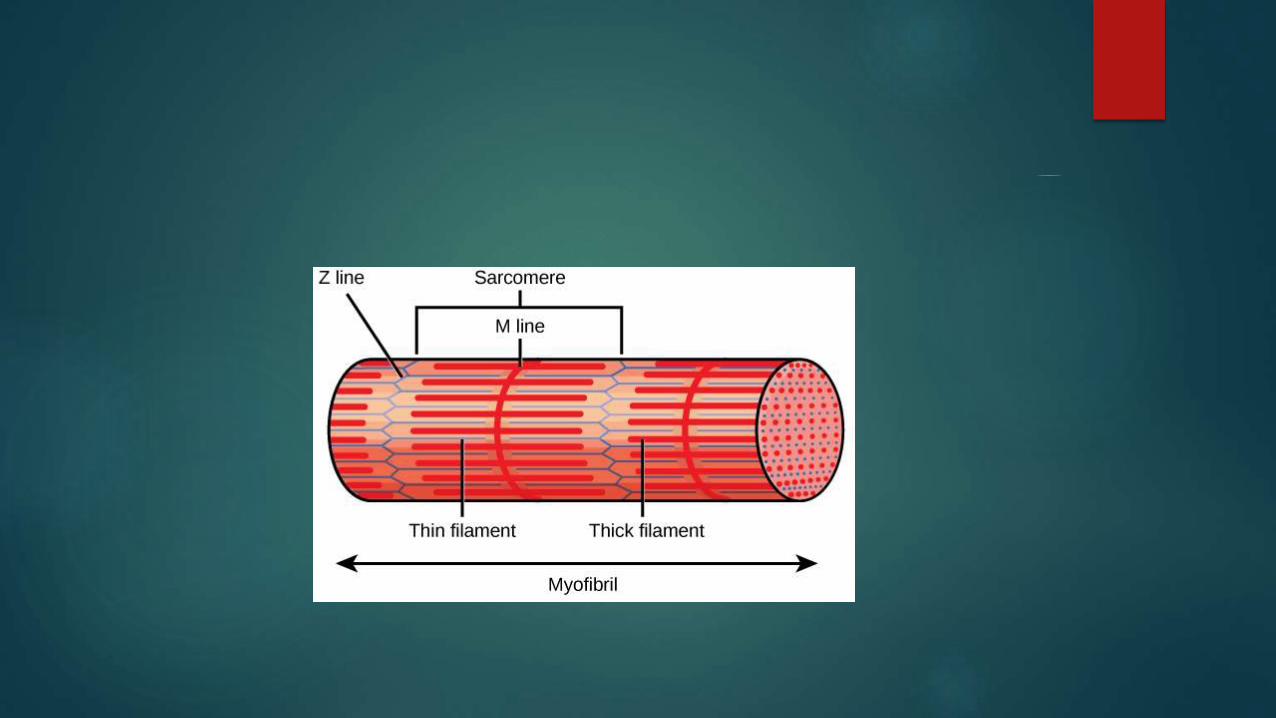

sarcomere
structural and functional unit of contraction
lies between adjacent Z lines
Within the sarcomere are alternating light and dark
bands - striated appearance under the light microscope
At the center of the sarcomere is a dark band of
constant length, the A band, which is flanked by two
lighter bands, the I bands, , which are of variable length


consists of two sets of interdigitating myofilaments
Thicker filaments, composed of myosin ,traverse the A
band
Thinner filaments, composed of actin course from the Z
lines through the I band into the A band
thick and thin filaments overlap only within the (dark) A
band, whereas the (light) I band contains only thin
filaments

The Contractile Process
Sliding filament model for muscle contraction
With activation, the actin filaments are
propelled farther into the A band
A band remains constant in length, whereas the
I band shortens and the Z lines move toward one
another


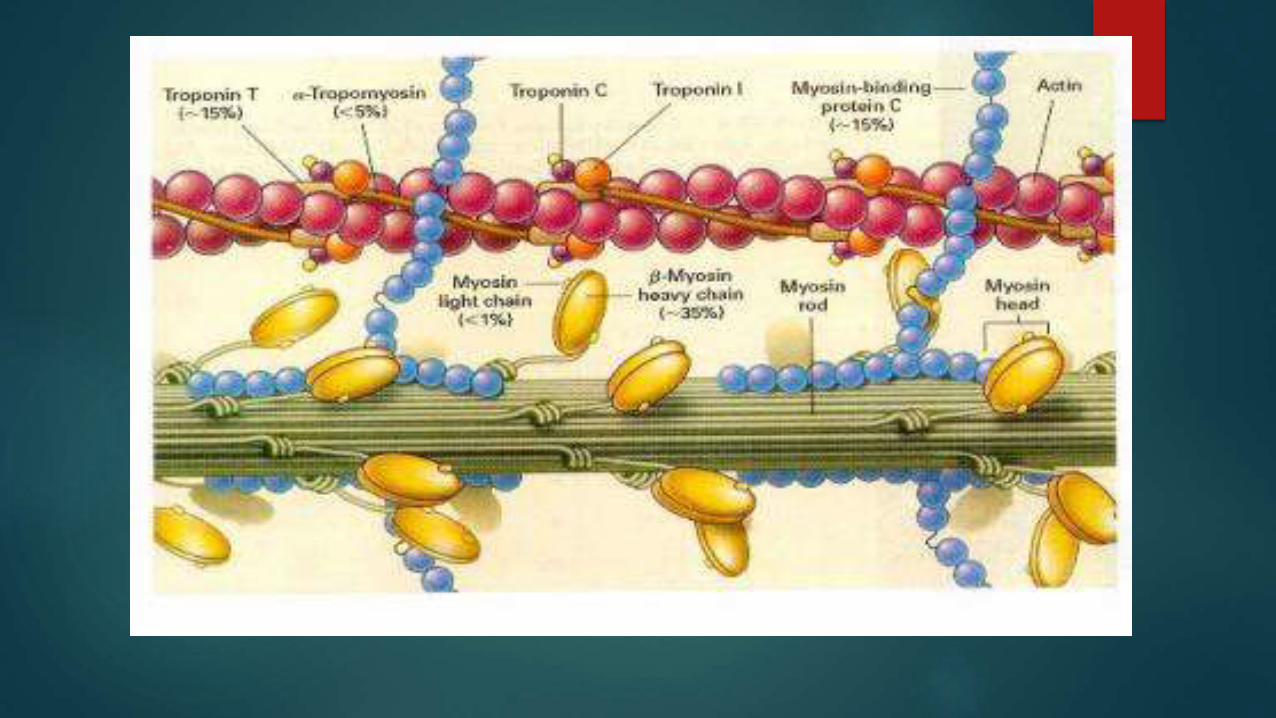
myosin molecule - has a rodlike portion with a globular portion (head) at its end
globular portions of myosin form the bridges between the myosin and actin molecules and are the site of ATPase activity
Actin molecule - double helix of two chains of actin molecules wound about each other on a larger molecule, tropomyosin
regulatory proteins—troponins C, I, and T—are spaced at regular intervals on actin

Four steps in cardiac muscle
contraction and relaxation
In relaxed muscle, ATP bound to the myosin head
dissociates the thick and thin filaments
actin binding site is blocked by tropomyosin
Step 1: Hydrolysis of myosin-bound ATP by the ATPase site
on the myosin head


Step 2: Ca2+ binds to troponin C, exposed active sites on
actin
actin interacts with the myosin head to form an active
complex
Step 3: The muscle contracts when ADP dissociates from
the myosin head
Step 4: The muscle returns to its resting state, when a new
molecule of ATP binds to the rigor complex and
dissociates the myosin head from the actin

Cardiac Action Potential
action potential has four phases
Potassium current (IK1) is the principal current during phase 4 and determines the resting membrane potential of the myocyte
Sodium current generates the upstroke of the action potential (phase 0)
activation of IKto with inactivation of the Na current inscribes early repolarization (phase 1)
The plateau (phase 2) is generated by a balance of repolarizing potassium currents and depolarizing calcium current
Inactivation of the calcium current with persistent activation of potassium currents (predominantly IKr and IKs) causes phase 3 repolarization


Cardiac output
Cardiac output is the product of stroke volume
and heart rate
Stroke volume is the volume of blood ejected in
each cardiac cycle
Dependent upon
end-diastolic volume and pressure (preload),
myocardial contractility
systolic aortic pressure(afterload)

Control of Cardiac Performance
and Output
the stroke volume of the ventricle depend on
three major influences
(1) the length of the muscle at the onset of
contraction, i.e., the preload
(2) the tension that the muscle is called on to
develop during contraction, i.e., the afterload
(3) the contractility of the muscle, i.e., the extent
and velocity of shortening at any given preload
and afterload

Determinants of Stroke Volume

Starling's law of the heart
The relation between the initial length of the
muscle fibers and the developed force
prime importance for the function of heart
muscle.
states that within limits, the force of ventricular
contraction depends on the end-diastolic length
of the cardiac muscle(ventricular end-diastolic
volume)

Laplace's law
Afterload is determined by the aortic pressure as well as
by the volume and thickness of the ventricular cavity
Laplace's law states that the tension of the myocardial
fiber is the product of the intracavitary ventricular
pressure and ventricular radius divided by wall thickness
afterload on a dilated left ventricle exceeds that on a
normal-sized ventricle
afterload on a hypertrophied ventricle is lower than of a
normal chamber

Epidemiology of Cardiovascular
Disease
Introduction
Cardiovascular disease (CVD) is now the most
common cause of death worldwide
Before 1900, infectious diseases and malnutrition
were the most common causes and CVD was
responsible for less than 10% of all deaths
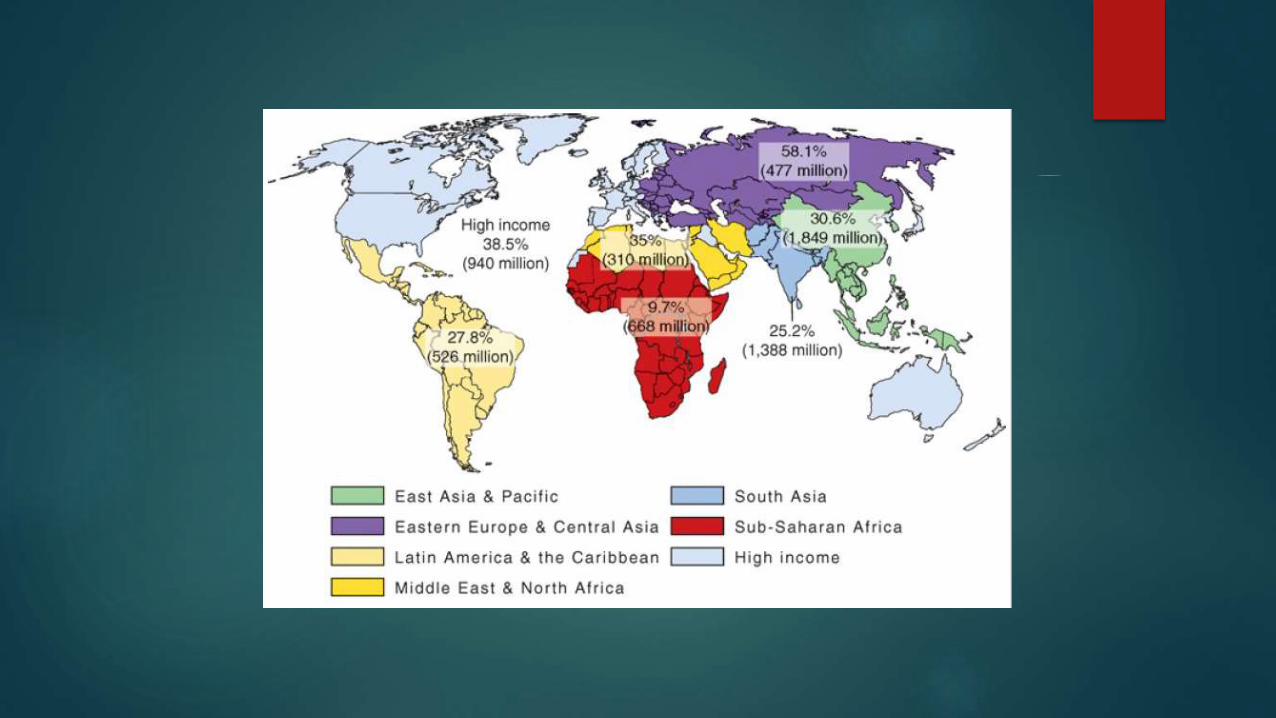
Today, CVD accounts for approximately 30% of
deaths worldwide, including nearly 40% in high-
income countries and about 28% in low- and
middle-income countries.


Known as THE EPIDEMIOLOGIC TRANSITION
driven by industrialization, urbanization, and
associated lifestyle changes
taking place in every part of the world among
all races, ethnic groups, and cultures
Three million CVD deaths occurred in high-
income countries in 2001, compared with 13
million in the rest of the world.

Global Trends in Cardiovascular
Disease
by 2001, CVD was responsible for 29% of all
deaths and 14% of the 1.5 billion lost DALYs
By 2030, when the population is expected to
reach 8.2 billion, 33% of all deaths will be the
result of CVD
Of these, 14.9% of deaths in men and 13.1% of
deaths in women will be due to CHD
Stroke will be responsible for 10.4% of all male
deaths and 11.8% of all female deaths

Behavioral Risk Factors
Tobacco
Tobacco currently causes about 5 million deaths—9% of all
deaths—annually.
Approximately 1.6 million are CVD-related
If current smoking patterns continue, by 2030 the global burden of
disease attributable to tobacco will reach 10 million deaths annually
Diet
increase in intake of saturated animal fats and hydrogenated
vegetable fats, which contain atherogenic trans-fatty acids, along with a decrease in intake of plant-based foods and an increase in
simple carbohydrates

Physical Inactivity
The increased mechanization that accompanies the economic
transition leads to a shift from physically demanding agriculture-based work to largely sedentary industry- and office-based work

Metabolic Risk Factors
Lipid Levels
Worldwide, high cholesterol levels are estimated to
cause 56% of ischemic heart disease and 18% of strokes,
amounting to 4.4 million deaths annually
Social and individual changes that accompany
urbanization clearly play a role because plasma
cholesterol levels tend to be higher among urban
residents than among rural residents
greater consumption of dietary fats—primarily from
animal products and processed vegetable oils—and
decreased physical activity

Hypertension
Worldwide, approximately 62% of strokes and
49% of cases of ischemic heart disease are
attributable to suboptimal (>115 mmHg systolic)
blood pressure, which is believed to account for
more than 7 million deaths annually
One major concern in low- and middle-income
countries is the high rate of undetected, and
therefore untreated, hypertension

Obesity
Although clearly associated with increased risk of CHD, much of the risk posed by obesity may be mediated by other CVD risk factors, including hypertension, diabetes mellitus, and lipid profile imbalances
Diabetes Mellitus
worldwide rates of diabetes—predominantly Type 2 diabetes—are on the rise
In 2003, 194 million adults, or 5% of the world's population, had diabetes
By 2025, this number is predicted to increase 72 percent to 333 million

Approach to the Patient with
Possible Cardiovascular Disease

Cardiac Symptoms
symptoms caused by heart disease result most
commonly from
myocardial ischemia
disturbance of the contraction and/or relaxation
of the myocardium
obstruction to blood flow
abnormal cardiac rhythm or rate

Chest pain

Breathlessness
Syncope
Palpitations
Pedal Edema
Fatigue

Diagnosis
As outlined by the New York Heart Association (NYHA),
the elements of a complete cardiac diagnosis include
the systematic consideration of the following
1. The underlying etiology. Is the disease congenital,
hypertensive, ischemic, or inflammatory in origin?
2. The anatomical abnormalities. Which chambers are
involved? Are they hypertrophied, dilated, or both?
Which valves are affected? Are they regurgitant and/or
stenotic? Is there pericardial involvement? Has there
been a myocardial infarction?

3 The physiological disturbances. Is an arrhythmia present? Is there
evidence of congestive heart failure or myocardial ischemia?
4 Functional disability. How strenuous is the physical activity required to elicit symptoms?

New York Heart Association
Functional Classification

Investigation of CardiovascularDisease
Basic tests
electrocardiography,
chest X-ray
Echocardiography
Procedures such as
cardiac catheterisation
Radionuclide imaging,
computed tomography (CT)
Magnetic resonance imaging (MRI)

Electrocardiogram (ECG)
used to assess cardiac rhythm and conduction
provides information about chamber size
main test used to assess for myocardial
ischaemia and infarction.