Embed Size (px)
DESCRIPTION
Internal medicine
Citation preview

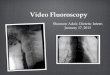
Picture QuizPicture QuizWhat is the diagnosis?What is the diagnosis?
Sandra Susanibar - UAMS

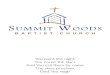
Picture QuizPicture QuizWhat is the diagnosis?What is the diagnosis?
Sandra Susanibar - UAMS
Pleural plaque

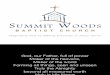
Picture QuizPicture QuizWhat is the diagnosis?What is the diagnosis?
Sandra Susanibar - UAMS
Pleural plaque

AsbestosisAsbestosis• Diagnosis:
o A reliable history of exposure to asbestos with a proper latency period (years) +
o Presence of markers of exposure (eg, pleural plaques or recovery of sufficient quantities of asbestos fibers/bodies in bronchoalveolar lavage or lung tissue) +
o Definite evidence of interstitial fibrosis +o Absence of other causes of diffuse parenchymal lung disease.
Sandra Susanibar - UAMS

Morning ReportMorning Report CaseCase
Sept 17, 2014

Case simulationCase simulation• ~50-60 yo woman comes in to clinic with fatigue,
mild confusion, and general malaise.• She doesn’t provide much more history, but has
been having a tough time with her family lately.• Physical exam is pretty unremarkable except her
cardiac exam reveals what sounds like sinus tachycardia ~130. You ask about chest pain, dyspnea, palpitations, n/v/d/anorexia, she denies all.
• You order an ECG…

ECG ECG

InterpretationInterpretation• Sinus tachycardia w q waves in II, III, aVF, ST
elevation w inverted waves in V2-6

Glad you got the ECGGlad you got the ECG• What now?• DC to home? Go to ED? Activate cath lab?

To the EDTo the ED• She goes to the ED, where cath lab has been
activated• Troponin is elevated, but less than 5. She
continues to deny chest discomfort/dyspnea.• (next slides are examples of left side and right
side pictures during a left heart cath example of this disease)



End of DiastoleEnd of Diastole(ventriculogram)(ventriculogram)
End of Systole

Diagnosis?Diagnosis?• STEMI w no evidence of acute ischemia on left
heart catheterization with left ventriculogram evidence of apical hypokinesis and mild global ejection fraction dysfunction…

Takotsubo Takotsubo CardiomyopathyCardiomyopathy
AKA Apical Ballooning SyndromeAKA Broken Heart Syndrome
AKA Stress-Induced Cardiomyopathy

DefinitionDefinition• Transient systolic dysfunction of the apical and/or
mid segments of the LV that mimics MI, but in the absence of obstructive coronary disease
• Decreased contractile function: apex of LV• Hyperkinesis: basal walls• Women>>>>>>Men• Prevalence 1.2% of troponin positive ACS
Uptodate.com

PathogenesisPathogenesis• Triggers: acute illness,
intense emotional or physical stress
• Proposed mechanisms:o Catecholamine excesso Coronary artery spasmo Microvascular dysfunction
• Catecholamine excesso Mouse Model: switch from Beta-2 Gs
(positively inotropic) to beta-2 Gi (negatively inotropic); higher levels of epinephrine act on Gi
Uptodate.comMedscape.com

Clinical PresentationClinical Presentation• Similar to Acute MI
o Acute substernal Chest Pain (most common)o Dyspnea, syncope, shocko EKG abnormalities (ST elevation anterior precordial leads)o Mild troponin elevations (<5.2)
• Acute Complicationso Heart failureo Tachy and Bradyarrhythmiaso Mitral regurgitationo Cardiogenic shocko LV outflow tract obstructiono Apical thrombus formation and stroke
Uptodate.com

DiagnosisDiagnosis• Suspect in postmenopausal women who
experience severe stress and present with ACS and have presentation/EKG findings out or proportion to cardiac markers
Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, et al. Systematic Review: Transient Left Ventricular Apical Ballooning: A Syndrome That Mimics ST-Segment Elevation Myocardial Infarction. Ann Intern Med. 2004;141:858-865.

TreatmentTreatment• Therapy is based upon patient’s overall clinical
condition• If they have symptoms of HF and fluid overload
o ACE-I, BB, Diureticso Treat until systolic function recovers (1-4 weeks)
• Coexisting coronary atherosclerosiso Aspirin
• Due to possibility of recurrence (up to 10%)o Continue adrenergic blockade with BB or combined AB/BB indefinitely unless
contraindicated
• Hypotension and Shock: Get urgent ECHO to determine if LVOT obstruction is present (13-18%)o No LVOT: can cautiously use inotropes (dobutamine, dopamine) or IABPo LVOT: BB, fluid replacement
• Thrombus: Get an ECHO to checko 3 months of anticoagulation if LV thrombus detectedo No thrombus but severe LV dysfunction: 3 months or until function is normalo Prophylaxis: 10 days anticoagulation
Uptodate.com

PrognosisPrognosis• In-hospital mortality rates: 0-8%• Normal ventricular function typically returns in 1-
4 weeks• Study of 100 patients
o Mean follow up 4.4 +/- 4.6 yearso 31 patients had continued chest paino 10 had recurrenceo 17 died (no difference compared to age/gender matched population)
Uptodate.com
Elesber AA, Prasad A, Lennon RJ, Wright RS, Lerman A, Rihal CS. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J Am Coll Cardiol. 2007;50(5):448.