Embed Size (px)
DESCRIPTION
Citation preview

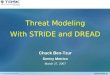
P4 Patient-Centered Medical Home Features
Resident Ratings of Importance*
Baseline (2007)Mean (SD)
Resident Ratings of Importance*
Midstride (2009)Mean (SD)
Difference between Baseline
and Midstride Results
EHR (Electronic Health Record) in practice 4.44 (0.89) 4.50 (0.86) +0.06 (2%)
Practice as paperless 3.99 (1.05) 4.07 (1.10) +0.08 (2%)
Fully secured remote access available 4.60 (0.85) 4.64 (0.66) +0.04 (1%)
Secure HIPPA-compliant email with patients 3.61 (1.31) 3.61 (1.30) 0
Ongoing population-based QA using an EHR 3.44 (1.44) 3.48 (1.43) +0.04 (2%)
Chronic disease management registries 4.01 (1.11) 3.93 (1.21) -0.08 (2%)
EHR-based preventive services registries 4.13 (1.14) 4.01 (1.14) -0.12 (3%)
Practice-based research done using an EHR 3.28 (1.40) 3.40 (1.33) +0.12 (4%)
Group visits 3.33 (1.35) 3.31 (1.49) -0.02 (1%)
Integrated "case management" and social services
4.32 (0.90) 4.32 (0.97) 0
Using teams to manage patient care
3.84 (1.19) 3.91 (1.18) +0.07 (2%)
Integrated behavioral health 4.12 (0.93) 4.14 (1.11) +0.02 (1%)
Innovations in Residency Training: Midstride Findings from the P4 Project
BACKGROUND
Larry Green, MD1; Patricia Carney, PhD, Patrice Eiff, MD, Elaine Waller2 ; James Puffer, MD3
1University of Colorado Denver, 2Oregon Health & Science University, 3American Board of Family Medicine
QUANTITATIVE CORE DATA Core Data are collected from all P4 sites: 1) Program Data; 2) Resident Survey; 3) Continuity Clinic Data; 4) Grad Survey
QUALITATIVE DATA
On-line diary entries from faculty, residents, staff
SITE SPECIFIC DATAEach program is additionally using specific measures designed to test their innovation-specific hypotheses
• P4 is an Observational Case Series Study of Revisions to FM Residency Training
• 14 Representative Residency Programs are Participating and are Nearing the 4th Year of the 6 Year project
• Key Innovations include: 4 Years of Training Different Ways of Teaching Elements
of the Patient Centered Medical Home Individualized Training Early Establishment of a Panel of Continuity Patients
Innovation Focus
No. of programs with this
focus
Total No. of residents training at sites with this focus
Programs
PCMH Practice Re-design 9 192
Baylor, Cedar Rapids, Colorado, Hendersonville, Lehigh Valley, Middlesex, Missouri, Rochester, West Virginia Rural
Individualized Curriculum “Intentional Diversification” 7 195
Cedar Rapids, Christiana, JPS, Lehigh Valley, Middlesex, Tufts-CHA, Waukesha
4 year Curriculum 6 186
JPS, Loma Linda, Middlesex, Missouri, Waukesha, West Virginia Rural
Team-based Care & Training in Teams 6 117
Baylor, Cedar Rapids, Hendersonville, Lehigh Valley, Middlesex, Rochester
Chronic Disease Management 5 108
Baylor, Cedar Rapids, Middlesex, Missouri, West Virginia Rural
Longitudinal Curriculum 4 93Colorado, Middlesex, Tufts-CHA, Waukesha
Re-Sequencing of Curriculum 4 78Baylor, Cedar Rapids, Colorado, Lehigh Valley
Less Inpatient Time & More Continuity Clinic Time (esp. PGY1) 4 87
Baylor, Christiana, Lehigh Valley, Missouri
Small Group Learning Labs/Problem-based Learning 4 84
Christiana, Hendersonville, Lehigh Valley, Missouri
Patient-Centered Care 4 96Lehigh Valley, Loma Linda, Missouri, West Virginia Rural
Learner Portfolios 3 66Lehigh Valley, Tufts-CHA, Waukesha
Community/Population Health Focus 3 57Colorado, Hendersonville, Loma Linda,
Community Practices as Training Sites 2 30 Hendersonville, Lehigh Valley
Resident Attitudes About Importance of PCMH
Features at Baseline and Midstride
*0=Don’t know, 1=Neutral/No Opinion; 2=Not at all important; 3=Somewhat important; 4=Moderately important; 5=Very important
MIDSTRIDE PRELIMINARY RESULTS
NEXT STEPS
Applicant and Match Experience of P4 Programs
Pre (2006/07) and Post (2008/09)
The mean number of US senior applicants increased more than
national trends
% of positions filled by US seniors higher than national average
(pre and post)
Programs that implemented customized training may have improved
performance in the match
P4 Recommendations to the FM-RC
Assess compliance with metrics other than time
Require continuing, comprehensive care to a panel of patients
Broaden definition of continuity beyond face-to-face contact in the
clinic (e.g. EHR, email, care teams)
Sustain core skills and expect customization to meet the needs of
individual learners
Allow more flexibility
Center FM training in the evolving model of the PCMH
Information management skills are essential
Training Residents in a PCMH is in Evolution
It’s unclear which approach is better: immerse residents in a
re-designed practice versus specific training to work in the PCMH
environment
New skills required that have been identified:
Working in teams
Managing chronic care
Population management
Process improvement skills
The Definition of Continuity of Care is Broadening Beyond
Face-to-Face Contact
Flexible Training Options that Address Individual Needs of
Learners While Addressing Core Skills are Educationally Valid
Shifting to Competency-based Assessment is Complex and Resource-Intensive
Educational learner portfolios can be a useful tool to
assess competency and enhance self-directed learning but
are faculty and resident time-intensive
Faculty Development Needs Are Paramount
Change fatigue and faculty burn-out are serious concerns
Faculty experience difficulty teaching the features of the PCMH
when the concept is emerging and changing and they themselves
are relative novices in practicing within a medical home
Residents are farther along than faculty in adopting new
information technology & the EMR
There is a shift required from the traditional pedagogical
approach to a “learning and discovering together” approach
Residency Re-design Requires Additional Financial Support
Rigorous Evaluation Must Accompany Innovation
Identify site-specific variables/measures that could be pooled to provide more power to assess common thematic intervention areas.
Disseminate the results of the Project through publications, presentations at national meetings and quarterly newsletters.
Secure additional funding to extend the project to years 6 and 7 to expand the number of cohorts of residents who have fully participated in the P4 project and for whom we have both core data and graduate survey data.
Continue to build the infrastructure necessary for a Primary Care Educational Research Network (PCERN) using P4 as the foundation to accomplish both practice transformation and translating research into practice via educational settings.
METHODS
For more information visit www.transformed.com/p4.cfm
P4 Manuscripts in Progress
Effect of curriculum innovation on residency applications and match performance: A P4 report
Preparing the Personal Physician for Practice (P4): Baseline innovations, hypotheses, measures and project trajectory
Designing Measures for Educational Innovation for the Preparing the Personal Physician for Practice (P4) Project: A Model for Centers of Excellence in Medical Education research
A report from Preparing the Personal Physician for Practice (P4): midstride preliminary results and emerging themes


![STRIDE-based Threat Modeling for Cyber-Physical Systems · STRIDE-based threat modeling can be performed in two possible ways [22]: (i) STRIDE-per-element and (ii) STRIDE-per-interaction](https://img.pdfslide.us/doc/110x75/5ec0069865be937c564c10b3/stride-based-threat-modeling-for-cyber-physical-systems-stride-based-threat-modeling.jpg)