Embed Size (px)
Citation preview
MANAGEMENT OF INFLAMMATORY BOWEL
DISEASE
Dr ANKITA MISHRAJNMCH
AMU,ALIGARH
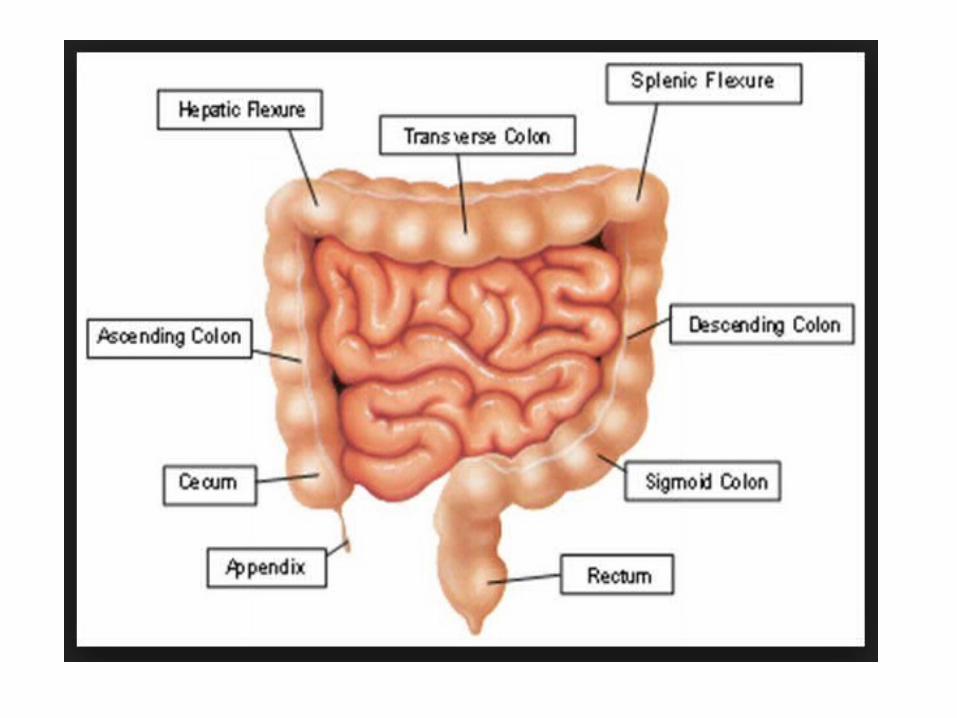
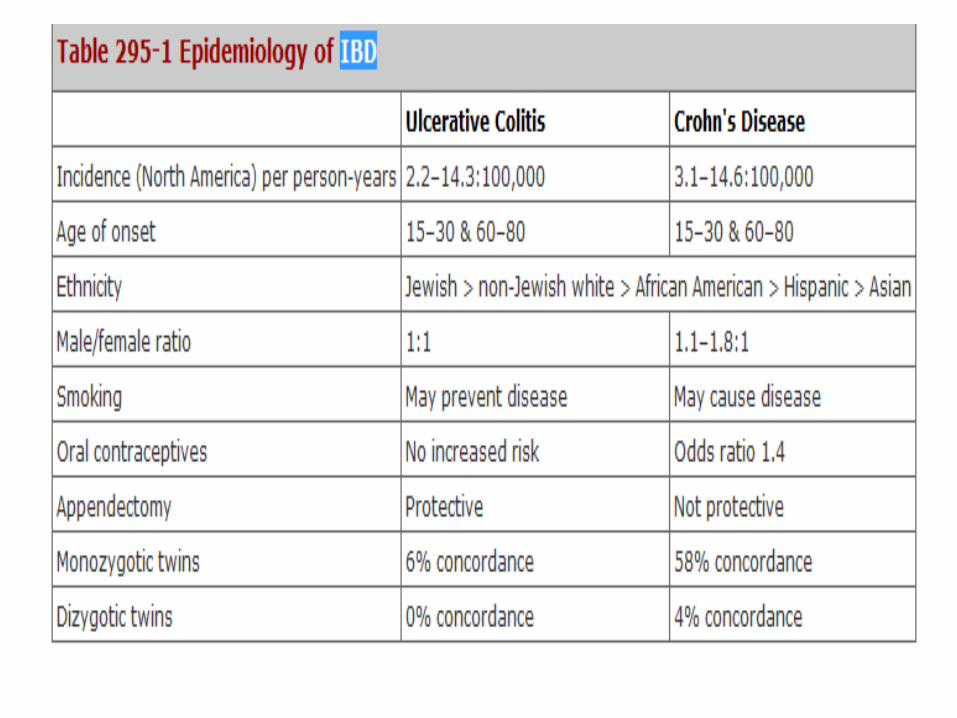
Inflammatory Bowel Disease
• Inflammatory bowel disease (IBD) is a spectrum of chronic idiopathic inflammatory gastrointestinal conditions.
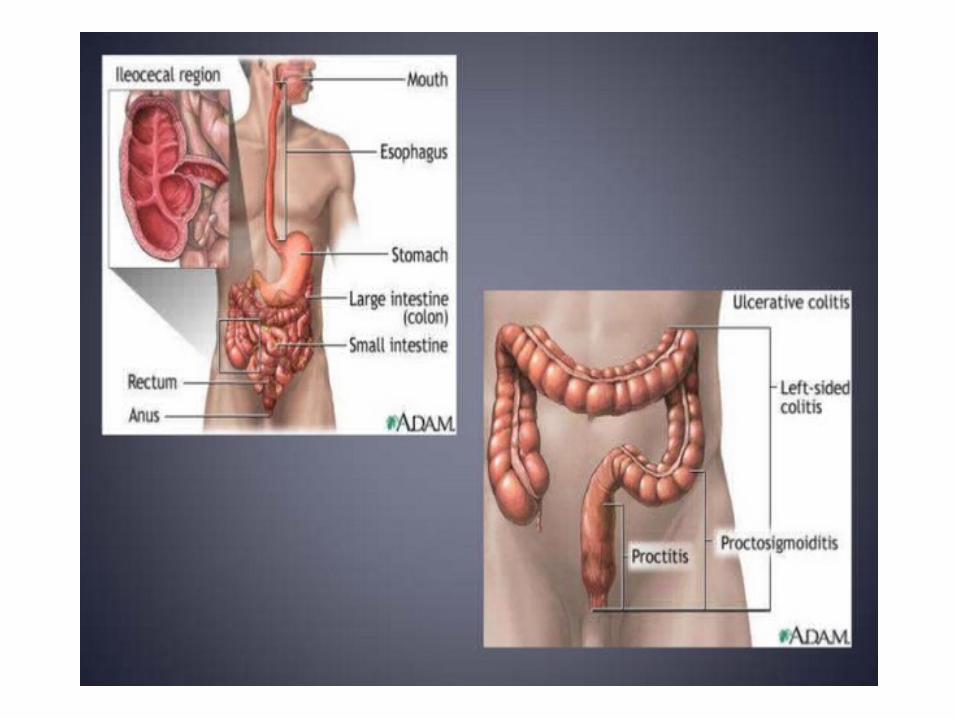
• Two major types of IBD:– Ulcerative colitis (UC) – Crohn's disease (CD)
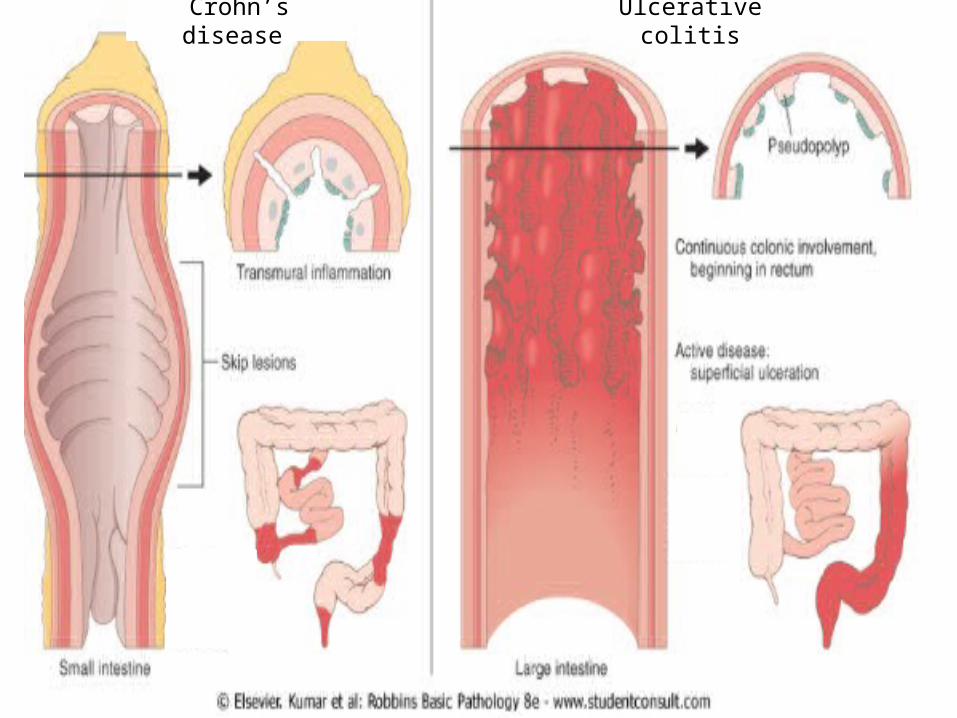
Crohn’s disease Ulcerative colitis
Etiopathogenesis
• Exact cause is unknown• Genetic factors(NOD2/CARD15)• Immunological factors(defective
immunosuppresion)• Microbial
factors(campylobacter,mycobacterium)• Psychosocial factors(smoking,stress)
IL12/IL18
IL-1
CLINICAL FEATURES Crohn’s disease- Diarrhoea Abdominal Pain Weight loss Malabsorption Steatorrhea
Ulcerative colitis- Rectal bleeding
TenesmusPassage of mucousAbdominal pain
DRUG THERAPY FOR IBD
GOALS OF THERAPY • Relief of symptoms • Induction of remission in patients of active disease
• Prevention of relapse(maintenance therapy)
• Healing of fistula
• Avoidance of emergent surgery
Ulcerative colitis• Active disease• 5ASA therapy• Glucocorticoids• Infliximab• Cyclosporine• Maintenance• 5ASA therapy• AZA/6-MP
Crohns disease• Active disease• 5ASA therapy• Glucocorticoids• Biological therapies• Methotrexate• Antibiotics• Maintenance• Azathioprine• Biological therapies
Mesalamine(5-ASA)based therapyUSES
• Mild to moderate UC & CD• Induce remission in both UC & CD• Maintain remission in UC• No role in maintaining remission in CD
SULFASALAZINE(prototype)
• 5-ASA + sulfapyridine by an azo bond
• Developed originally for rheumatoid arthritis.
• Therapeutic moiety- 5ASA
• Cleaved by Azo-reductase(colonic bacteria).
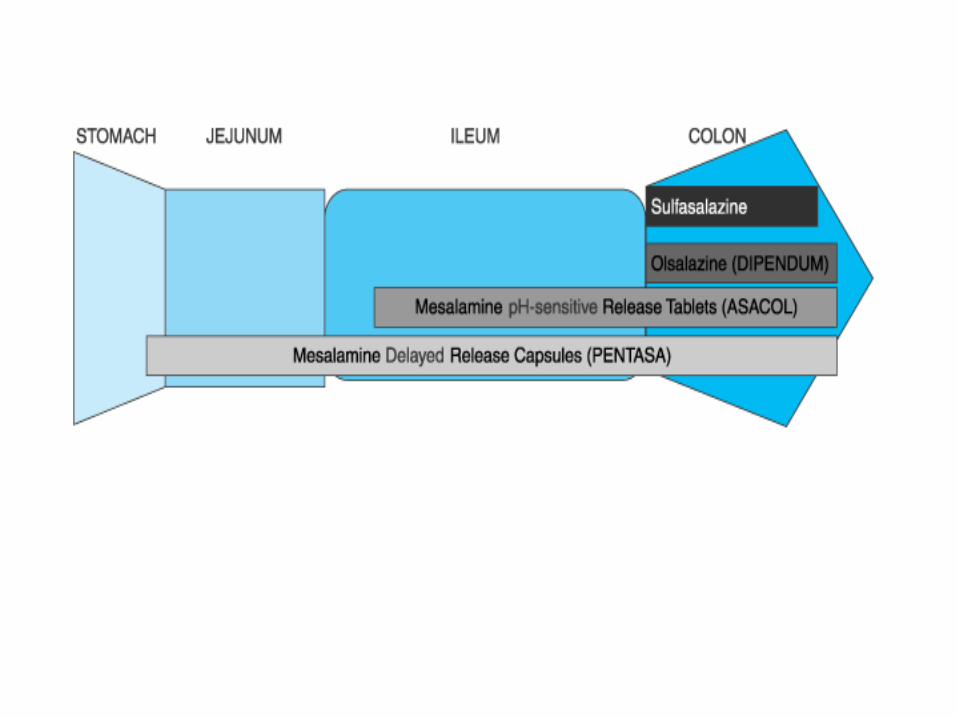
second-generation 5-ASA compounds two groups:
–Prodrugs: – 5ASA + 5-ASA (olsalazine) – 5ASA + 4ABA(balsalazide).
–Coated drugs: MESALAMINE(5ASA)– delayed-release formulation (Pentasa)– pH-sensitive coating.(Asacol)
DOSING • Oral prepartions• Sulfasalazine• Initial dose of 500 mg BD 4gm /day,4times with food• Doses as high as 6 g/day can be used• Maintenance- 1gm twice daily
• Asacol• 800mg thrice daily(active disease)• 800mg twice daily(maintenance)• Pentasa• 1-4gm,4times a day(active disease)
Active disease
• Balsalazide• Active disease- 2.25 gm thrice daily• Maintenance-1.5 gm twice daily
• Olsalazine• 1-3 gm / day
• Topical preparations---• Mesalamine suppository —• Used in active proctitis• 500mg ,2-3 times/day- atleast 3hrs
• Mesalamine enema —• Used in distal ulcerative colitis• 4gm/60ml,bedtime-atleast 8hrs
Adverse Effects• Occur in 10-45% of pts. ( related primarily to sulfa moiety)• Some are dose-related:
– Headache – Nausea – Fatigue – Bone marrow suppresion
• Allergic reactions: – Rash– Fever – Pneumonitis
• Also inhibits intestinal folate absorption• Olsalazine-diarrhoea Mesalamine-interstitial nephritis
Give with meals/Decrease the dose
GLUCOCORTICOIDS• Effects on inflammation - numerous & well documented.• Effective in acute exacerbations of UC or CD• Given for moderate to severe conditions.• Not effective in maintaining remission.
• Responders to steroids - three general classes: – steroid-responsive (40%): improve clinically, within 1-2 wk. ,
remain in remission as steroids- tapered & discontinued.– steroid-dependent (30-40%): also respond - experience a
relapse of symptoms as dose tapered.– steroid-unresponsive (15-20%): do not improve even with
prolonged high-dose.
DOSE & FORMULATIONS
• ORAL• Prednisone (for moderate to severe exacerbation)• 40-60mg/day• Dose tapered over wks. to months (@<=5mg/wk)• Most pts. improve within 5 days.
• Budesonide (ileocecal CD)• Enteric release form • 9mg/day(up to 8wks in active disease)• 6mg/day(maintenance up to 3mths)
• TOPICAL• Hydrocortisone• Retention enemas(100mg/60ml)• Disease limited to rectum & lt. colon• 60ml enema/night(2-3wks)
• Cortifoam(10% foam suspension)• Distal proctitis& difficulty in retaining fluid• Once/twice daily(80 mg per application)
• I/V
• Severe U.C & C.D.• Methylprednisolone- 40-60mg/day• Hydrocortisone-300mg/day
SIDE EFFECTS• The side effects are numerous, – fluid retention– Susceptibility to infection– fat redistribution– hyperglycemia – osteonecrosis– Myopathy
IMMUNOSUPPRESSIVE AGENTS
• AZATHIOPRINE &MERCAPTOPURINE
• METHOTREXATE
• CYCLOSPORINE
Thiopurine Derivatives
Azathioprine & Mercaptopurine USES• Steroid dependent disease• Steroid unresponsive• Recurrent flares requiring repeated steroids• Equally effective in CD & UC• Maintains remission & prevents recurrence in
CD after surg. resection.
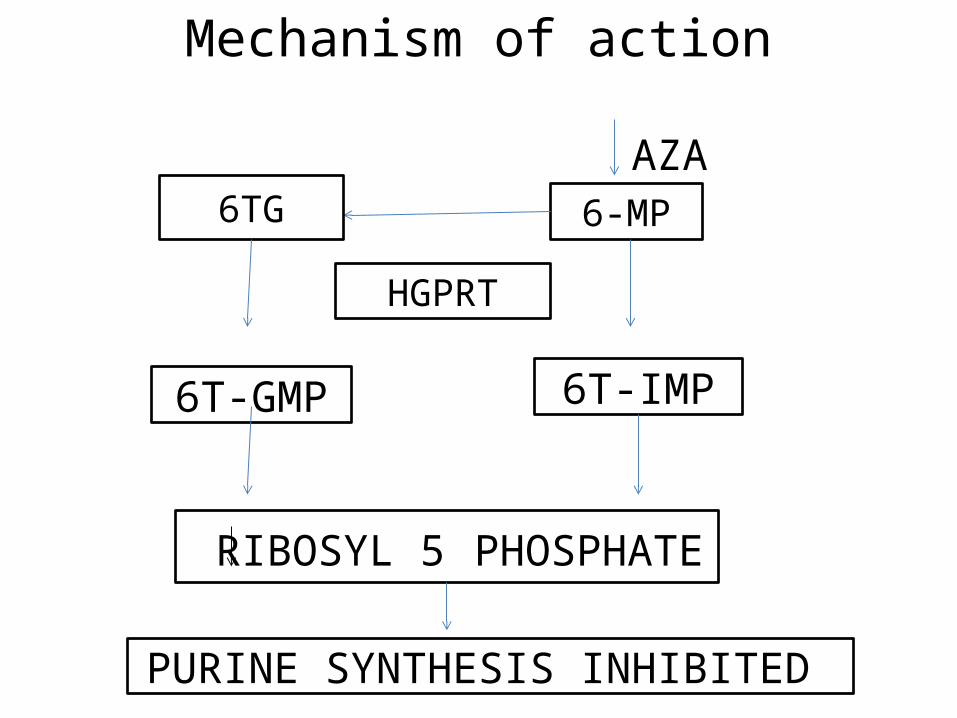
Mechanism of action AZA
6-MP6TG
HGPRT
6T-GMP 6T-IMP
RIBOSYL 5 PHOSPHATE
PURINE SYNTHESIS INHIBITED
Dosage• Azathioprine– oral 2-2.5mg/kg/day
• Mercaptopurine– oral 1.5mg/kg/day
• Clinical response in 6-8 wks
Adverse effects • Idiosyncratic:– Pancreatitis– Fever– Rash– Arthralgias
• Dose-related:– Bone marrow suppression– Elevations in liver enzymes– Increased risk of infection
• Possible:– risk of hematological malignancies (non-Hodgkin's
lymphoma)
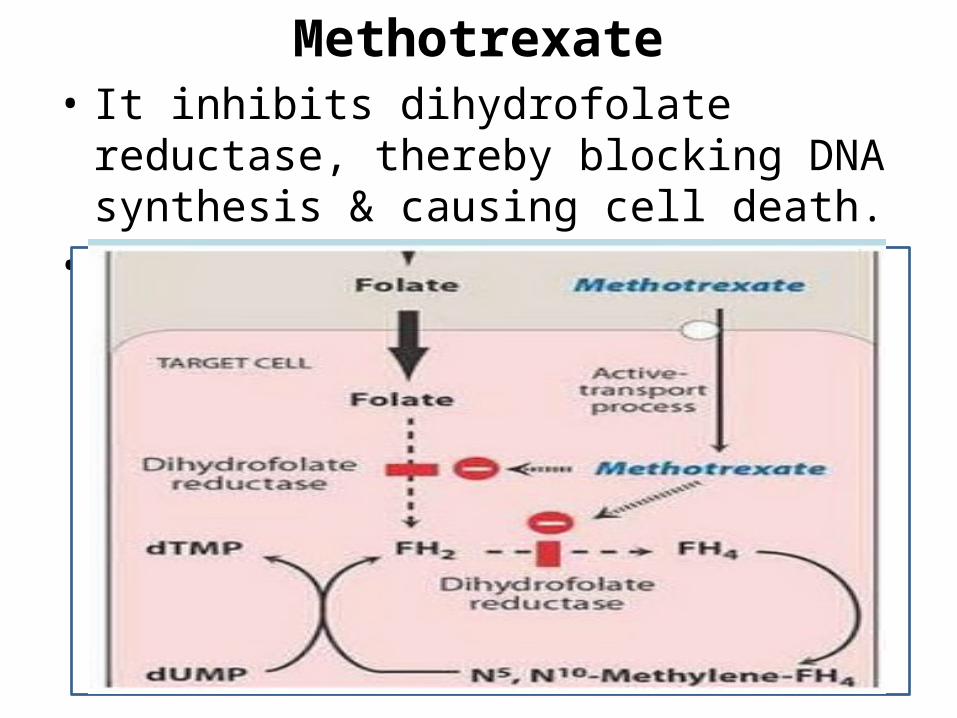
Methotrexate• It inhibits dihydrofolate reductase, thereby
blocking DNA synthesis & causing cell death.• Also decreases IL-1 production.
Methotrexate
• USE-steroid-resistant or steroid-dependent CD• In CD- induces & maintains remission, more
rapid response than 6MP or azathioprine.• In UC -not thoroughly investigated.• DOSE- 15-25 mg/wk, given IM/SC. • ADRs-
leukopenia,hepatotoxicity,nephrotoxicity,neu-rotoxicity
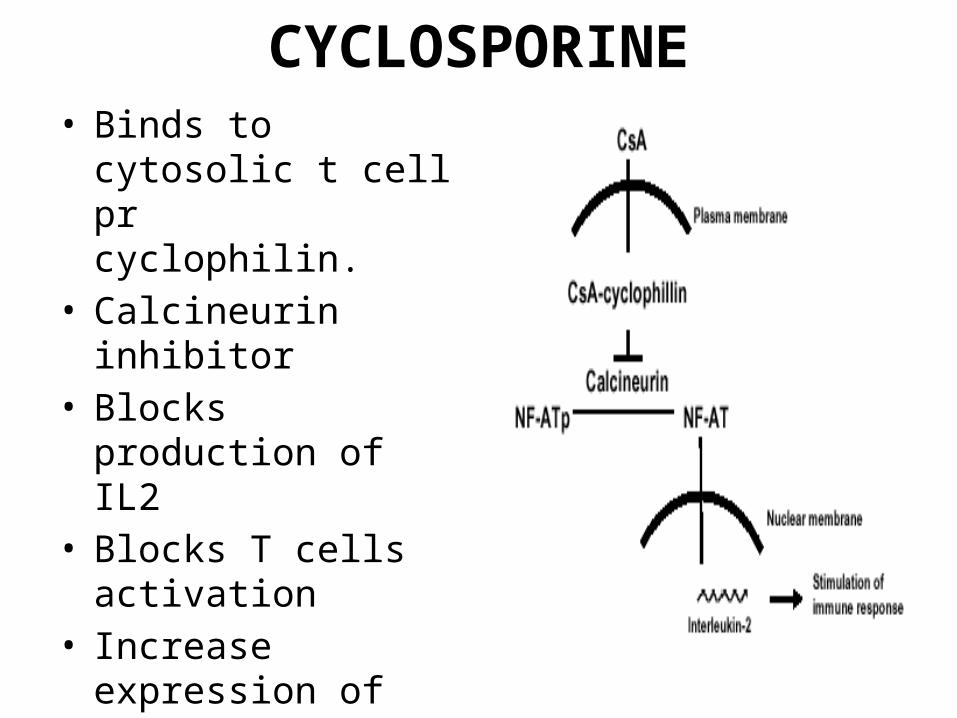
CYCLOSPORINE• Binds to cytosolic t cell
pr cyclophilin.• Calcineurin inhibitor• Blocks production of IL2• Blocks T cells activation• Increase expression of
TGF beta
USES• Severe UC - failed to respond adequately to
steroid therapy.• Fistulous complication(CD)-rapid response but
frequent relapse
• Not effective in maintenance therapy
DOSAGE
• I/V Cyclosporine– 2-4mg/kg/day• Careful monitoring to maintain therapeutic level
b/w 300-400ng/ml
ADR
• Nephrotoxicity• Neurotoxicity• Hepatotoxicity• Hypertension• Hirsuitism
BIOLOGICAL THERAPIES
• INFLIXIMAB• ADALIMUMAB• CERTOLIZUMAB PEGOL• NATALIZUMAB
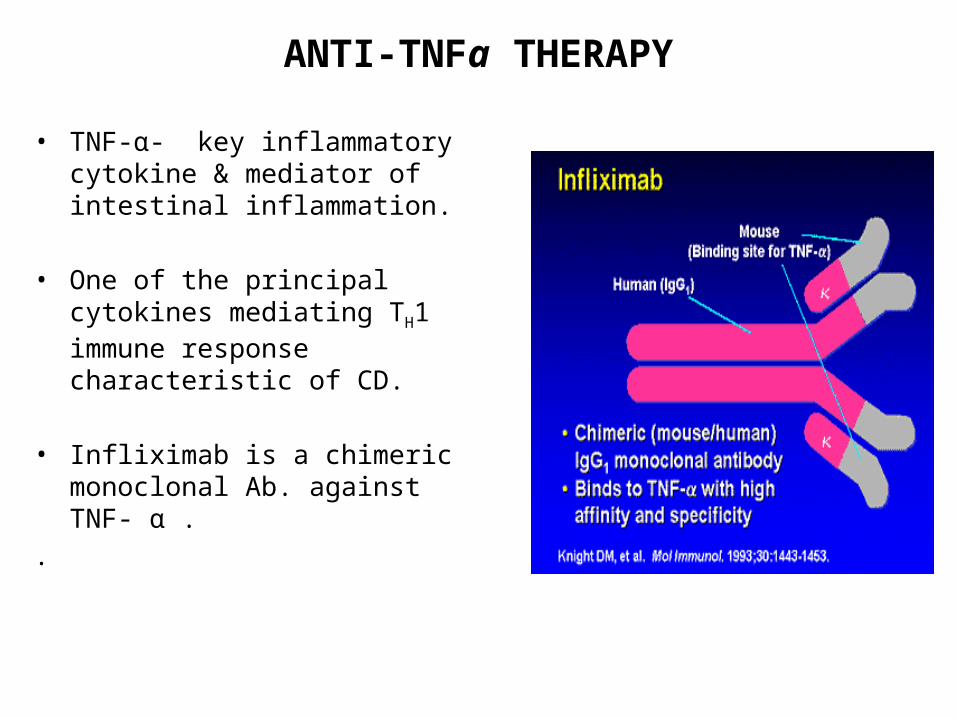
ANTI-TNFa THERAPY
• TNF-α- key inflammatory cytokine & mediator of intestinal inflammation.
• One of the principal cytokines mediating TH1 immune response characteristic of CD.
• Infliximab is a chimeric monoclonal
Ab. against TNF- α . .
USES & DOSAGE • Infliximab 5mg/kg infused I/V –0,2,6 wks interval
—decrease frequency of ac. flares in 2/3rd pts. with moderate –severe CD.
• Facilitates closing of enterocutaneous fistula- maintains remission & prevent recurrence
• Infliximab+Azathioprine-more effective in inducing remission & mucosal healing in steroid resistant patient.
• Also effective for refractory UC
SIDE EFFECTS• Acute:
– Fever– Chills– Urticaria– anaphylaxis
• Subacute: – serum sickness
• Resp. infections; potential reactivation of tuberculosis or other granulomatous infections with subsequent dissemination.
• Possible increased incidence of non-Hodgkin's lymphoma
• ADALIMUMAB Recombinant human monoclonal IgG1 Ab against TNFa Not used in infliximab unresponsive pts. DOSE- S/C 160,80,40mg at 0,2,4 wks respectively.
• CERTOLIZUMAB- • Pegylated Fab antibody to TNFα. DOSE- S/C 400mg at 0,2,4 wks interval.
NATALIZUMAB• Humanized monoclonal antibody against
a4 integrins• Binding of this antibody to integrins(adhesion
molecule) - reduce extravasation of certain leukocytes-prevents their migration to site of inflammation –reduces exacerbation of tissue injury.
USE & DOSAGE• Reintroduced in 2008 • Induction and maintenance of remission of
moderate to severe CD (who didn’t respond to other therapy)
• 300 mg every 4 wks by i/v infusion.
C/I• Interacts with other immunomodulators to
increase risk of PML –withdrawn earlier.
ANTIBIOTICS
• Commonly used Antibiotics–Metronidazole
–Ciprofloxacin
–Clarithromycin .
• USE– Adjunctive Tt. along with other medications for active IBD– Treatment of specific complications of CD– Metronidazole 20mg/kg/day
• Specific CD related complications that may benefit from antibiotic therapy include:– intra-abdominal abscess– inflammatory masses– perianal disease (including fistulas & perirectal abscesses)– small bowel bacterial overgrowth secondary to partial small bowel
obstruction– Secondary inf. with organisms such as C. difficile
PROBIOTICS
• Probiotics are a mixture of beneficial lyophilized bacteria given orally
• Several studies showed beneficial effects of probiotics in UC
• Utility as primary therapy remains unclear.
SUPPORTIVE THERAPY IN IBD
• Individualized based on symptoms• Supplementary to antinflammatory medication• Anticholinergic: (dicyclomine hydrochloride) are
used to reduce abdominal cramps, pain & rectal urgency
• Antidiarrheal agents: Loperamide can be used to reduce frequency of bowel movements & relieve rectal urgency in pts. with mild disease.
• Oral iron, folate & vitamin B12 adm. as indicated.
THANK YOU
• Genetic analyses of CD, mutations in a gene called nucleotide-binding oligomerization domain-2 (NOD2, also called CARD15) associated with both familial & sporadic CD.
• NOD2 is expressed in monocytes, granulocytes, dendritic cells, and intestinal epithelial cells
• It is proposed to function as an intracellular sensor for bacterial infection by recognizing peptidoglycans, thereby playing an important role in the natural immunity to bacterial pathogens.
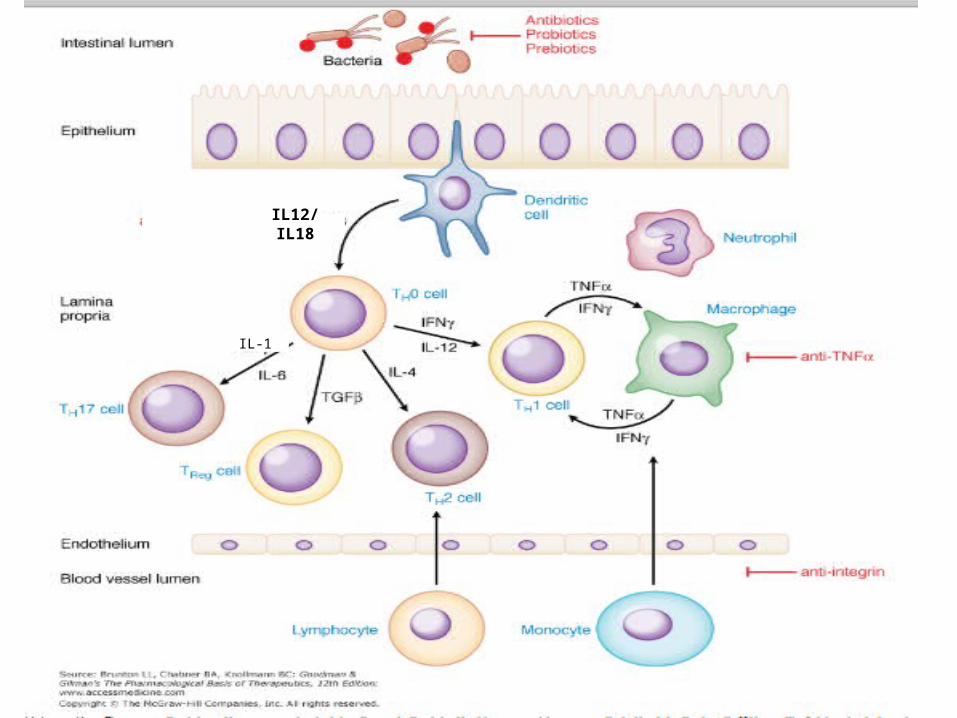
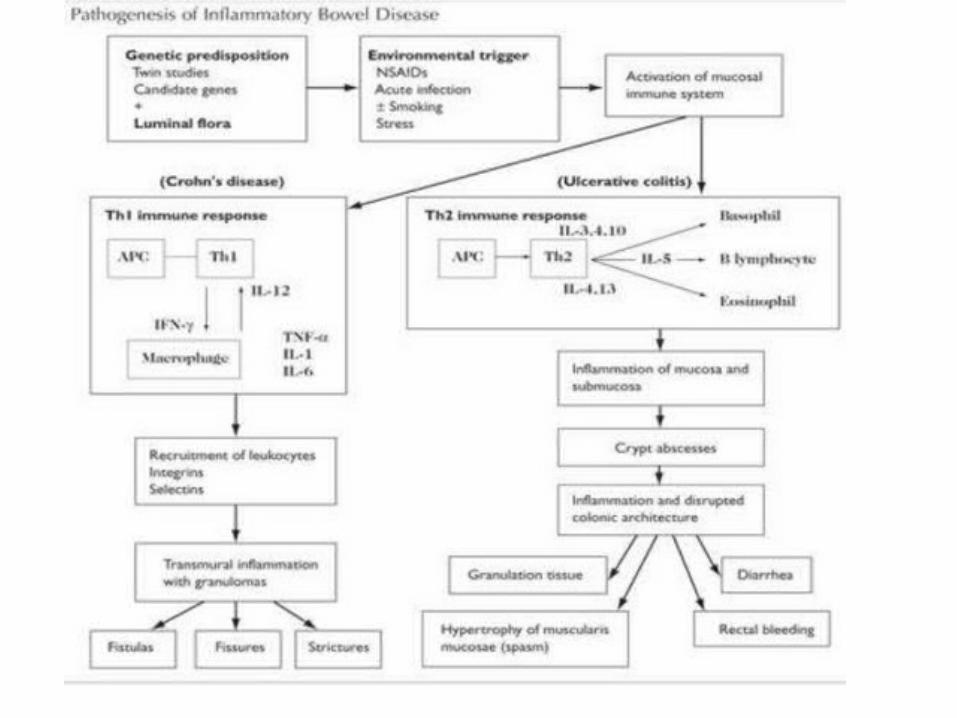
• In IBD there is imbalance between proinflammatory and anti inflammatory mediators.
• CD transmural lesions-lymphocytes and macrophages, granuloma formation ,submucosal fibrosis. cytokine profile -- increased IL-12, IFN-ϒ, & TNF- α, characteristic- T-helper 1 (TH1)-mediated inflammatory processes.
• UC superficial lesions-lymphocytic and neutrophilic
infiltrates.resembles more closely with that mediated by TH2 pathway.

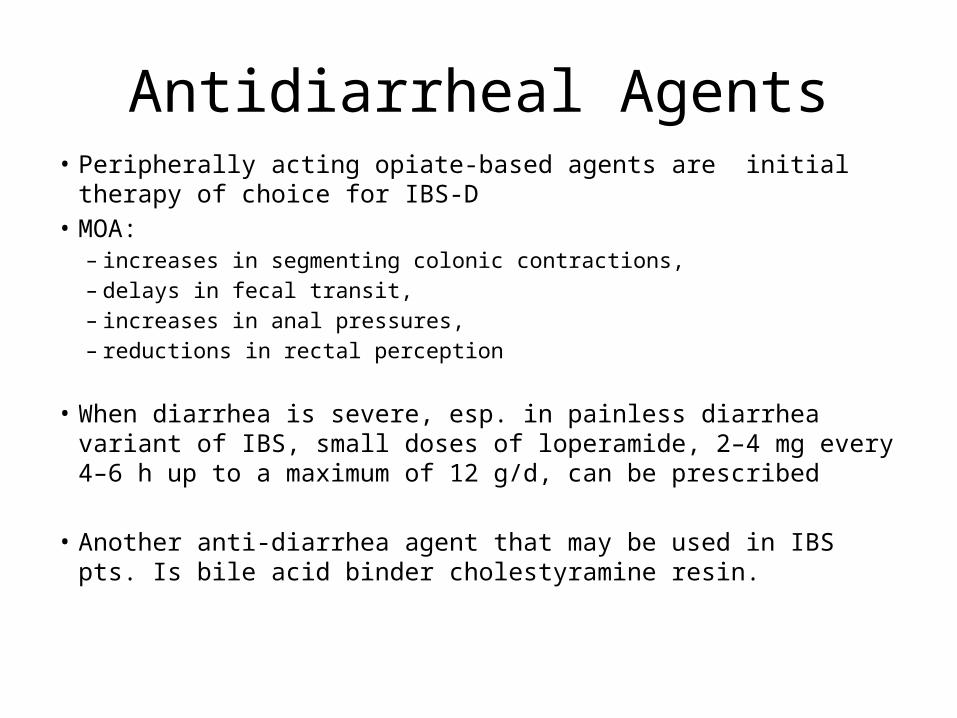
Antidiarrheal Agents• Peripherally acting opiate-based agents are initial therapy of choice for IBS-
D• MOA:
– increases in segmenting colonic contractions, – delays in fecal transit, – increases in anal pressures, – reductions in rectal perception
• When diarrhea is severe, esp. in painless diarrhea variant of IBS, small doses of loperamide, 2–4 mg every 4–6 h up to a maximum of 12 g/d, can be prescribed
• Another anti-diarrhea agent that may be used in IBS pts. Is bile acid binder cholestyramine resin.
COMPLICATIONS
• Severe diarrhoea with electrolyte imbalance• Massive hemorrhage• Severe colonic dilatation(toxic megacolon)• Perforation• Stricture of the colorectum• Malignancy
SIDE EFFECTS
• Renal function impairment• Hypertension• Gingival hyperplasia• Hypertrichosis• Paresthesias • Tremors• Electrolyte abnormalities • Opportunistic infections, most notably Pneumocystis
carinii pneumonia.
MOA: It blocks TNF- α in serum & at cell surface & lyses TNF- α producing macrophages & T cells through complement fixation & antibody-dependent cytotoxicity