Embed Size (px)
DESCRIPTION
Designed for UG Pathology teaching.
Citation preview

Inflammation
and Repair - 8
Dr.CSBR.Prasad, M.D.
v3-CSBRP-May-2012

Tissue renewal
Regeneration
and
Repair
v3-CSBRP-May-2012

Regeneration
Regeneration refers to the proliferation of
cells and tissues to replace lost structures
Whole organs and complex tissues rarely
regenerate after injury
Exceptions are liver, epithelia of GIT, Skin,
Hemopoietic tissue
Compensatory growth Vs Regeneration
v3-CSBRP-May-2012

Repair
Repair is a healing process
It’s a combination of regeneration and scar formation
v3-CSBRP-May-2012

Repair
Tissue repair depends on:
the ability of the tissue to
regenerate and
the extent of the injury
v3-CSBRP-May-2012

Repair
Chronic inflammation > growth factors and cytokines > Scar
FIBROSIS is used to describe the extensive deposition of collagen
v3-CSBRP-May-2012

Repair
ECM components are essential for wound healing: Provide the framework for cell migration
Facilitate Angiogenesis
Cells in the ECM produce growth factors
v3-CSBRP-May-2012

Repair
Although repair is a healing process,
it may cause tissue dysfunction
v3-CSBRP-May-2012

Repair
Examples:
• AS
• Healed MI
• Cirrhosis
• Contractures
• Corneal opacities
• Pulmonary fibrosis
• Bronchiectasis
• Intestinal strictures
• Adhesions after
surgery
• Ankylosis
• Cranial nerve palsies
after TB-meningitis
Although repair is a healing process, it may cause tissue dysfunction
v3-CSBRP-May-2012

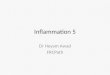
Cirrhosis of liver v3-CSBRP-May-2012

Pulmonary fibrosis v3-CSBRP-May-2012

v3-CSBRP-May-2012

v3-CSBRP-May-2012

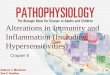
Basal Meningitis - TB v3-CSBRP-May-2012

6th left cranial nerve plasy v3-CSBRP-May-2012

v3-CSBRP-May-2012

v3-CSBRP-May-2012

v3-CSBRP-May-2012

v3-CSBRP-May-2012

Ocular Herpes v3-CSBRP-May-2012

v3-CSBRP-May-2012

Understanding the mechanisms of regeneration
and repair requires:
•knowledge of the control of cell proliferation
•signal transduction pathways, and
•functions of ECM components
v3-CSBRP-May-2012

Principles of cell proliferation
Control of Normal Cell Proliferation and
Tissue Growth
• In adult tissues the size of cell
populations is determined by the rates
of cell proliferation, differentiation, and
death by apoptosis
• Cell proliferation can be stimulated by
physiologic and pathologic conditions
v3-CSBRP-May-2012

Principles of cell proliferation
Physiological:
EM to Estrogen
Thyroid to TSH,
pregnancy
Pathological:
• NPH to
dihydrotestosterone
• Nodular goitres to
TSH
Control of Normal Cell Proliferation and Tissue Growth
Cell proliferation can be stimulated by physiologic
and pathologic conditions
v3-CSBRP-May-2012

Why thyroid enlarges in
pregnancy?
α-chain of HCG is identical to
the α-chain of TSH
v3-CSBRP-May-2012

Principles of cell proliferation
Cell proliferation is largely controlled by signals
(soluble or contact-dependent) from the
microenvironment that either stimulate or inhibit
proliferation
An excess of stimulators or a deficiency of
inhibitors leads to net growth and, in the case of
cancer, uncontrolled growth
v3-CSBRP-May-2012

TISSUE PROLIFERATIVE
ACTIVITY
The tissues of the body are divided into
three groups on the basis of the
proliferative activity of their cells:
1. Continuously dividing (labile tissues)
2. Quiescent (stable tissues) and
3. Nondividing (permanent tissues)
v3-CSBRP-May-2012

TISSUE PROLIFERATIVE ACTIVITY
1. Continuously dividing (labile tissues)
Cells proliferate throughout life, replacing those that are destroyed
Examples include:
Surface epithelia, such as stratified squamous epithelia of the skin, oral cavity, vagina, and cervix; the lining mucosa of all the excretory ducts of the glands of the body (e.g., salivary glands, pancreas, biliary tract)
The columnar epithelium of the GI tract and uterus; the transitional epithelium of the urinary tract
Cells of the bone marrow and hematopoietic tissues
In most of these tissues mature cells are derived from adult stem cells, which have a tremendous capacity to proliferate
v3-CSBRP-May-2012

TISSUE PROLIFERATIVE ACTIVITY
1. Continuously dividing (labile tissues)
2. Quiescent (stable tissues)
Have a low level of replication
Can undergo rapid division in response to stimuli
Examples:
Parenchymal cells of liver, kidneys, and pancreas
Mesenchymal cells such as fibroblasts and smooth muscle
Vascular endothelial cells and
Lymphocytes and other leukocytes v3-CSBRP-May-2012

TISSUE PROLIFERATIVE ACTIVITY
1. Continuously dividing (labile tissues)
2. Quiescent (stable tissues)
3. Nondividing (permanent tissues)
Cells that have left the cell cycle
Cannot undergo mitotic division
Examples:
• Neurons
• Skeletal and
• Cardiac muscle cells
Gliosis
Cardiac muscle has very limited regenerative capacity v3-CSBRP-May-2012

v3-CSBRP-May-2012

v3-CSBRP-May-2012
Role of the extracellular
matrix in regeneration
and repair:
Liver regeneration with
restoration of normal
tissue after injury requires
an intact cellular matrix. If
the matrix is damaged the
injury is repaired by
fibrous tissue deposition
and scar formation

STEM CELLS
• Stem cells are characterized by their self-
renewal properties and by their capacity to
generate differentiated cell lineages
v3-CSBRP-May-2012

Stem cells
Maintainance of stem cells is achieved by two mechanisms:
1. Obligatory asymmetric replication
with each cell division, one of the daughter cells retains its self-renewing capacity while the other enters a differentiation pathway
2. Stochastic differentiation:
cell division may generate either two self-renewing stem cells or two cells that will differentiate
v3-CSBRP-May-2012

v3-CSBRP-May-2012

Terms
o Pluripotent stem cells: can generate all tissues of the body
o Multipotent stem cells: which have more restricted developmental potential, and eventually produce differentiated cells from the three embryonic layers
o Transdifferentiation: indicates a change in the lineage commitment of a stem cell
o Adult stem cells or somatic stem cells: have a more restricted capacity to generate different cell types have been identified in many tissues
o Induced pluripotent stem cells: differentiated cells of humans can be reprogrammed into pluripotent cells, similar to ES cells, by the transduction of genes encoding ES cell transcription factor
v3-CSBRP-May-2012

v3-CSBRP-May-2012

Reprogramming of Differentiated Cells:
Induced Pluripotent Stem Cells
• Transfer the nucleus to an enucleated oocyte.
• The oocytes implanted into a surrogate mother
• This can generate cloned embryos that develop into complete animals
• This procedure, known as reproductive cloning,
• therapeutic cloning:In this technique the nucleus of a skin fibroblast from a patient is introduced into an enucleated human oocyte to generate ES cells, which are kept in culture, and then induced to differentiate into various cell types.
• These cells are inefficient and often inaccurate. One of the main reasons for the inaccuracy is the deficiency in histone methylation in reprogrammed ES cells, which results in improper gene expression.
v3-CSBRP-May-2012

v3-CSBRP-May-2012

LIVER REGENERATION
Hepatocyte proliferation in the regenerating
liver is triggered by the combined actions of
cytokines and polypeptide growth factors
– Priming phase – TNF, IL-6 & C – system
– DNA synthesis – HGF, TGFα, and HB-EGF
– Adjuvants - Norepinephrine, serotonin, insulin,
thyroxin and growth hormone
v3-CSBRP-May-2012

• Individual hepatocytes replicate once or twice during regeneration and then return to quiescence
• Growth inhibitors, such as TGF-β and activins, may be involved in terminating hepatocyte replication
• Intrahepatic stem or progenitor cells do not play a role in the compensatory growth that occurs after partial hepatectomy
• Endothelial cells and other nonparenchymal cells in the regenerating liver may originate from bone marrow precursors
v3-CSBRP-May-2012

v3-CSBRP-May-2012

Extracellular Matrix and
Cell-Matrix Interactions
Tissue repair and regeneration depends on:
• Cytokines
• Interactions between cells & ECM
The ECM regulates the growth, proliferation,
movement, and differentiation of the cells
living within it
v3-CSBRP-May-2012

ECM - various functions
• Mechanical support
• Control of cell growth
• Maintenance of cell differentiation
• Scaffolding for tissue renewal
• Establishment of tissue
microenvironments
• Storage and presentation of regulatory
molecules
v3-CSBRP-May-2012

ECM - Composition
The ECM is composed of three groups of
macromolecules:
Fibrous structural proteins - provide tensile
strength
Adhesive glycoproteins: connect the
matrix elements to one another and to
cells
Proteoglycans and hyaluronan - resilience
v3-CSBRP-May-2012

Mechanisms by which ECM components and growth
factors interact and activate signaling pathways
v3-CSBRP-May-2012

Angiogenesis by mobilization of endothelial precursor
cells (EPCs) from the bone marrow and from
preexisting vessels (capillary growth)
v3-CSBRP-May-2012

Main components of the
extracellular matrix (ECM)
v3-CSBRP-May-2012

Healing by Repair,
Scar Formation and Fibrosis
v3-CSBRP-May-2012

Healing by Repair,
Scar Formation and Fibrosis
Repair occurs by fibrosis & scar formation
when:
• There is loss of parenchyma & frame work
Here lost tissue will be replaced by collagen
v3-CSBRP-May-2012

Repair by connective tissue deposition
includes the following basic features:
• Inflammation
• Angiogenesis
• Migration and proliferation of fibroblasts
• Scar formation
• Connective tissue remodeling
v3-CSBRP-May-2012

Angiogenesis
During embryonic development:
Vasculogenesis:
• Angioblasts
• Hemangioblasts
In adults:
Angiogenesis or Neovascularization
• Endothelium of adjacent pre-existing vessels
• BM endothelial progenitor cells (EPCs) v3-CSBRP-May-2012

Angiogenesis
Angiogenesis from Preexisting Vessels:
• Vasodilation
• Degradation of the BM
• Migration of endothelial cells
• Proliferation of endothelial cells
• Maturation of endothelial cells
• Recruitment of periendothelial cells
v3-CSBRP-May-2012

Angiogenesis
Angiogenesis from Endothelial Precursor Cells (EPCs):
• EPCs can be recruited from the bone marrow
• The number of circulating EPCs increases greatly in patients with ischemic conditions
• Examples:
– Re-endothelization of vascular implants
– Neovascularization of ischemic organs
– Neovascularization of cutaneous wounds
– Neovascularization of tumors v3-CSBRP-May-2012

Angiogenesis
Growth Factors and Receptors Involved in Angiogenesis
VEGF is the most important growth factor in adult tissues
Newly formed vessels are fragile and need to become “stabilized” – Pericytes
– Smooth muscle cells
Factors that participate in the stabilization process: – Angiopoietins 1 and 2
– PDGF, and
– TGF-β
v3-CSBRP-May-2012

E N D
v3-CSBRP-May-2012

v3-CSBRP-May-2012