Embed Size (px)
Citation preview
Improve EPSDT Service Quality Through Meaningful Use of HIT
Xiaohui Zhang, Ph.D., Chief Scientist & Technology Strategist, STCMark Shishida, Executive Vice President, Cognosante
Seonho Kim, Chief Architect, ApeniMed, Inc.
Presented at:
Medicaid Enterprise Systems Conference 2012, Boston, MA
This white paper contains data that shall not be duplicated, used, or disclosed in whole or in part without the express permission of Cognosante. Copyright© 2012.

Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
Contents
WHO WE ARE AND WHAT WE DO..............................................................................................................1
HIGHLIGHT OF THE PRESENTATION............................................................................................................1
EPSDT – THE PEDIATRIC COMPONENT IN MEDICAID..............................................................................1
HEALTH CARE BENEFITS.................................................................................................................................2
STATE ADMINISTRATIVE SUPPORT SERVICES....................................................................................................2
CHALLENGES IN EPSDT MANAGEMENT AND DATA MONITORING..........................................................2
EPSDT DENTAL PERIODICITY SCHEDULES BY STATES – SOME STILL NOT AVAILABLE......................................3
SUMMARY OF MEDICAID ENROLLMENT CHANGE 2000 – 2011.........................................................................4
2011: MEDICAID AND CHIP ENROLLMENT CHILDREN IS ABOUT 83% OF TOTAL MEDICAID ENROLLMENT......5
CURRENT EPSDT DATA MONITORING AND CHALLENGES.......................................................................6
AN ILLUSTRATION OF CURRENT EPSDT DATA MONITORING BY ANNUAL REPORT FORM-416...............................7
DISCONNECTIONS IN THE CURRENT MEASUREMENTS...............................................................................7
A CLOSE LOOK AT THE LATEST NATIONAL EPSDT REPORT DATA......................................1
SUPPORT EPSDT IN ERA OF MEANINGFUL USE OF HIT.............................................................6
SOME QUESTIONS WE HAVE BEEN ASKING...............................................................................................1
LEVERAGE THE MU OF HIT AND CHIPRA AND OTHER INITIATIVES.....................................................2
EXAMPLE OF LEVERAGE HEALTHDATA.GOV FOR (MEASURE-3) PERCENTAGE OF LIVE BIRTH WEIGHTING LESS THAN 2500 GRAMS....................................................................................................................................3
EASY TO QUERY, EXPORT DATA AND BETTER SUPPORT MEDICAID MANAGEMENT...........................................4
EXAMPLE – CHILDHOOD IMMUNIZATION STATUS (MEASURE 5)..............................................................4
EXAMPLE : CHILDHOOD IMMUNIZATION STATUS REPORT.......................................................................5
THE CONCLUSION AND DISCUSSIONS..........................................................................................................7
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
ii
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
WHO WE ARE AND WHAT WE DO
Scientific Technologies Corp. (STC)
Leading PH IT solutions in 24 years, supporting 16 states immunization registries with 700+ HL7 links, 17,000+ providers, 24 M patients
STC has supported disease surveillance in 10 states, NYC and WDC
Cognosante
Healthcare IT company serving more than 40 Medicaid, EPSDT and CHIP programs for over 25 years
Expert in Health Information Exchange, assisting ONC with CONNECT architecture & standards
ApeniMED
Provides clinical networking interoperability solutions
An industry-leader in HIE and federal agency connectivity using the NwHIN
HIGHLIGHT OF THE PRESENTATION
Introduction to EPSDT and a snapshot of its beneficiaries
Current EPSDT service and quality monitoring
The major challenges and the gaps
Better support EPSDT with the initiatives in MU of HIT
The historical opportunity for EPSDT in ARRA/HITECH with EMRs, EDRs, PHRs and HIE efforts
“Healthdata.gov “and initiatives
Improve EPSDT delivery through leveraging the Core Set of Children’s Healthcare Quality Measures
Examples of integrated EPSDT management tool in new quality measures
EPSDT – THE PEDIATRIC COMPONENT IN MEDICAID
The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit provides comprehensive and preventive health care services for children under age 21 who are enrolled in Medicaid. A legal standard of coverage and access for low-income children
EPSDT has remained a central component of Medicaid, because of the operational and financial capacity it gives states to create appropriate pediatric health care systems (its ability to finance early, preventive, and on going healthcare for children at medical and social risk remains unparalleled in public or private health insurance).
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
1

Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
Health Care Benefits
Periodic assessments of children’s growth and development in accordance with accepted pediatric assessment standards, including:
Unclothed physical exam incuding a nutritional assessment; An assessment to determine a child’s overall physical, mental, and developmental health (the
developmental assessment); Health history; Laboratory services as needed, including assessment of blood lead levels; Immunizations in accordance with the recommendations of the Advisory Committee on the
Immunization Practices; and Anticipatory guidance.
Interperiodic (as needed) assessments.
Comprehensive vision, dental, and hearing services in accordance with reasonable professional standards.
All medically necessary dagnostic and treatment items and services that fall within the definition of medical assistance.
A preventive standard of medical necessity that specifies “early” coverage to “correct or ameliorate” physical and mental conditions in children.
Coordination with related programs.
State Administrative Support Services
Information about EPSDT and the value of preventive health care.
Provision of scheduling and transportation to families who request services in order to ensure the timely provision of care.
Provision of reports to the United States Department of Health and Human Services regarding the number of children referred for corrective treatment, and the state’s results in attaining federally set participation goals.
—From EPSDT at 40 by CHCS
CHALLENGES IN EPSDT MANAGEMENT AND DATA MONITORING
State varying well-child visiting periodicity schedules and the visit documentation forms
Most states follow AAP Bright Future for age groups in 0-11 months, 1-4 years, 5-10 years old
Age 12-21 years old
36 states require annual preventive visit
12 states require a visit every two years
One state requires a visit every four years
States use different forms
State varying separated dental visiting periodicity schedules
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
2
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
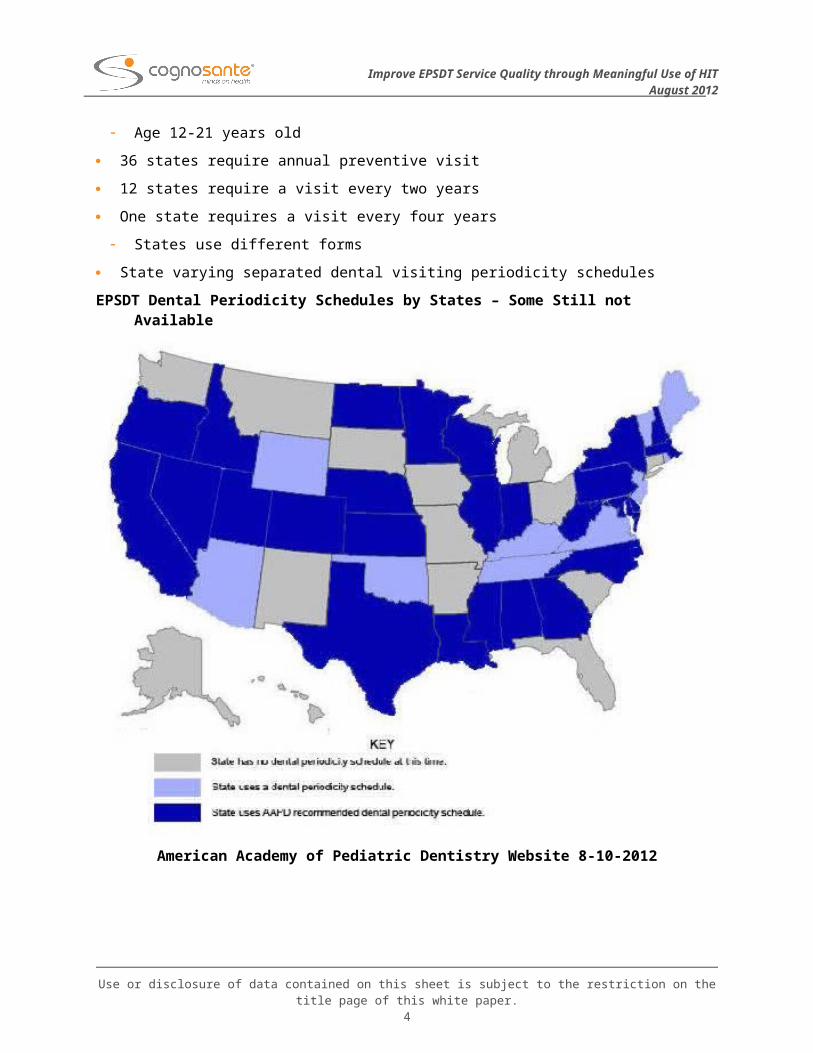
EPSDT Dental Periodicity Schedules by States – Some Still not Available
American Academy of Pediatric Dentistry Website 8-10-2012
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
3
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
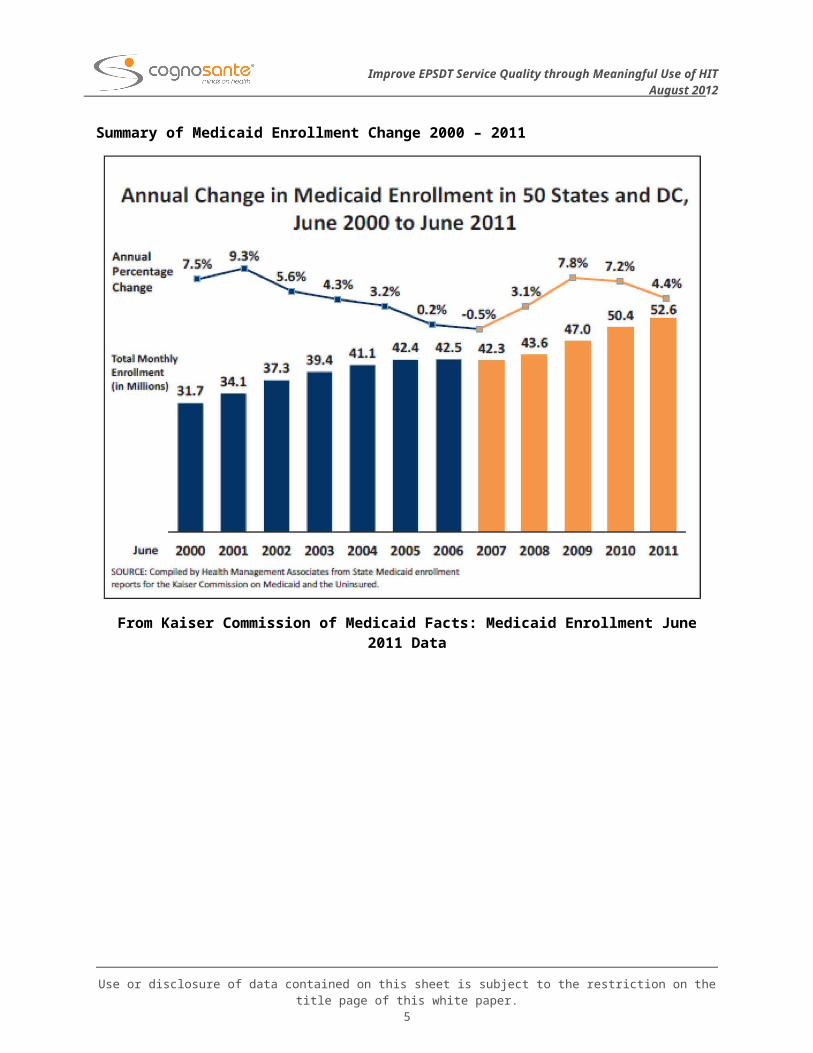
Summary of Medicaid Enrollment Change 2000 – 2011
From Kaiser Commission of Medicaid Facts: Medicaid Enrollment June 2011 Data
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
4
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
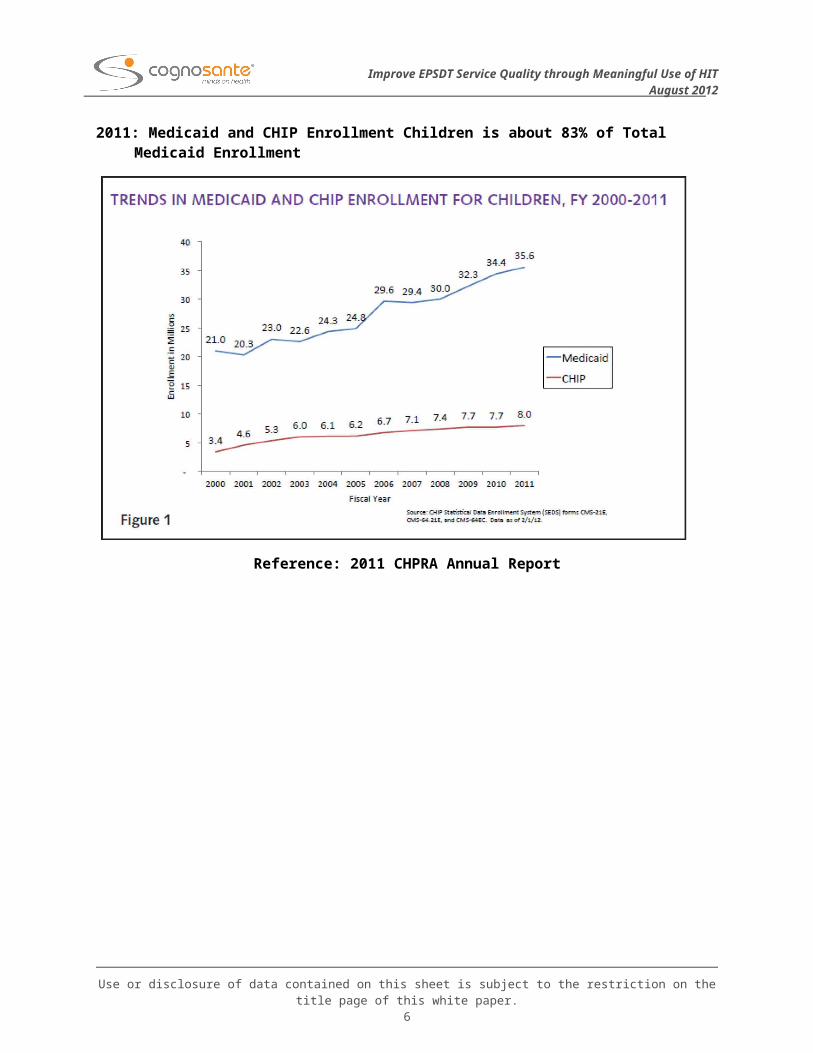
2011: Medicaid and CHIP Enrollment Children is about 83% of Total Medicaid Enrollment
Reference: 2011 CHPRA Annual Report
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
5
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
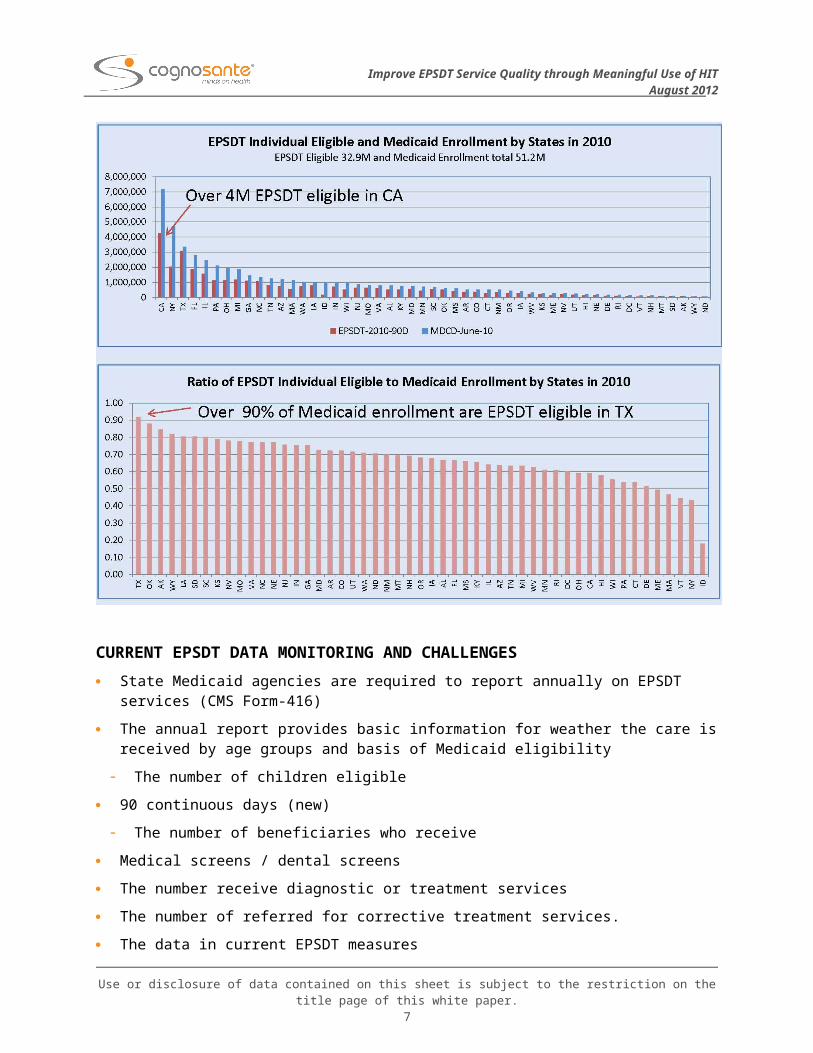
CURRENT EPSDT DATA MONITORING AND CHALLENGES
State Medicaid agencies are required to report annually on EPSDT services (CMS Form-416)
The annual report provides basic information for weather the care is received by age groups and basis of Medicaid eligibility
The number of children eligible
90 continuous days (new)
The number of beneficiaries who receive
Medical screens / dental screens
The number receive diagnostic or treatment services
The number of referred for corrective treatment services.
The data in current EPSDT measures
Claim based
Paper based
Participant ratio and screen ratio
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
6
Improve EPSDT Service Quality through Meaningful Use of HITAugust 2012
Little about the content of care
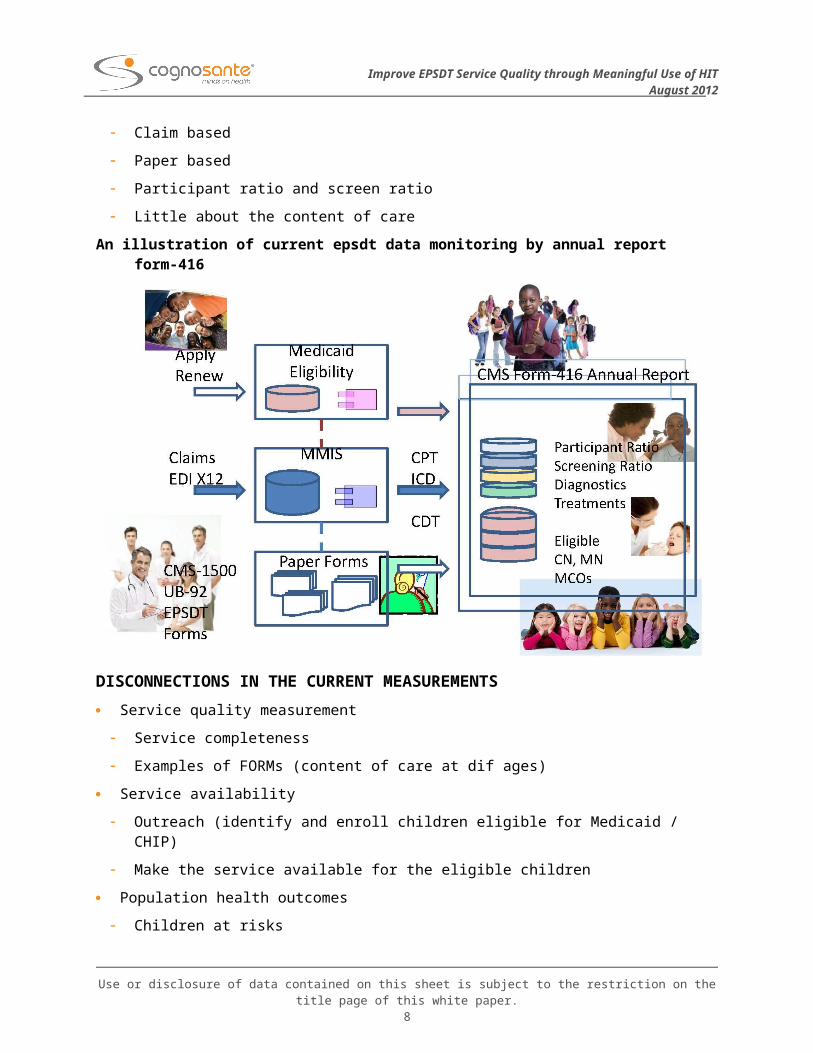
An illustration of current epsdt data monitoring by annual report form-416
DISCONNECTIONS IN THE CURRENT MEASUREMENTS
Service quality measurement
Service completeness
Examples of FORMs (content of care at dif ages)
Service availability
Outreach (identify and enroll children eligible for Medicaid / CHIP)
Make the service available for the eligible children
Population health outcomes
Children at risks
Chronic conditions
Mental health issues
Referrals and follow up treatment
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
7
Improve EPSDT Service Quality through Meaningful Use of HITDate
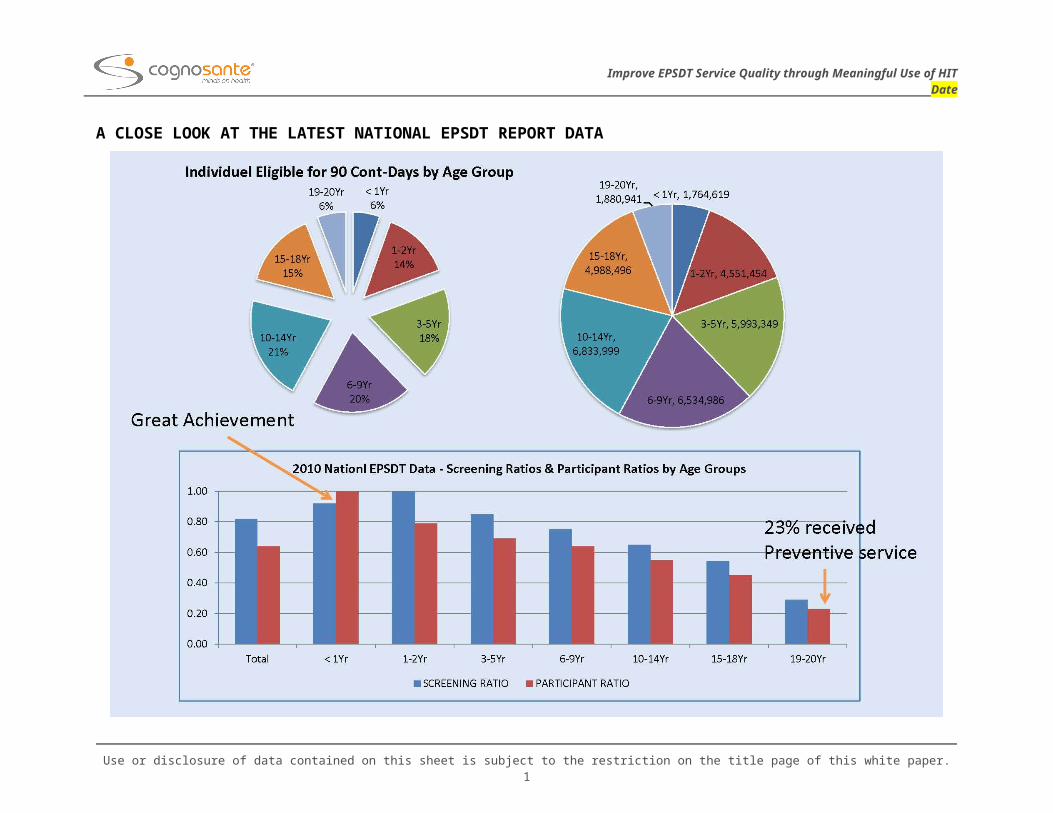
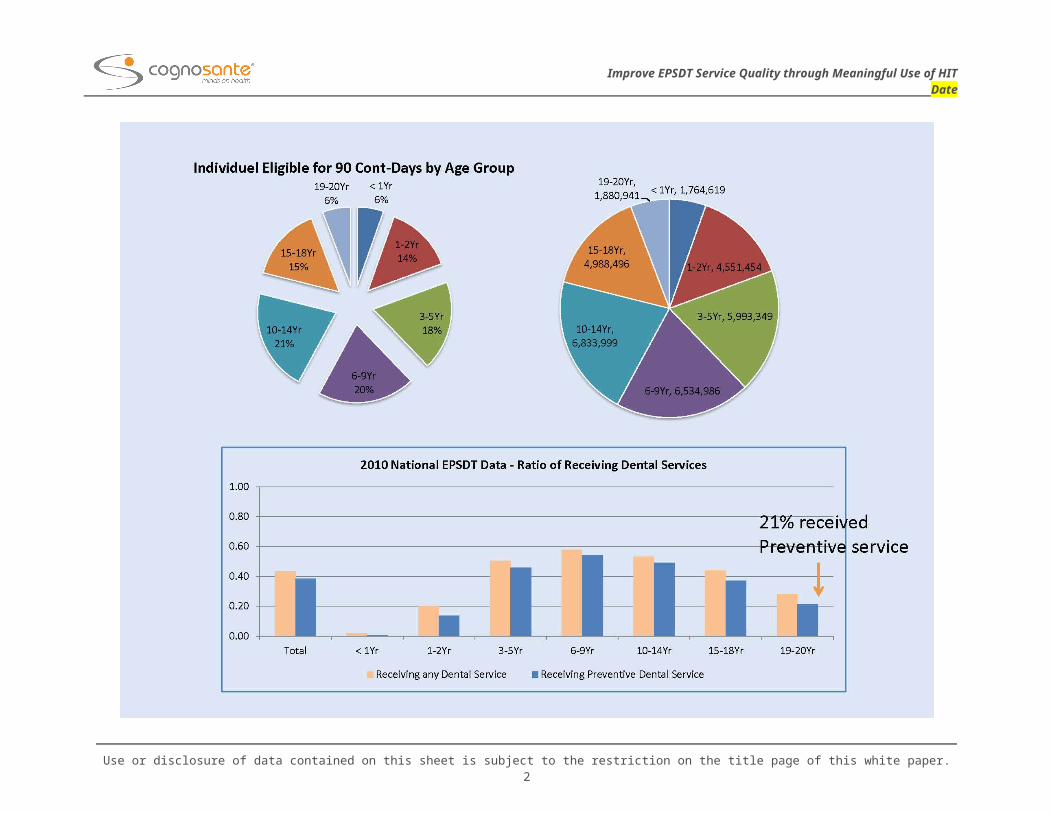
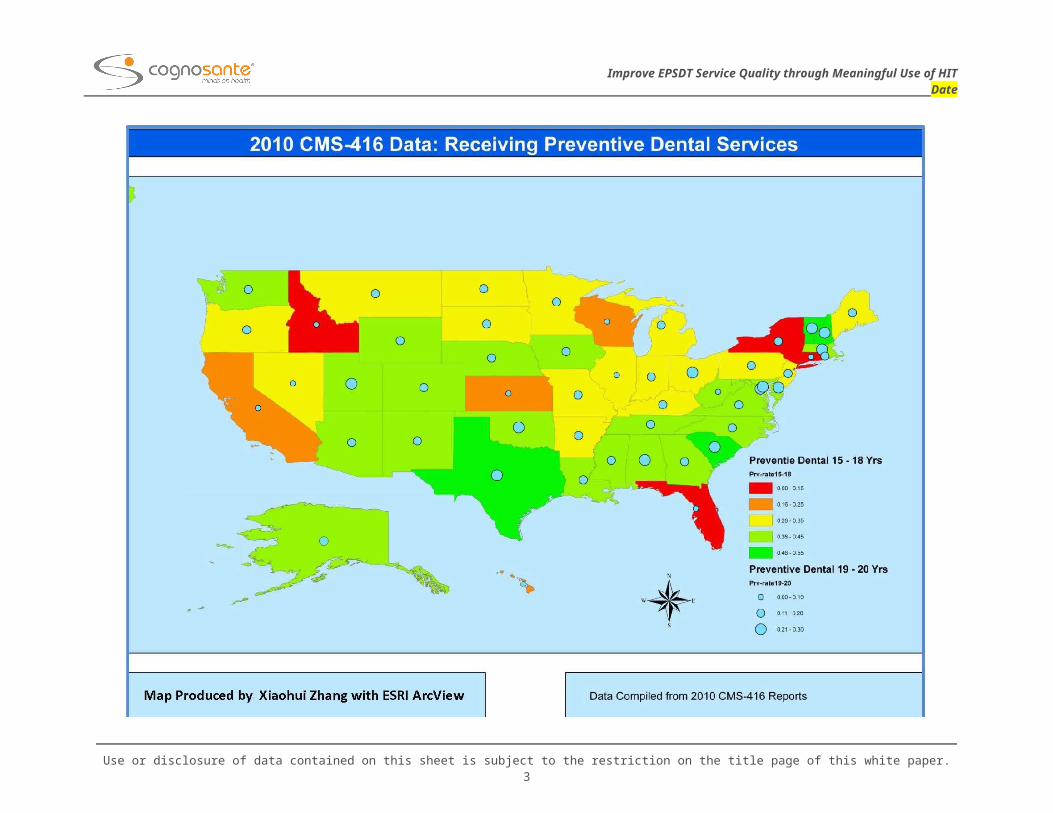
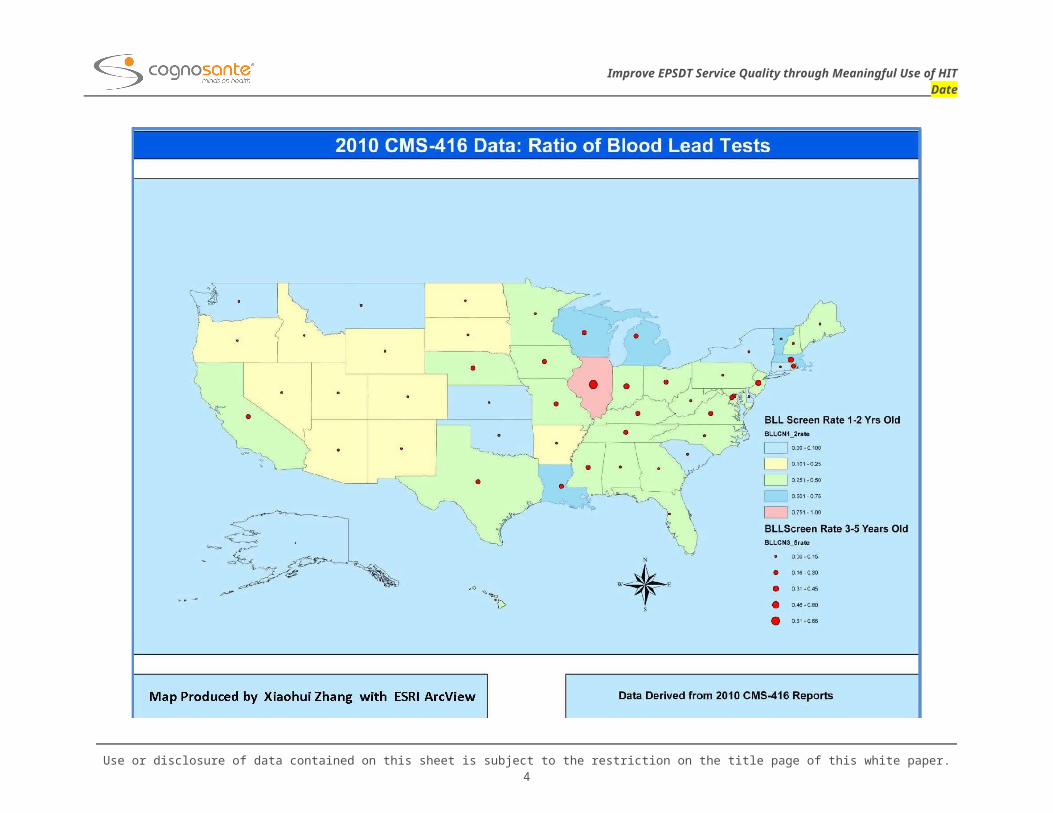
A CLOSE LOOK AT THE LATEST NATIONAL EPSDT REPORT DATA
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.1

Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.2
Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.3
Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.4
Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.5
Improve EPSDT Service Quality through Meaningful Use of HITDate
SUPPORT EPSDT IN ERA OF MEANINGFUL USE OF HIT
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.6
Improve EPSDT Service Quality through Meaningful Use of HITDate
SOME QUESTIONS WE HAVE BEEN ASKING
How to improve the EPSDT service quality
Improve the service availability, accessibility and service quality
Improve the EPSDT management efficiency and lower the cost (such as the coordinated integrated eligibility and enrollment systems for Medicaid, CHIP and HIX)
How to help providers improve performance
Improve the service efficiency by leveraging e-data and HIE, such as EMR data and EDR data
Improve the service completeness by clinical support systems with EPSDT workflow
How to improve the Medicaid children health outcomes through the new initiatives
How to leverage the chart review data captured in EPSDT visiting to Identify the population health issues
How to better support the early preventive healthcare
How to construct the coordinated and integrated EPSDT service systems by leveraging the new initiatives
Better support the continuous care through the HIE effort
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
1
Improve EPSDT Service Quality through Meaningful Use of HITDate
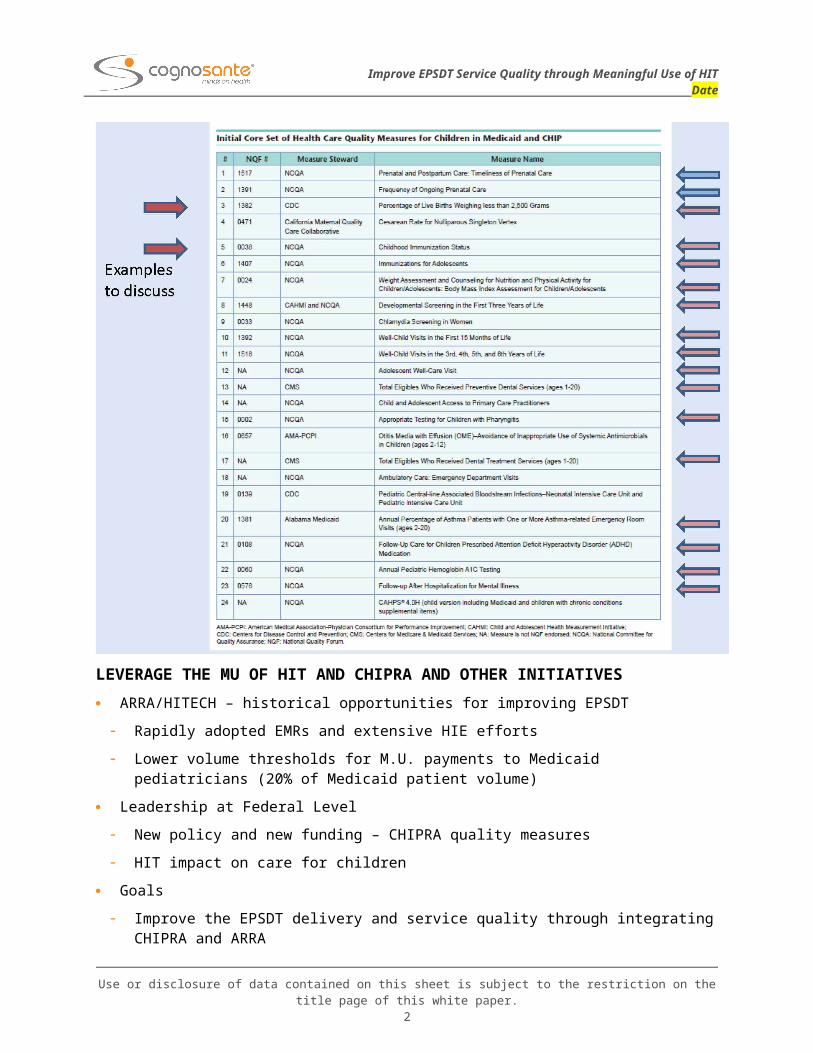
LEVERAGE THE MU OF HIT AND CHIPRA AND OTHER INITIATIVES
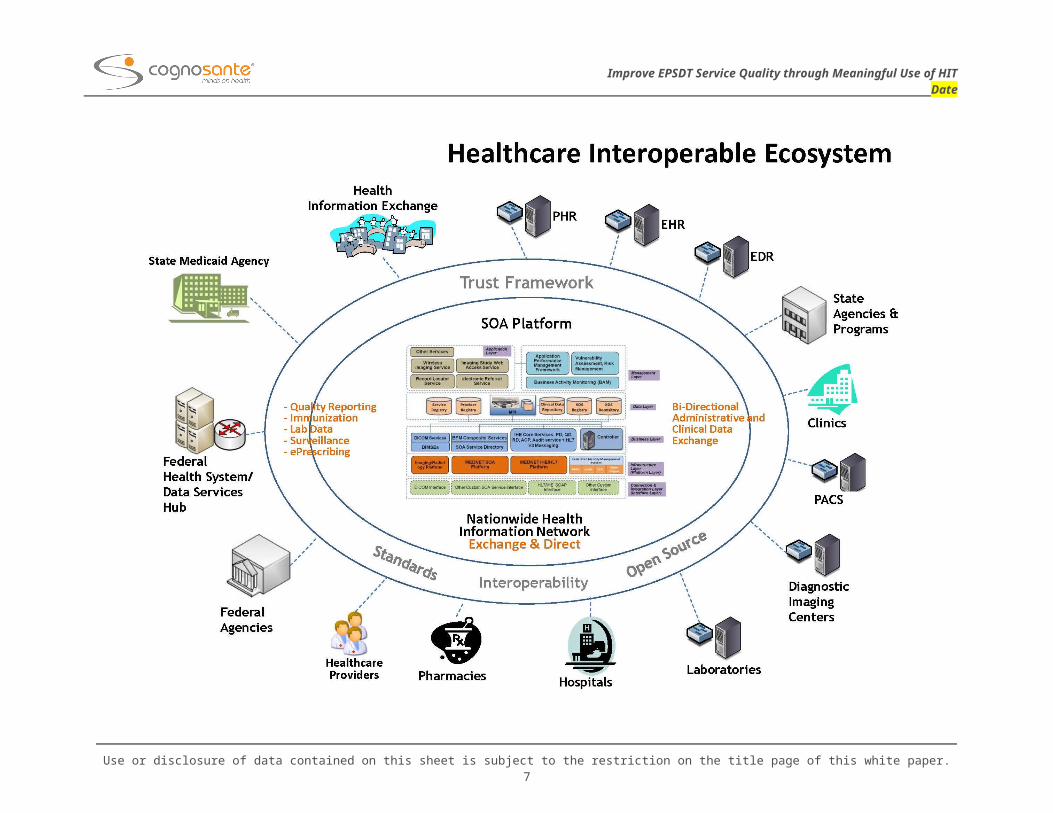
ARRA/HITECH – historical opportunities for improving EPSDT
Rapidly adopted EMRs and extensive HIE efforts
Lower volume thresholds for M.U. payments to Medicaid pediatricians (20% of Medicaid patient volume)
Leadership at Federal Level
New policy and new funding – CHIPRA quality measures
HIT impact on care for children
Goals
Improve the EPSDT delivery and service quality through integrating CHIPRA and ARRA
Improve the Medicaid children health outcomes
Selected Examples with Illustrated Approaches
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
2
Improve EPSDT Service Quality through Meaningful Use of HITDate
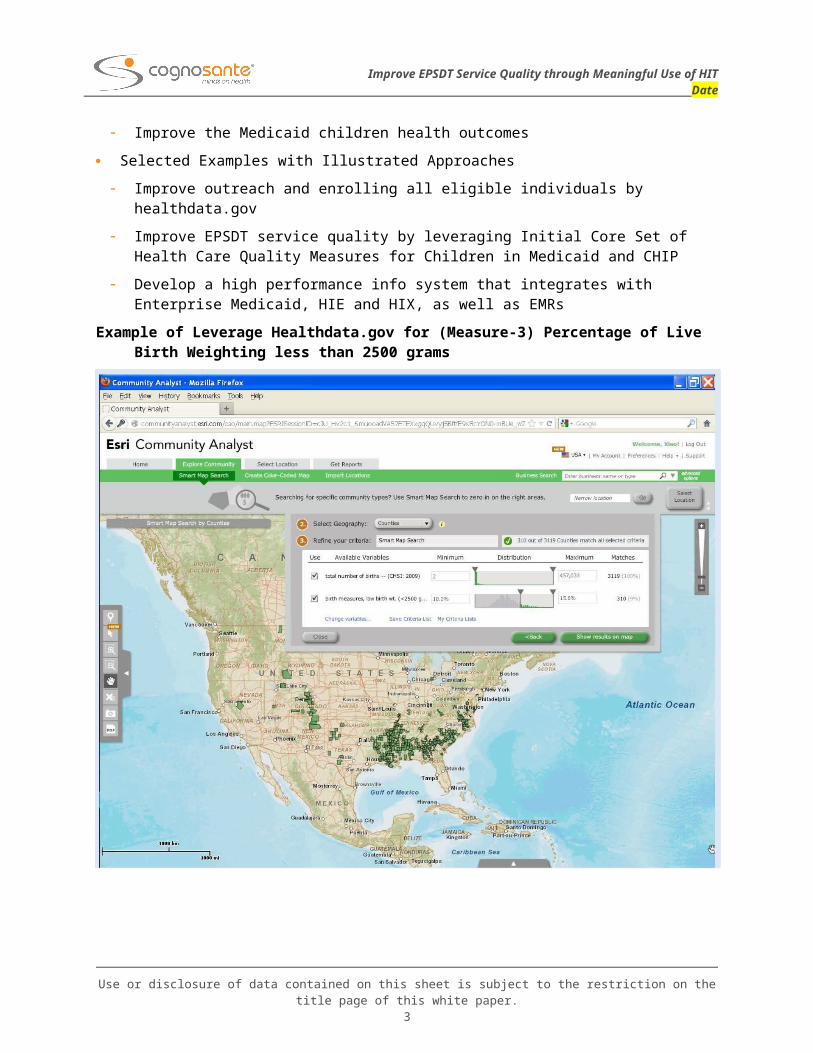
Improve outreach and enrolling all eligible individuals by healthdata.gov
Improve EPSDT service quality by leveraging Initial Core Set of Health Care Quality Measures for Children in Medicaid and CHIP
Develop a high performance info system that integrates with Enterprise Medicaid, HIE and HIX, as well as EMRs
Example of Leverage Healthdata.gov for (Measure-3) Percentage of Live Birth Weighting less than 2500 grams
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
3
Improve EPSDT Service Quality through Meaningful Use of HITDate
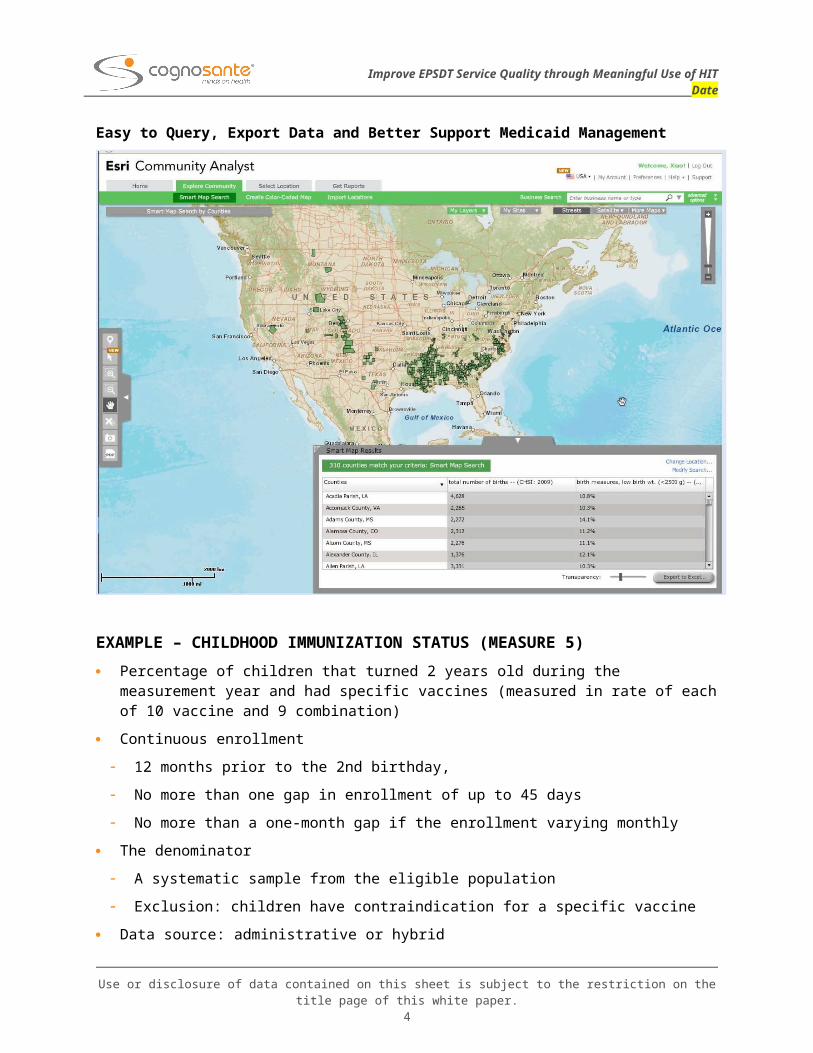
Easy to Query, Export Data and Better Support Medicaid Management
EXAMPLE – CHILDHOOD IMMUNIZATION STATUS (MEASURE 5)
Percentage of children that turned 2 years old during the measurement year and had specific vaccines (measured in rate of each of 10 vaccine and 9 combination)
Continuous enrollment
12 months prior to the 2nd birthday,
No more than one gap in enrollment of up to 45 days
No more than a one-month gap if the enrollment varying monthly
The denominator
A systematic sample from the eligible population
Exclusion: children have contraindication for a specific vaccine
Data source: administrative or hybrid
EXAMPLE : CHILDHOOD IMMUNIZATION STATUS REPORT
(Core Set Measure-5)
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
4
Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
5
Improve EPSDT Service Quality through Meaningful Use of HITDate
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
6
Improve EPSDT Service Quality through Meaningful Use of HITDate
THE CONCLUSION AND DISCUSSIONS
EPSDT has maintained as a central component in Medicaid
The initiatives in MU of HIT and CHIPRA quality measures have provided tremendous opportunities for improving EPSDT delivery and service quality
EPSDT should take advantage of rapidly adopted EMRs and HIE effort
Develop EPSDT module in pediatric EMRs
Improve patient safety
Advance the standards of care
Integrate EPSDT with HIE to support care coordination
Share the data among pediatricians, PCP and dentists
An integrated EPSDT information system in the state Medicaid management could help
Outreach the eligible children to enroll EPSDT and receive the services
Identify the Medicaid children population health risk early
Better capture the provided care data and improve the quality
providers improve performance
In memory of Barbara Bridgewater for her passion, insight, courage and dedication to the Medicaid industry.
Barbara was the coauthor of the original abstract for this presentation.
Thank You and Contact Information : Xiaohui Zhang, Ph.D., Chief Scientist & Technology Strategist, STC [email protected] Mark Shishida, Executive Vice President, Cognosante Seonho Kim, Chief Architect, ApeniMed, Inc.,
Use or disclosure of data contained on this sheet is subject to the restriction on the title page of this white paper.
7