Embed Size (px)
Citation preview

CBI CONFERENCE:RISK-BASED MONITORING FOR SMALL TO MID-SIZE
COMPANIES
Impact of Risk-Based Monitoring and eSource Methodologies on Clinical Sites, Patients,
Regulators and Sponsors
March 2015
For information contact:
Jules T. Mitchel, MBA, PhD
212-681-2100
© Copyright Target Health 2015
A Touch of Philosophy
“Life is really simple, but we insist on
making it complicated” Confucius
“Simplicity is the ultimate sophistication”Leonardo da Vinci
“The art of being wise is the art of
knowing what to overlook” William James
2
More Philosophy
Every truth passes through three stages before it is recognized:
In the first it is ridiculed
In the second it is opposed
In the third it is regarded as self-evident
(Arthur Schopenhauer)
3
There is No Substitute for Doing
What a person hears he/she may doubt
What he/she sees, he/she may possibly doubt
But what he/she does, cannot be doubted
(Adapted from Seaman Knapp: American Agriculturist and Educator)
Target Health Inc.
1. Industry leader in software supporting the paperless
clinical trial
2. Private, New York City-based, full-service eCRO
3. Total Drug and Device Development, including:
• Regulatory Affairs
• Strategic Planning
• Clinical Research
• Data Management
• Biostatistics
• Medical Writing
5
CTTI
Briggs W Morrison, Pfizer; Chrissy J Cochran, Division of
Bioresearch Monitoring, FDA; Jennifer Giangrande White,
Roche; Joan Harley, Training Extension/Pastor Consulting;
Cynthia F Kleppinger; Division of Scientific Investigation,
FDA; An Liu, Alquest; Jules T Mitchel, Target Health; David F
Nickerson, Pfizer; Cynthia R Zacharias, BMS; Judith M Kramer
Duke Translational Medicine Institute; and James D Neaton,
University of Minnesota6
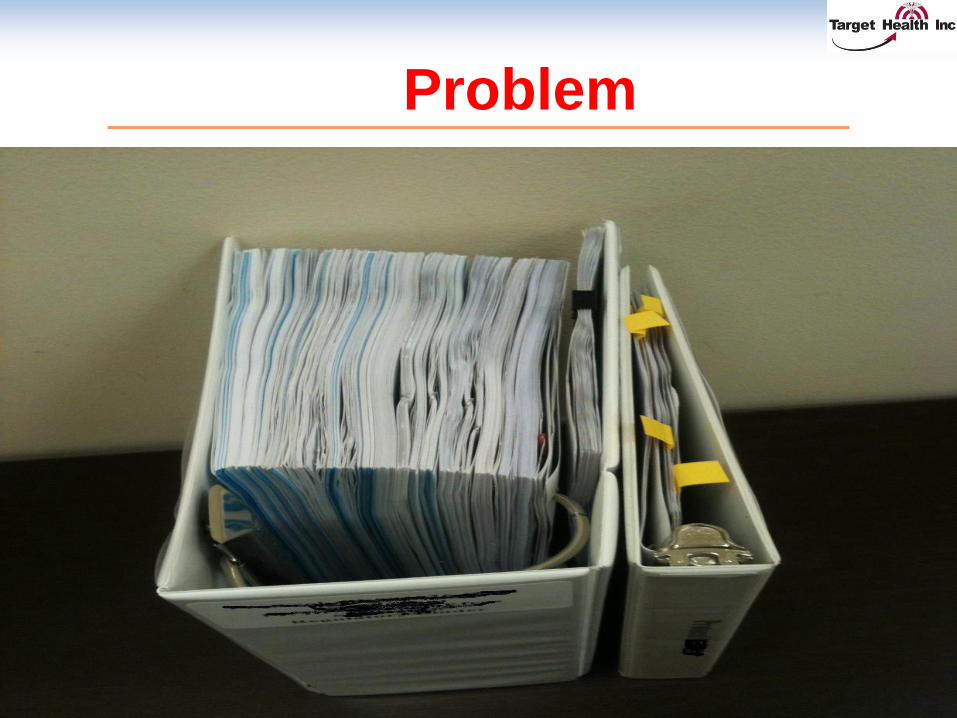
Problem
7

Solution
8
The Opportunity
Quality by Design (QbD) allows for an intelligent approach
for assuring that the clinical sites and study subjects
understand and are following the protocol.
Electronic source documents greatly reduce the need to
generate paper records, dramatically reducing the follow-
on need for onsite monitoring and SDV.
We can no longer justify spending a lot of time and money
requiring that sites first capture clinical trial data on paper,
only to subsequently transcribe those data into an
electronic EDC system, and then check the accuracy of
the transcription. 9
Business Benefits
Beyond cost savings, when performing risk-based monitoring and DDE, benefits include…
1. Improved site/sponsor relationships
2. Savings accrued to sites
3. Value of making faster, mid-course corrections
4. Improved quality of data (w/associated cost savings)
5. Focus on things that matter more effective allocation of resources
10
Key Messages
1. Full business benefit realized only through
use of processes developed to exploit its
potential
2. Direct cost savings are significant and
obvious – additional business benefits may in
fact deliver even greater value
3. Regulators can worry less about data quality
do to transcription errors
4. Clinical sites are happy as they can double
the number of office visits a day and get rid of
most of the paper!!! 11
Starting a Study
1. Write a meaningful and feasible protocol
2. During the kickoff meeting, assess the risks to the study and focus on the risk-based monitoring plan
3. Assure that the sites can really deliver subjects
4. Set up a lean hierarchy
5. Get feedback from the study sites
6. At the investigator focus on study implementation and the “10 things that can go wrong” and the risk mitigation strategies to minimize the occurrence of risky events.
7. Make sure the sites and monitors understand the importance of DDE and RBM
8. Train, train, train………………… 12
During the Study
1. Visit the sites early to do a “sniff test” and make sure the protocol is understood and being followed
2. Review the data and generate queries in real time
3. No tolerance for delays in CRF review and query aging
4. Meet weekly during the QbD meetings with all interested parties
5. Agree on review of RBM reports especially an analysis of the edit checks that are firing and queries being generated
13
During the Study
6. Assess edit check that fire and do not be afraid to make changes when it is clear there is relevance or new ones are needed
7. Review queries to ensure that they focus on things that matter
8. Have study specific online reports that focus on the “things that matter”
9. Take immediate action10. Share results among all study staff who need to
know
11. Keep meeting minutes
12. Train, train, train the sites and monitors14
Table of Contents of Clinical Data
Monitoring Plan (CDMoP)
1. Purpose2. References3. Study Roles and Responsibilities4. Tools and Processes
4.1 Study Data4.2 EDC Monitoring Module
5. Risk Mitigation Strategy6. Source Documents7. Monitoring
7.1 Onsite Monitoring7.2 Central Monitoring7.3 Qualification Visit7.4 Site Initiation Visit7.5 Interim Monitoring Visits7.6 Closeout Visit 15
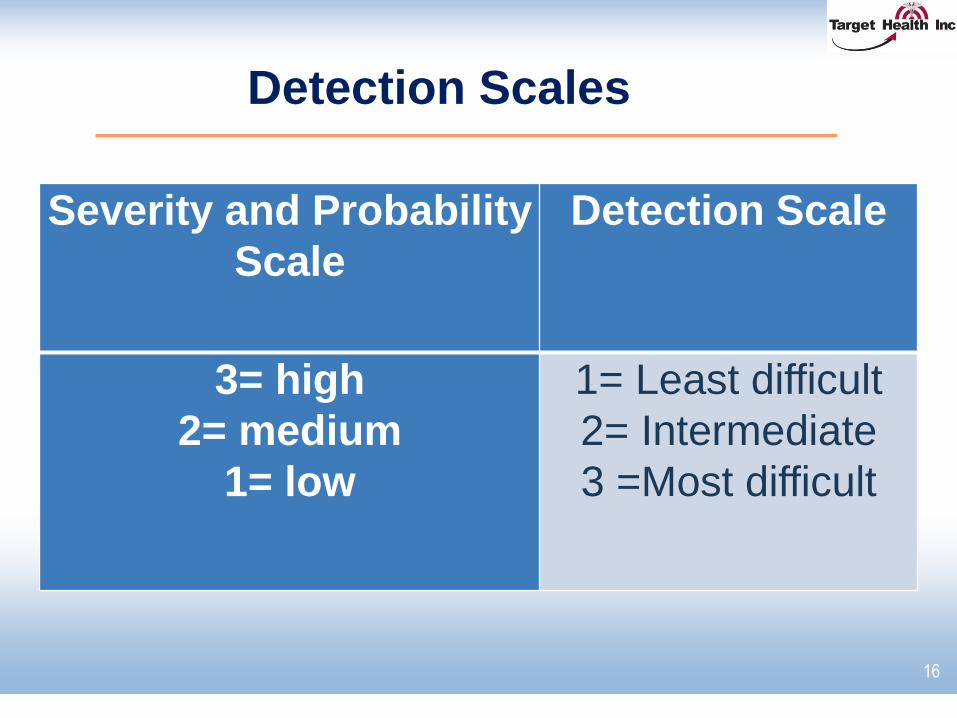
Detection Scales
16
Severity and Probability
Scale
Detection Scale
3= high
2= medium
1= low
1= Least difficult
2= Intermediate
3 =Most difficult
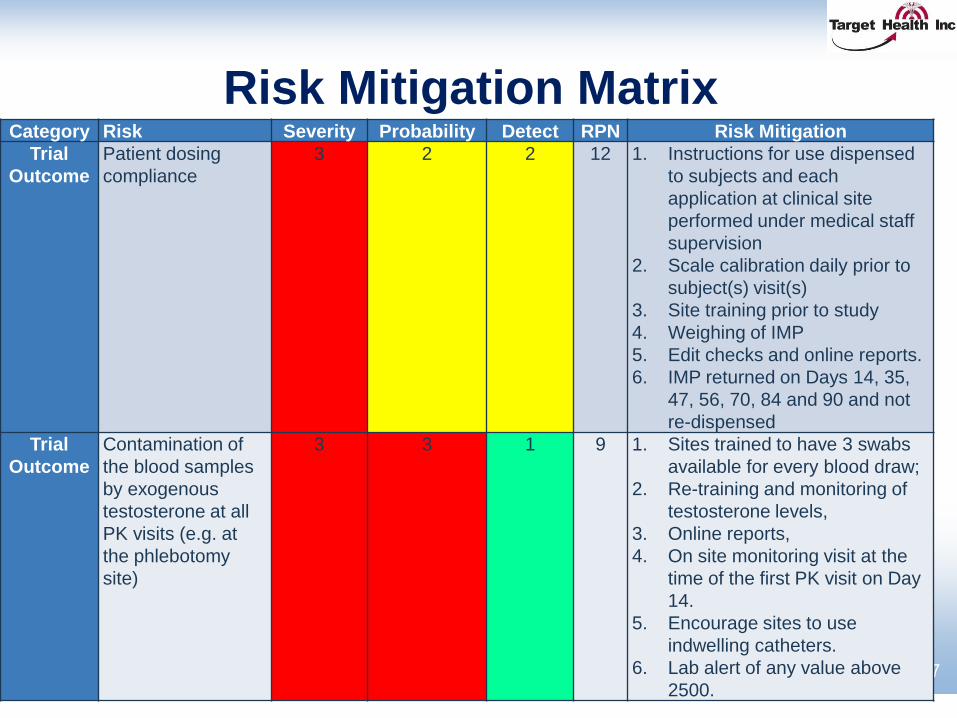
Risk Mitigation Matrix
17
Category Risk Severity Probability Detect RPN Risk Mitigation
Trial
Outcome
Patient dosing
compliance
3 2 2 12 1. Instructions for use dispensed
to subjects and each
application at clinical site
performed under medical staff
supervision
2. Scale calibration daily prior to
subject(s) visit(s)
3. Site training prior to study
4. Weighing of IMP
5. Edit checks and online reports.
6. IMP returned on Days 14, 35,
47, 56, 70, 84 and 90 and not
re-dispensed
Trial
Outcome
Contamination of
the blood samples
by exogenous
testosterone at all
PK visits (e.g. at
the phlebotomy
site)
3 3 1 9 1. Sites trained to have 3 swabs
available for every blood draw;
2. Re-training and monitoring of
testosterone levels,
3. Online reports,
4. On site monitoring visit at the
time of the first PK visit on Day
14.
5. Encourage sites to use
indwelling catheters.
6. Lab alert of any value above
2500.
Real-Time, On-Line EDC Reports
18

Sample Reports
19
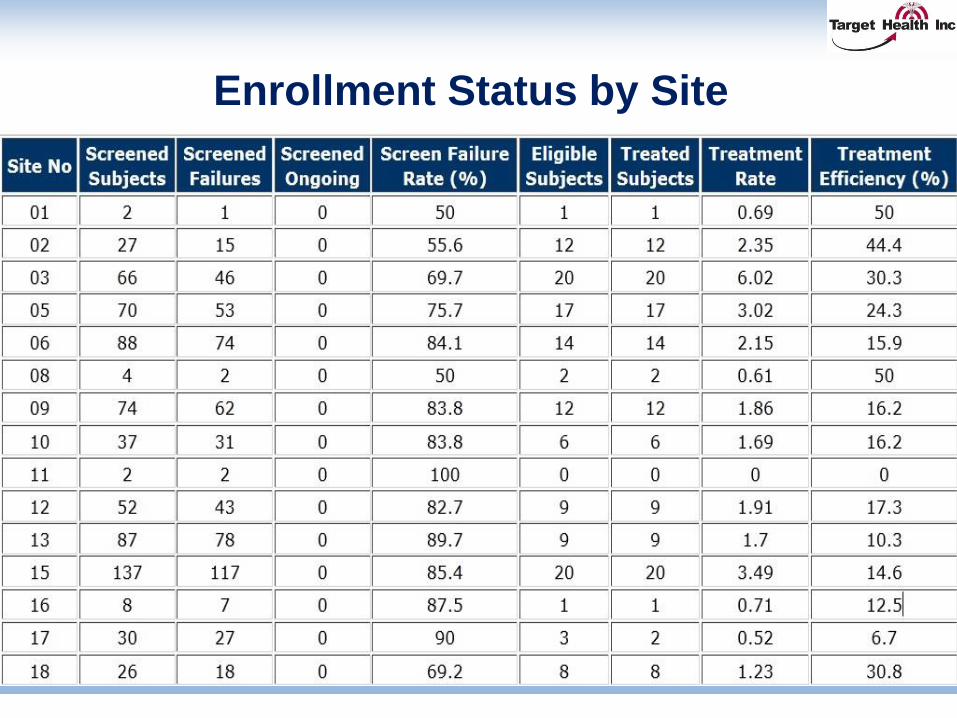
Enrollment Status by Site
20
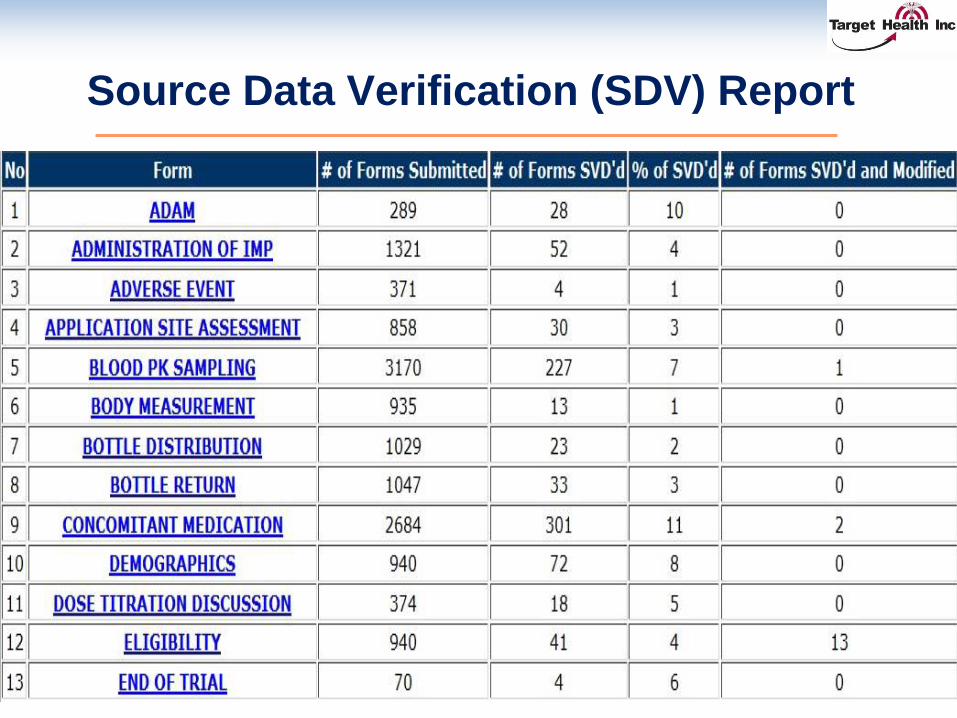
Source Data Verification (SDV) Report
21
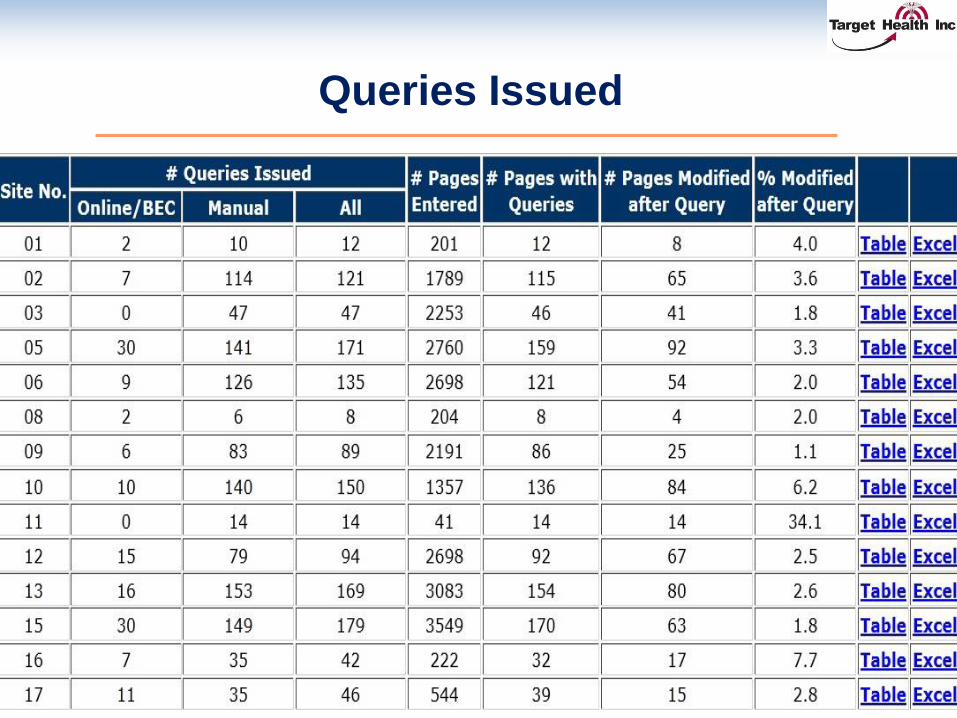
Queries Issued
22
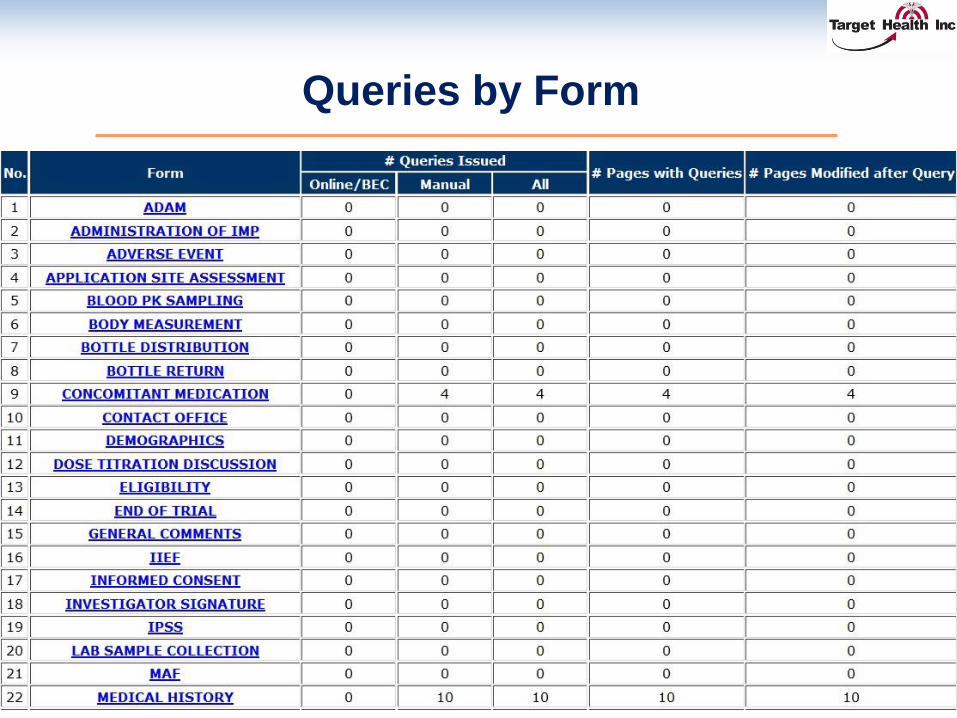
Queries by Form
23
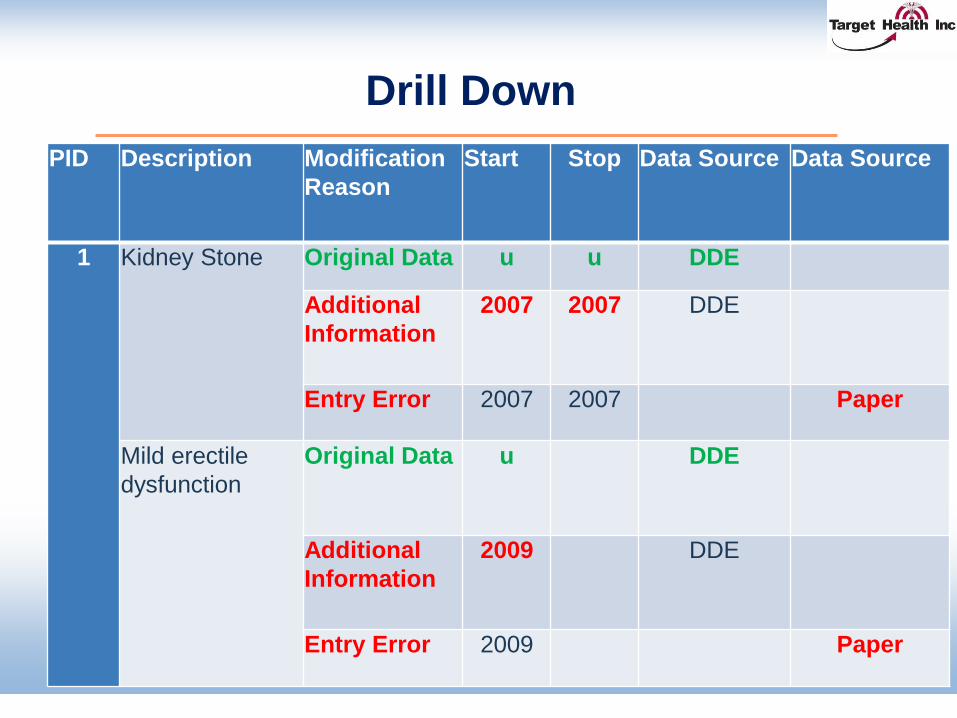
Drill Down
24
PID Description Modification
Reason
Start Stop Data Source Data Source
1 Kidney Stone Original Data u u DDE
Additional
Information
2007 2007 DDE
Entry Error 2007 2007 Paper
Mild erectile
dysfunction
Original Data u DDE
Additional
Information
2009 DDE
Entry Error 2009 Paper
eSource: eClinical Trial Record
Target e*CTR is an electronic clinical trial patient record system, access to which is controlled by the clinical investigator
Within the eCTR, the original patient record is created at the time data are initially entered into the electronic data base, and before the data are transmitted to the sponsor’s or EDC database
Therefore, the original record created within the eCTR can serve as the source
25
Target e*CTR (eClinical Trial Record)
1. Direct data capture of manually entered clinical trial data as
specified within the protocol. Other source data such as
ECG files, MRI reading etc. are captured independently of
Target e*CTR.
2. Allows for source data to be accurate, legible,
contemporaneous, original, attributable, complete and
consistent.
3. Provides an audit for the original creation and subsequent
modification of the source data.
4. Real-time retrieval of the source data.
5. Investigator maintains independent access to the original
source data.
26
Target e*CTR (eClinical Trial Record)
6. Source documents and data are protected from destruction.
7. Allows for accurate copies to be made.
8. Source documents are protected against unauthorized
access.
9. Sponsor does not have control of the source data.
10.Assure that the location of source documents and the
associated source data shall be clearly identified at all
points within the capture process.
11.Assure that when source data are copied, the process used
ensures that the copy is an exact copy preserving all of the
data and metadata of the original.
27
28
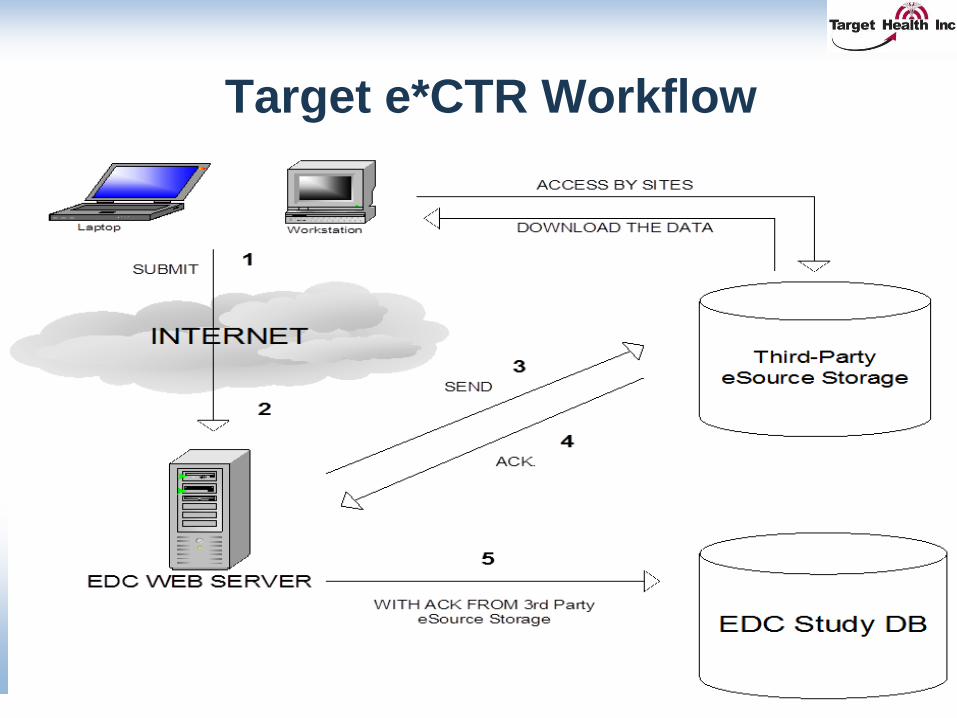
Target e*CTR Workflow
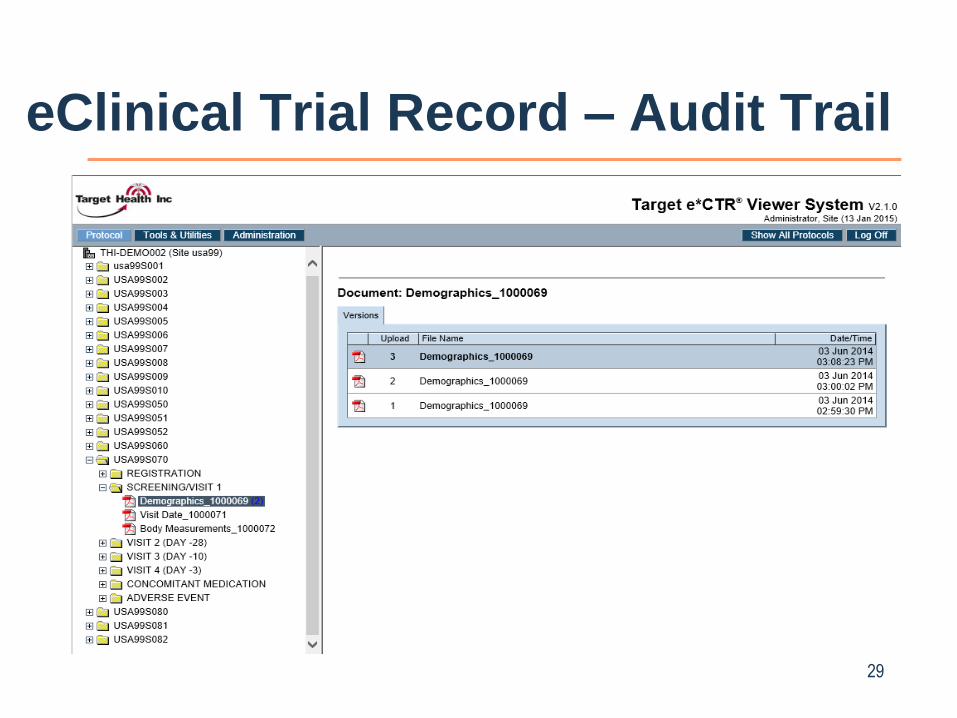
eClinical Trial Record – Audit Trail
29
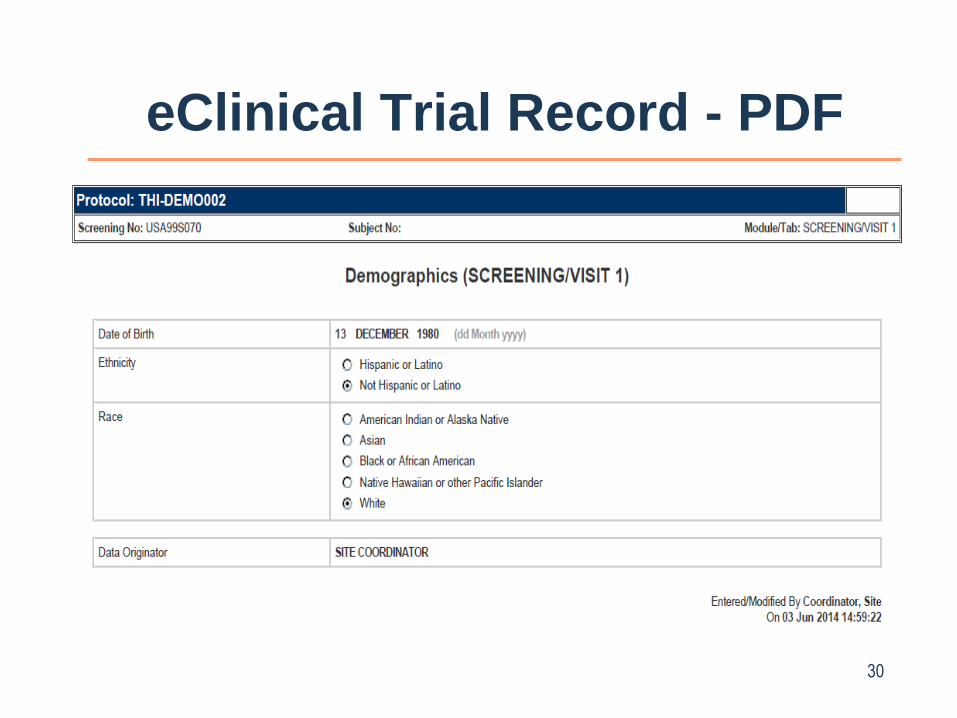
eClinical Trial Record - PDF
30
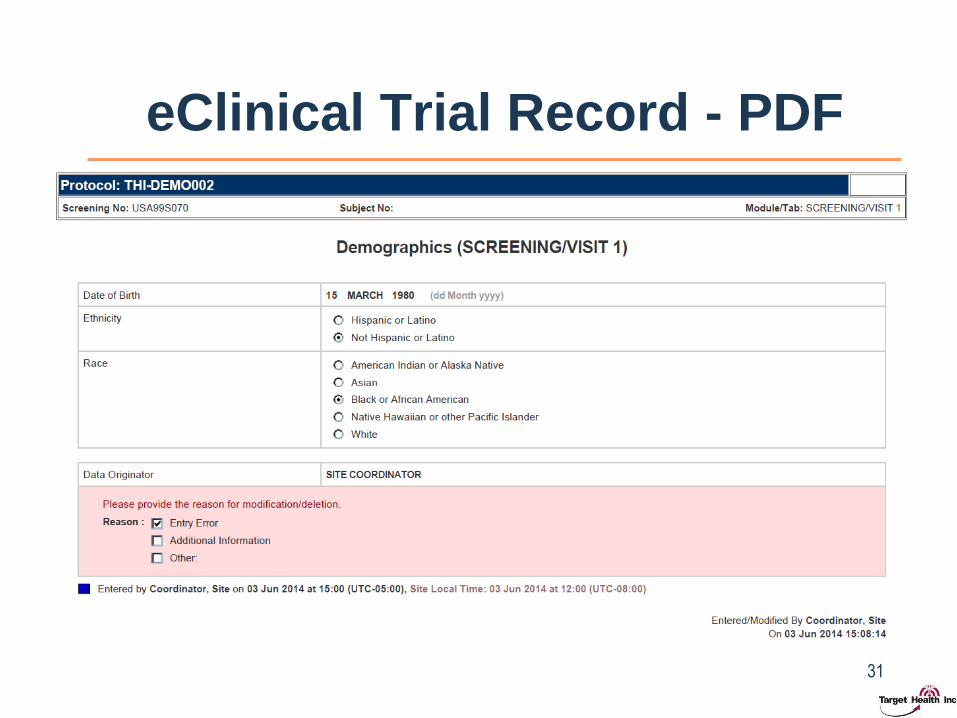
eClinical Trial Record - PDF
31
Benefits of DDE Integrated with RBM
1. Screening errors picked up early
2. Improved data quality due to immediate feedback
3. Enables Real-time monitoring
4. Major reduction in onsite monitoring
5. EDC edit checks refined early in the study
6. Compliance issues identified in real time
7. Transparency of safety issues
8. Productivity gains for sites -> High site acceptance
32
METRICS
33
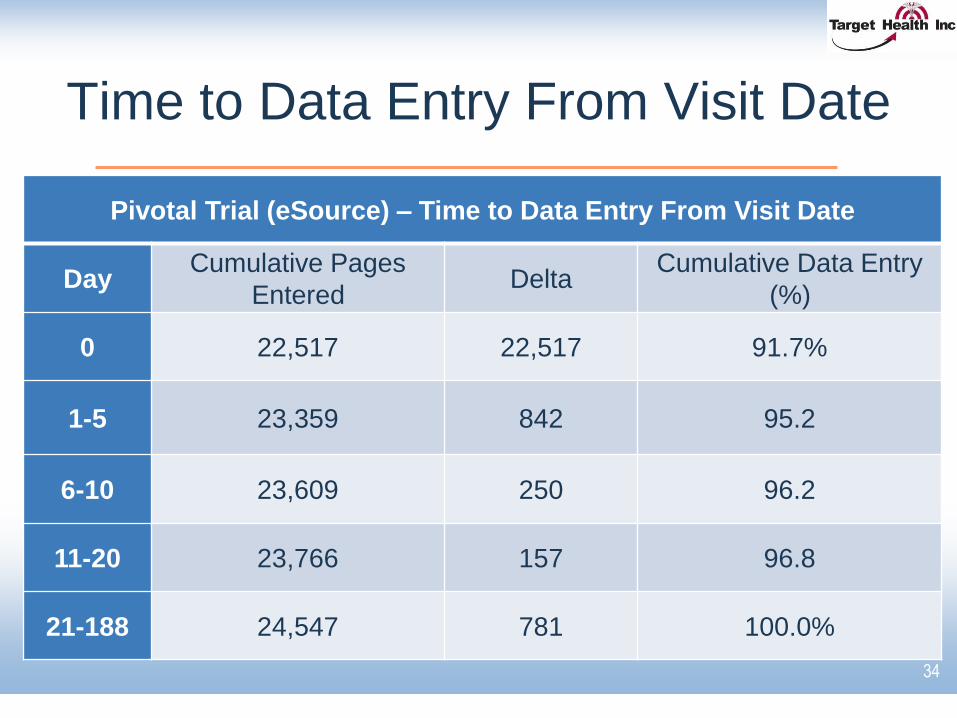
Time to Data Entry From Visit Date
34
Pivotal Trial (eSource) – Time to Data Entry From Visit Date
DayCumulative Pages
EnteredDelta
Cumulative Data Entry
(%)
0 22,517 22,517 91.7%
1-5 23,359 842 95.2
6-10 23,609 250 96.2
11-20 23,766 157 96.8
21-188 24,547 781 100.0%
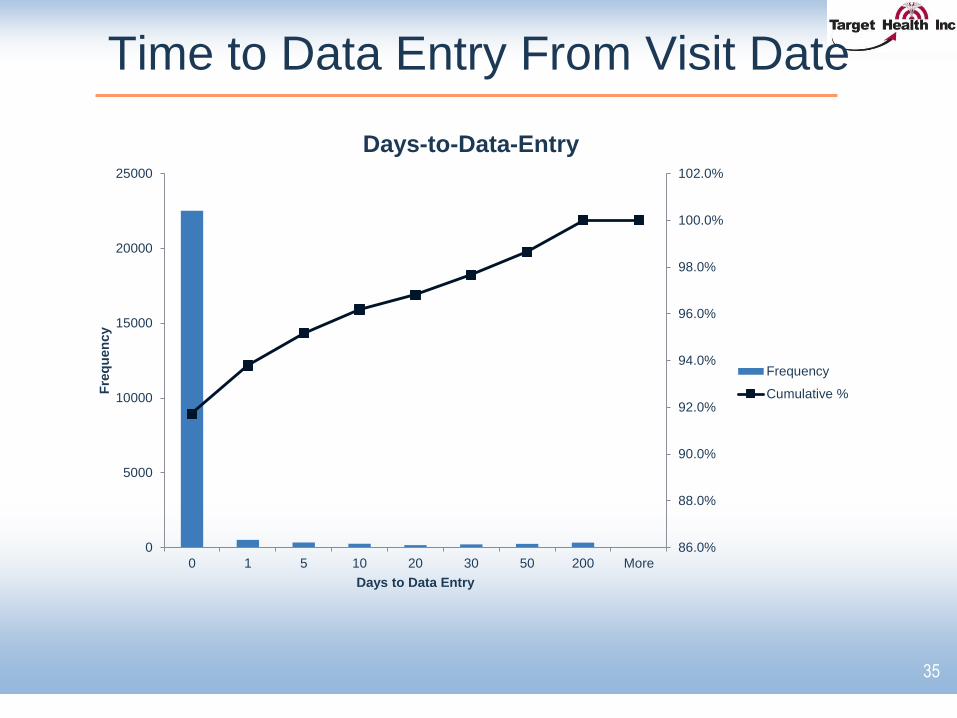
Time to Data Entry From Visit Date
35
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
102.0%
0
5000
10000
15000
20000
25000
0 1 5 10 20 30 50 200 More
Fre
qu
en
cy
Days to Data Entry
Days-to-Data-Entry
Frequency
Cumulative %
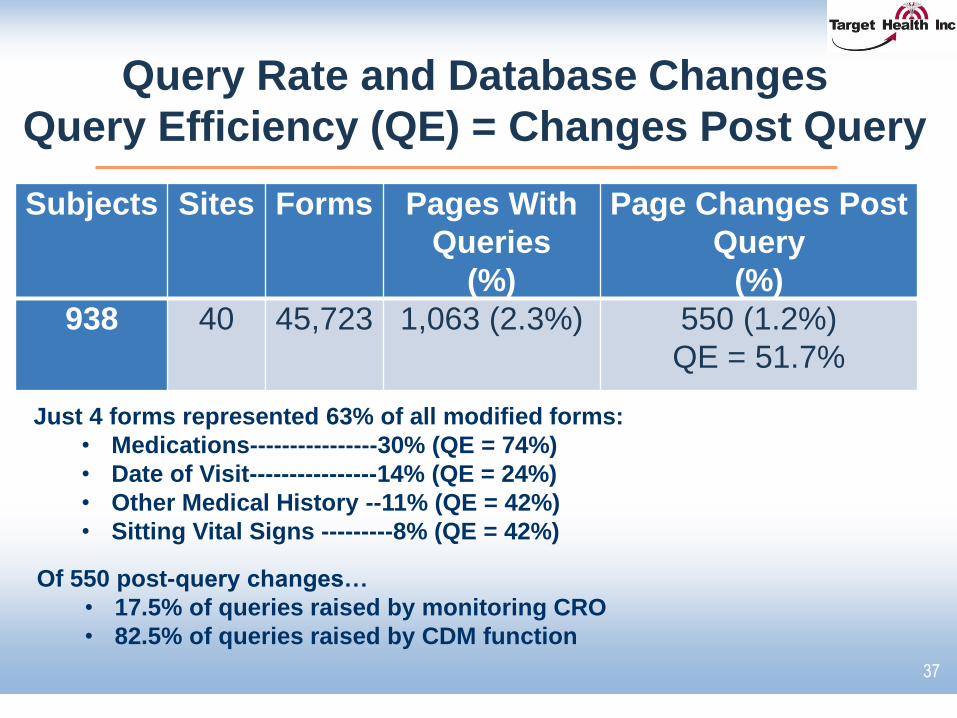
Query Rate and Database Changes
Query Efficiency (QE) = Changes Post Query
37
Subjects Sites Forms Pages With
Queries
(%)
Page Changes Post
Query
(%)
938 40 45,723 1,063 (2.3%) 550 (1.2%)
QE = 51.7%
Of 550 post-query changes…
• 17.5% of queries raised by monitoring CRO
• 82.5% of queries raised by CDM function
Just 4 forms represented 63% of all modified forms:
• Medications----------------30% (QE = 74%)
• Date of Visit----------------14% (QE = 24%)
• Other Medical History --11% (QE = 42%)
• Sitting Vital Signs ---------8% (QE = 42%)
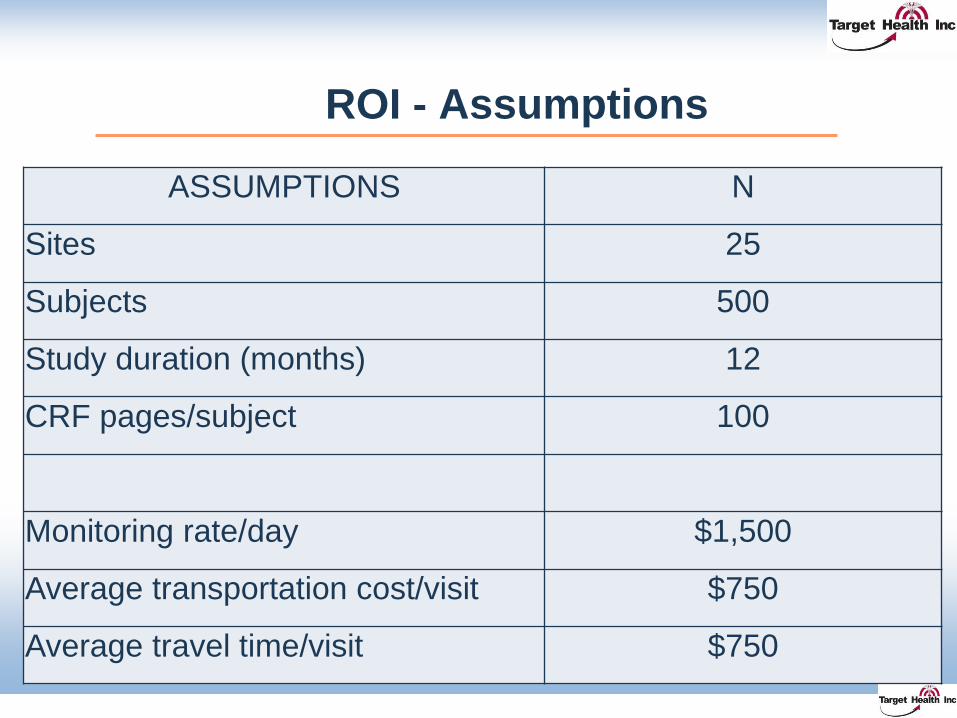
ROI - Assumptions
38
ASSUMPTIONS N
Sites 25
Subjects 500
Study duration (months) 12
CRF pages/subject 100
Monitoring rate/day $1,500
Average transportation cost/visit $750
Average travel time/visit $750
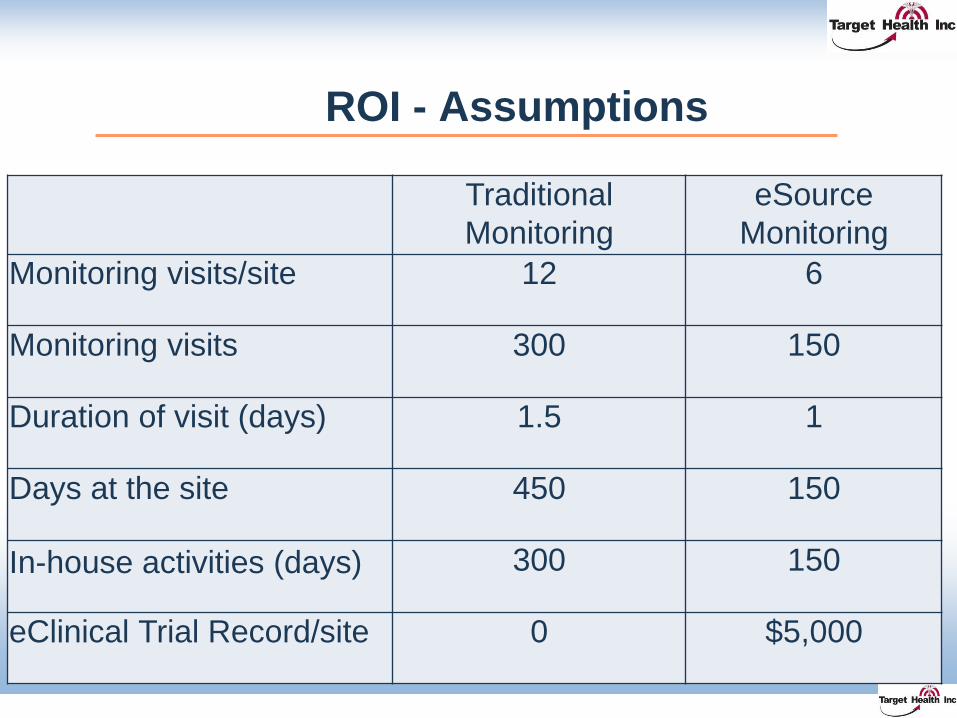
ROI - Assumptions
39
Traditional
Monitoring
eSource
Monitoring
Monitoring visits/site 12 6
Monitoring visits 300 150
Duration of visit (days) 1.5 1
Days at the site 450 150
In-house activities (days) 300 150
eClinical Trial Record/site 0 $5,000
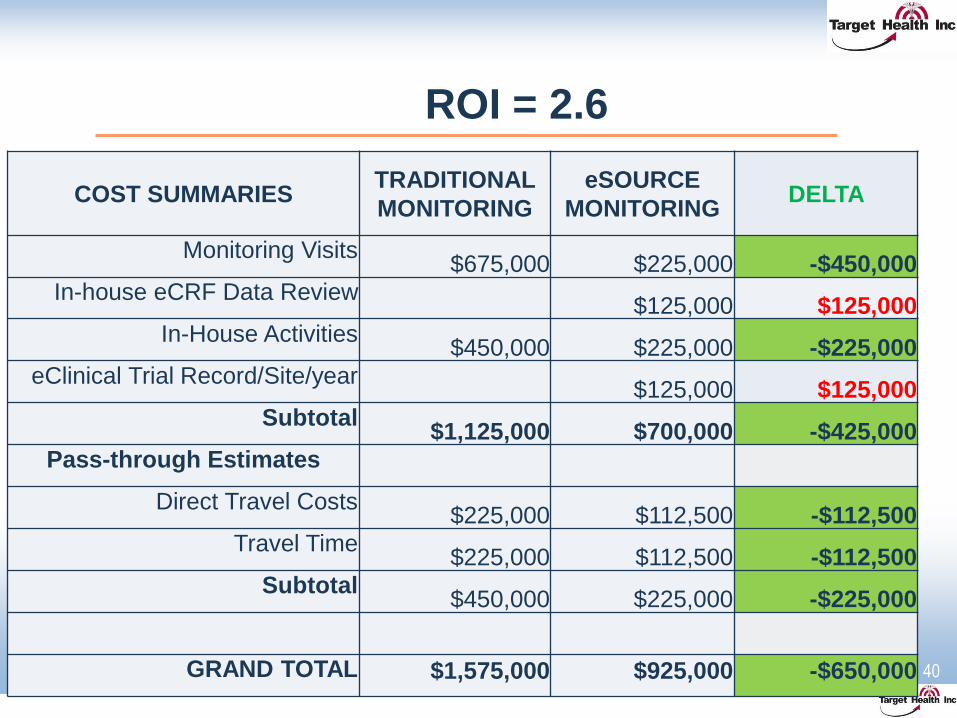
ROI = 2.6
40
COST SUMMARIESTRADITIONAL
MONITORING
eSOURCE
MONITORINGDELTA
Monitoring Visits$675,000 $225,000 -$450,000
In-house eCRF Data Review$125,000 $125,000
In-House Activities$450,000 $225,000 -$225,000
eClinical Trial Record/Site/year $125,000 $125,000
Subtotal$1,125,000 $700,000 -$425,000
Pass-through Estimates
Direct Travel Costs$225,000 $112,500 -$112,500
Travel Time$225,000 $112,500 -$112,500
Subtotal$450,000 $225,000 -$225,000
GRAND TOTAL $1,575,000 $925,000 -$650,000
Thank You
Jules T. Mitchel, MBA, Ph.D., President
Target Health Inc.
261 Madison Avenue, 24th Floor, New York, NY 10016
www.targethealth.com
TARGET HEALTH INC., founded in 1993, is a private, New
York City-based, full-service eCRO, engaged in all aspects of
Drug and Device Development, including Regulatory Affairs
Strategic Planning, Clinical Research, Data Management,
Biostatistics, Medical Writing and the paperless clinical trial.
41