Embed Size (px)
Citation preview
IMMEDIATE IMPLANT PLACEMENT
- DR. KAPIL ARORA
CONTENTS
• INTRODUCTION• HEALING OF EXTRACTION SOCKET• TRADITIONAL PROTOCOLS• TIMING OF IMPLANT PLACEMENT• IMMEDIATE IMPLANT PLACEMENT• ADVANTAGES• INDICATIONS • CONTRAINDICATIONS
• CLASSIFICATION OF EXTRACTION SITES• TREATMENT SEQUENCE• SURGICAL PROCEDURE• DIFFERENT TREATMENT PROTOCOLS• SOFT TISSUE MANAGEMENT• POST-OP MANAGEMENT • DISADVANTAGES• CLINICAL TRIALS• CLINICAL FACTORS TO BE CONSIDERED!!• CONCLUSION

INTRODUCTION
• Following an extraction there is a 25% decrese in the width of the alveolar boneduring first year and an average 4mm decrease in height during the first year following multiple extractions (Carlson 1967)
• Tatum and Misch have observed a 40%-60% decrease in alveolar bone width after the first 2-3 years post extraction.
• Christensen reports an annual resorption rate of at least 0.5% to 1% during the remainder for the rest of a patients lifes
• Schropp et al (2003) most of the bone gain in the socket occurred in the first 3 months.
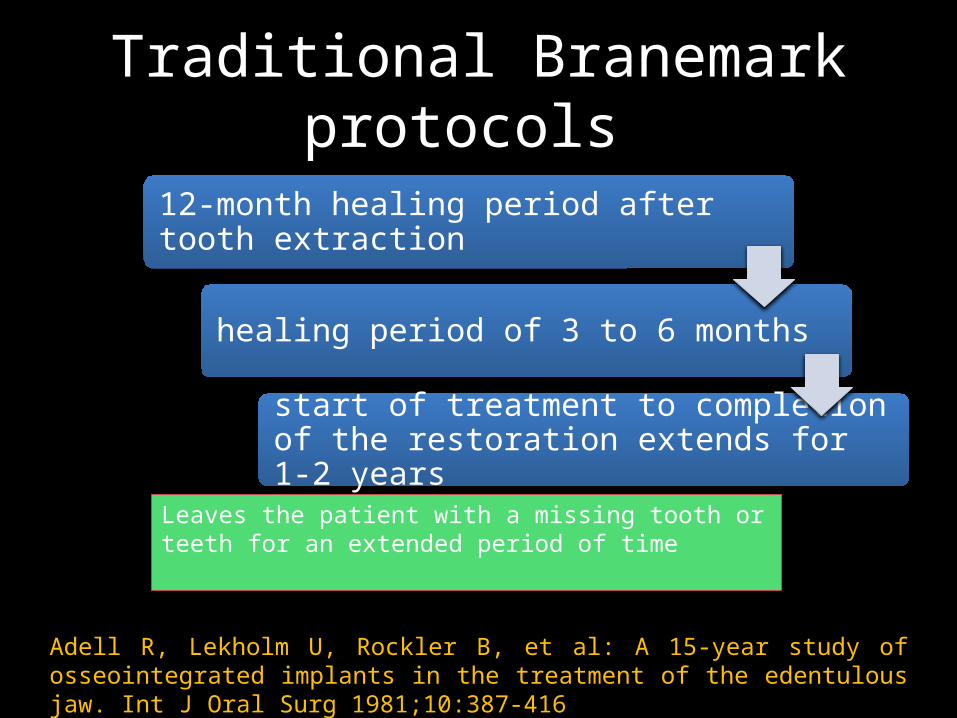
Traditional Branemark protocols
12-month healing period after tooth extraction
healing period of 3 to 6 months
start of treatment to completion of the restoration extends for 1-2 years
Leaves the patient with a missing tooth or teeth for an extended period of time
Adell R, Lekholm U, Rockler B, et al: A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10:387-416
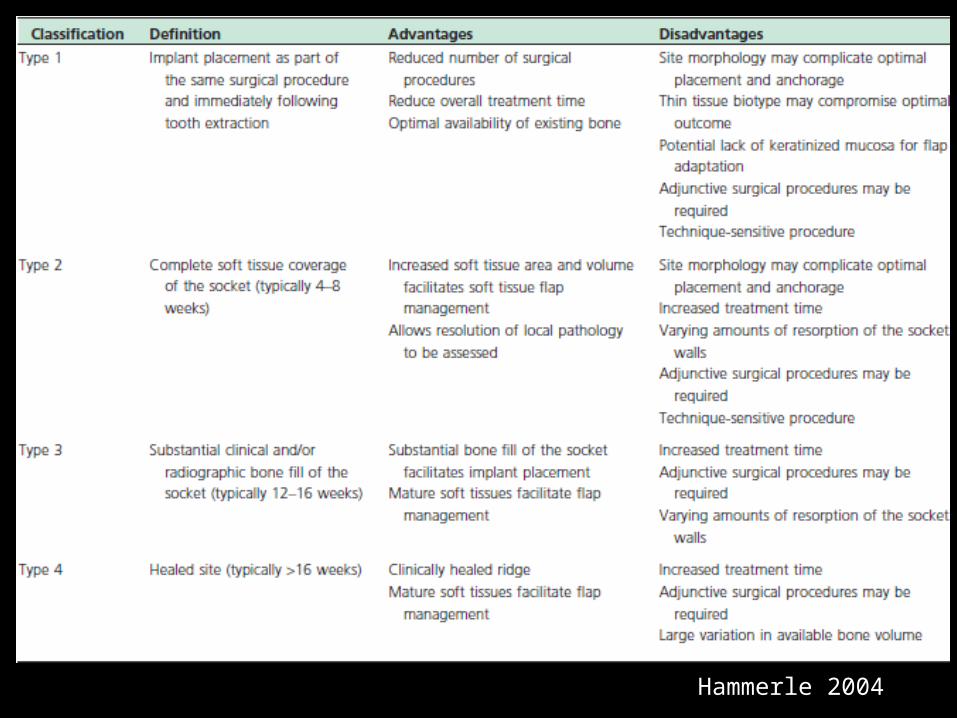
Hammerle 2004
KEY ASPECTS OF THIS CLASSIFICATION
• In clinical practice the decision to place an implant following tooth extraction is usually determined by:
- The attainment of specific soft and hard tissue characteristics of the healing socket
- These events do not necessarily follow rigid time frames and may vary according to the site and patients factors
• To avoid time based descriptions, this classification uses numeric descriptors
Type 1 is chosen- when an implant is placed immediately following extractionType 2 is preferred- when advanced soft tissue healing is desiredType 4 – hard tissue healing is desired
SOFT TISSUE CHANGES AFTER EXTRACTION
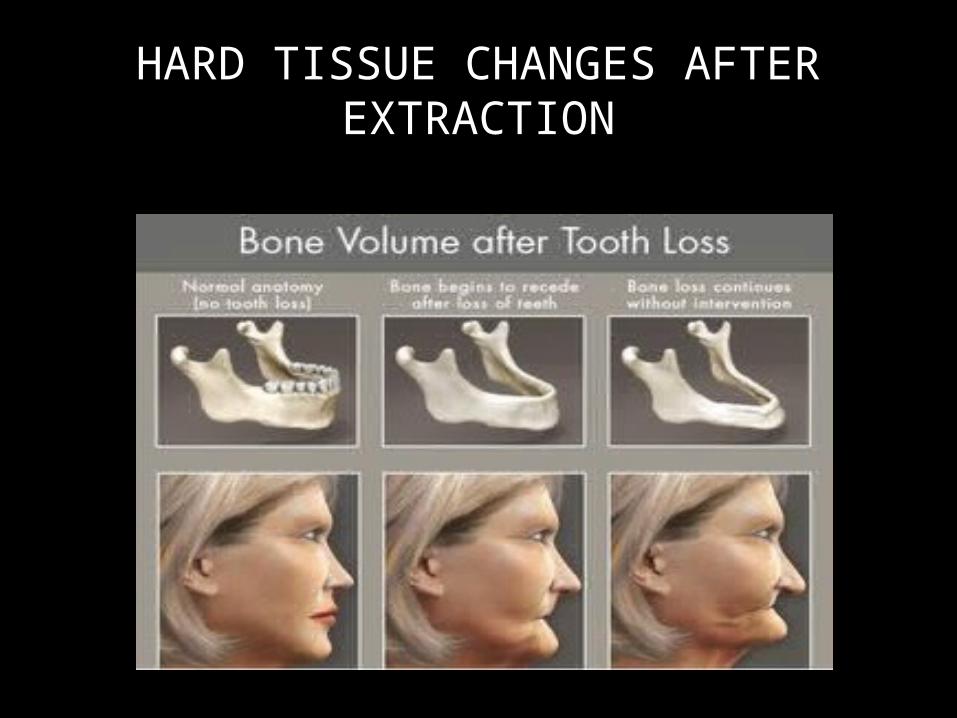
HARD TISSUE CHANGES AFTER EXTRACTION
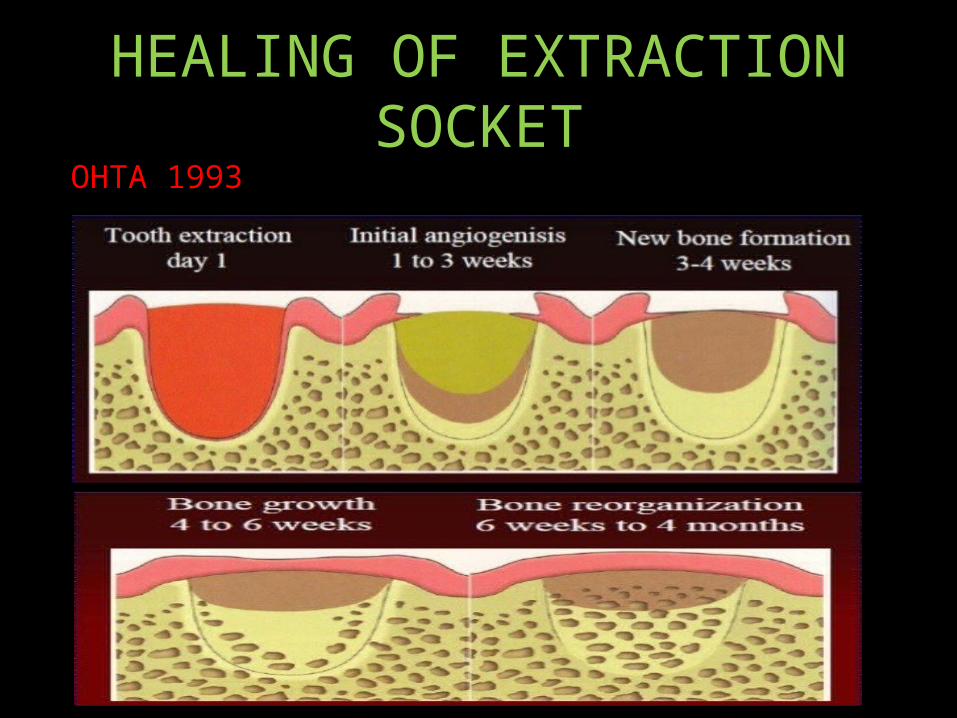
HEALING OF EXTRACTION SOCKETOHTA 1993
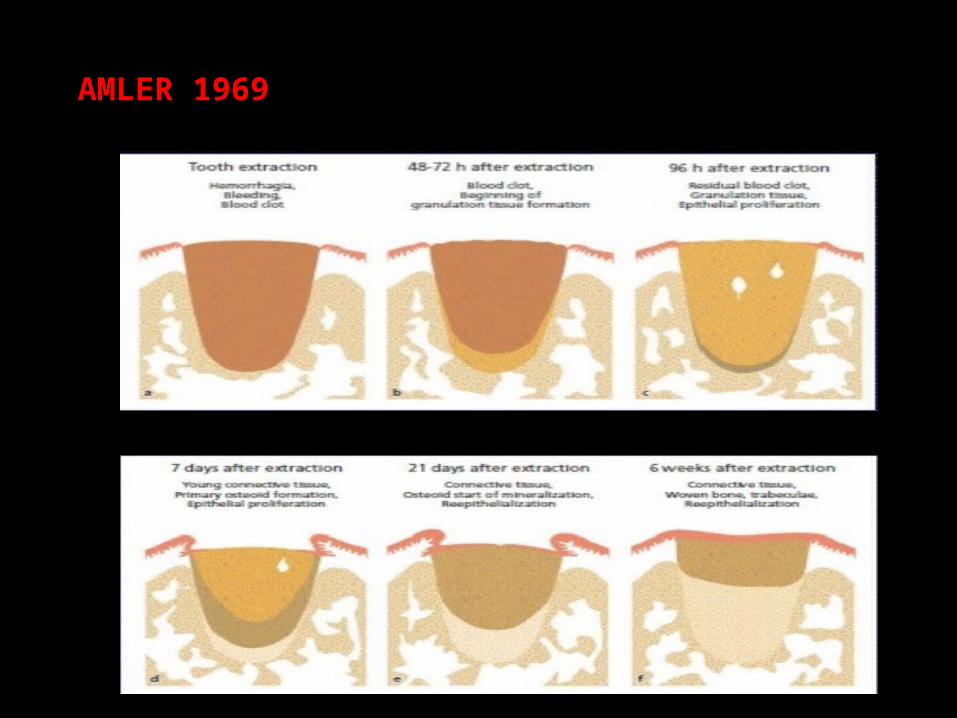
AMLER 1969
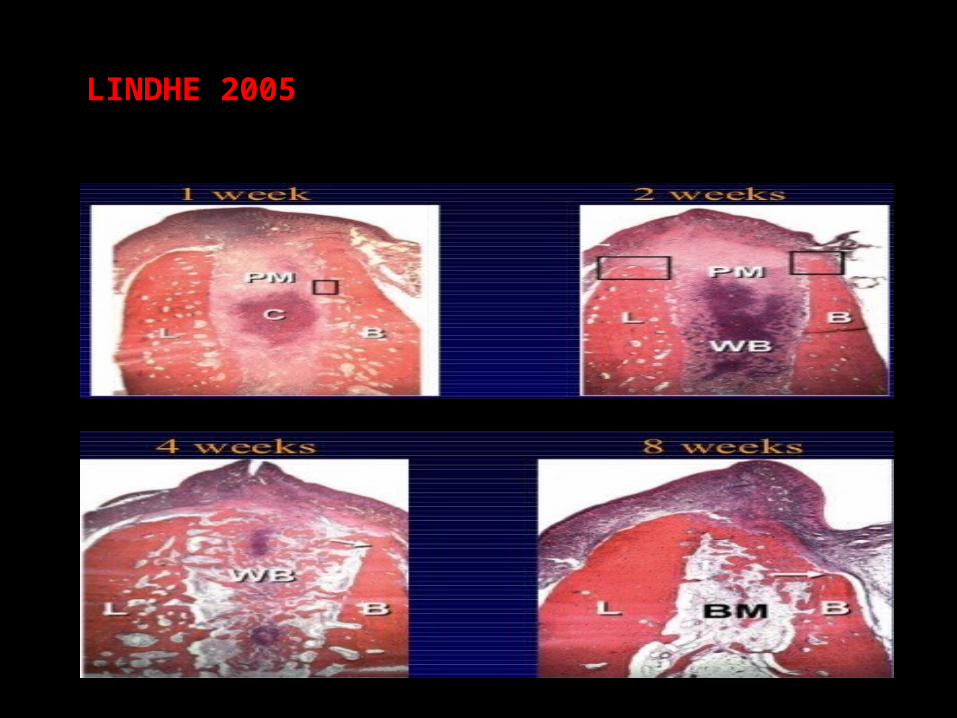
LINDHE 2005
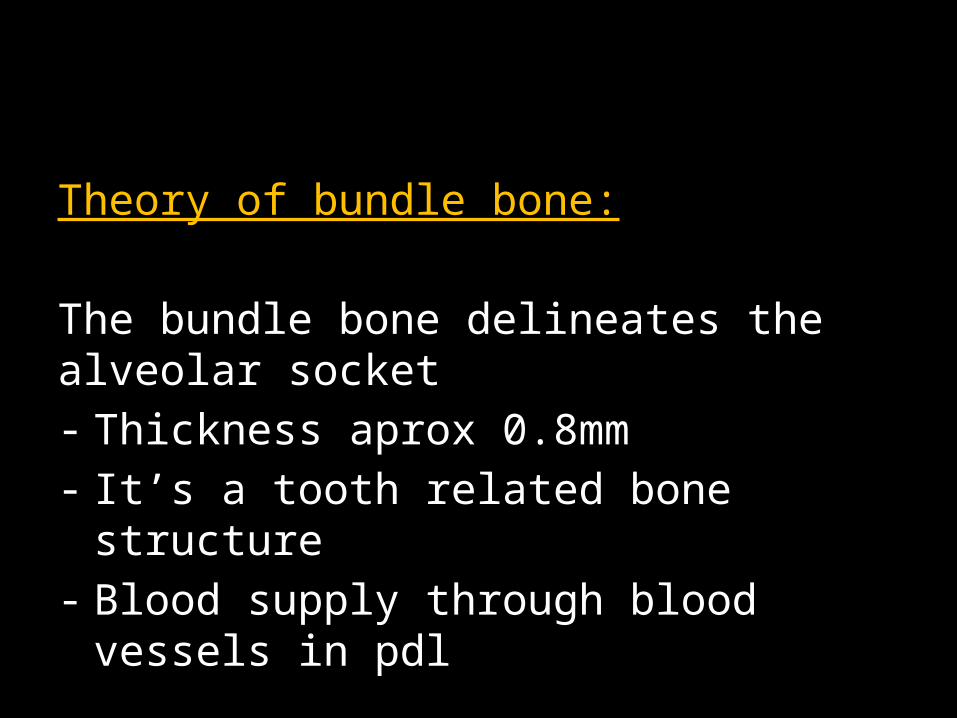
Theory of bundle bone:
The bundle bone delineates the alveolar socket- Thickness aprox 0.8mm- It’s a tooth related bone structure- Blood supply through blood vessels in pdl
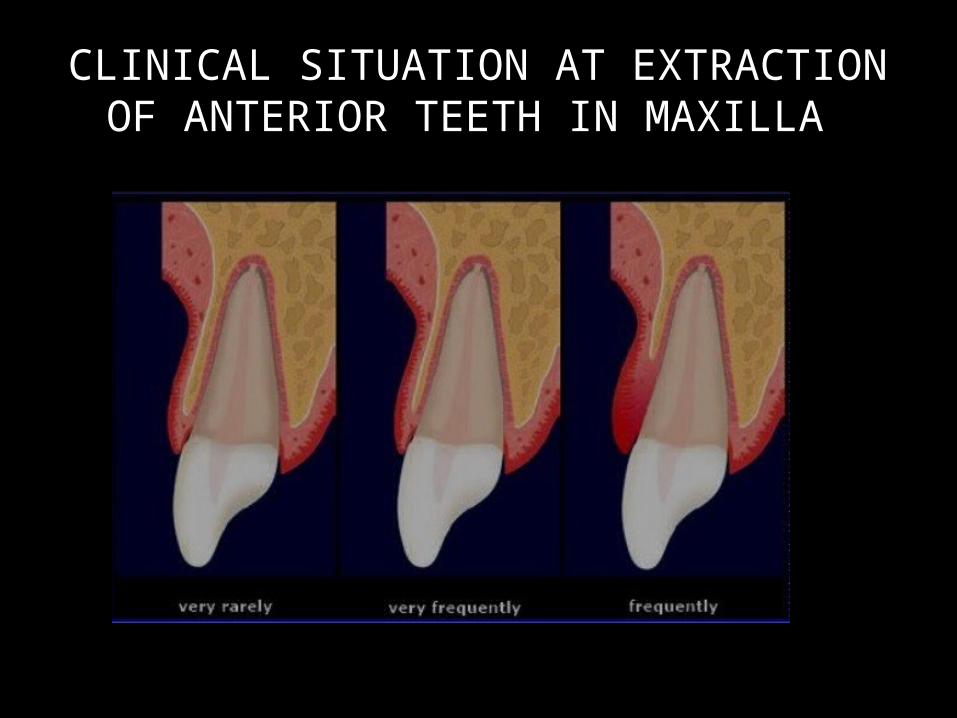
CLINICAL SITUATION AT EXTRACTION OF ANTERIOR TEETH IN MAXILLA
Attempts to shorten the overall length of treatment have focused on
Shortened or immediate loading subsequent to implant placement
Alteration of the surface of the implant fixture to promote faster healing
Immediate placement of the implant after extraction of the natural tooth
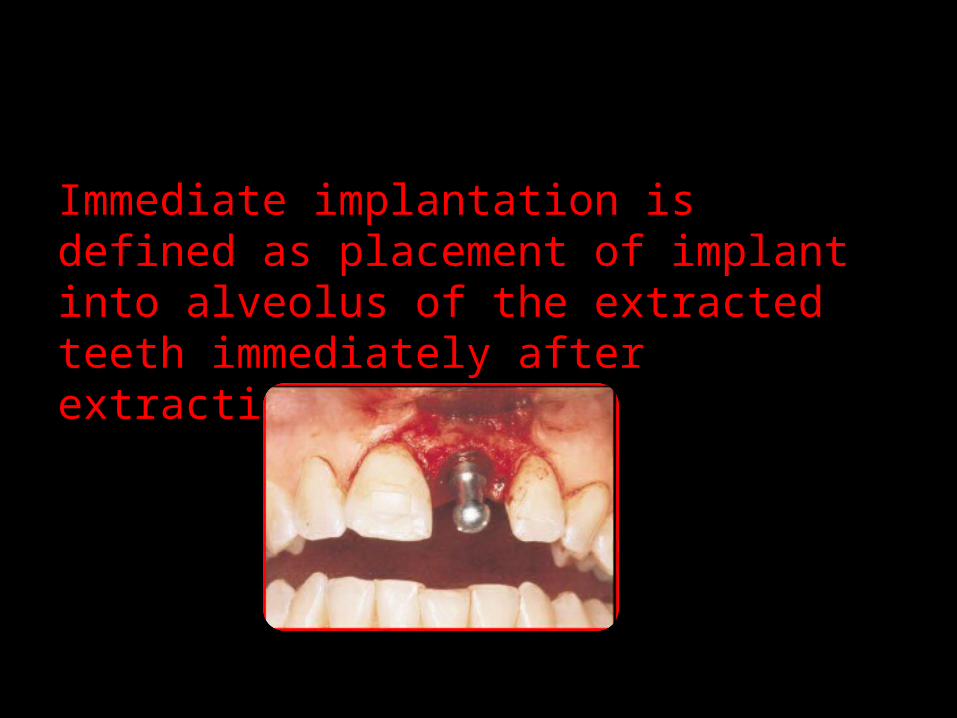
Immediate implantation is defined as placement of implant into alveolus of the extracted teeth immediately after extraction.
IMMEDIATE IMPLANT PLACEMENT
Placing an implant
Most edentulous sites are atrophic
Result of inadequate mechanical loading
Time dependant and localised healing
response
Controlled by cytokines
• Placement of implants into fresh extraction sites offer a no. of advantages to both the patients and the clinicians
• Without the support provided by functioning dental units, the bony receptor sites soon undergo a catabolic phase
• Varying amounts of atrophy occur after tooth removal.
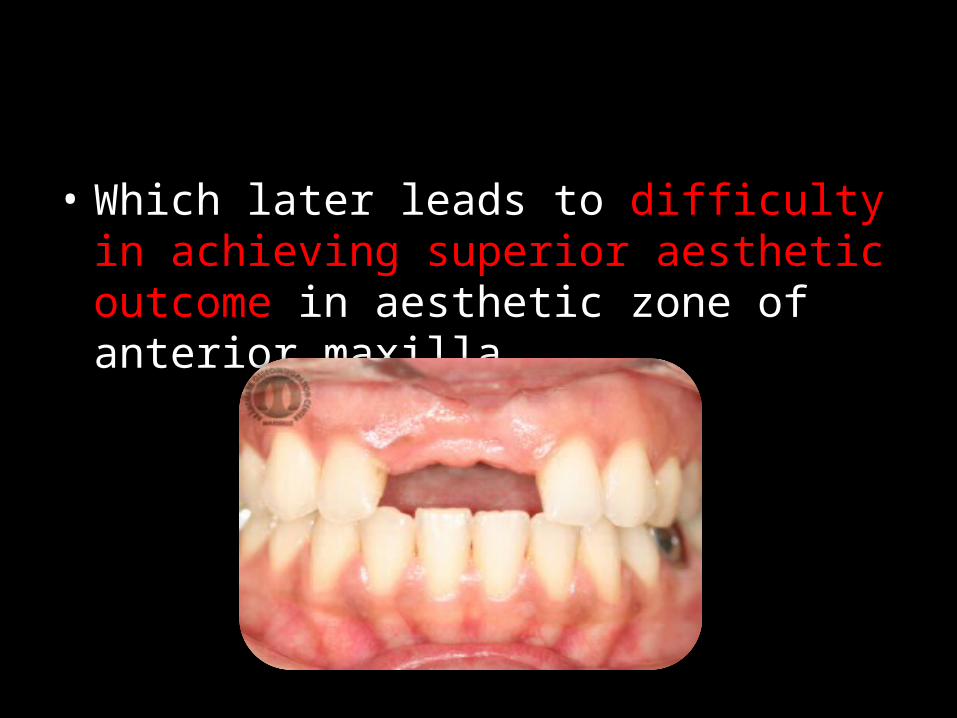
• Which later leads to difficulty in achieving superior aesthetic outcome in aesthetic zone of anterior maxilla.
ADVANTAGES
Patients acceptability
Reduces treatment time
Socket as a guide for determination of parallelism and alignment
Surgeon can position the implant more favourably than the original position
Facilitates final restoration and minimizes need for severly angled abutments
Implants in extraction sites can be placed in th same position as the extracted teeth
INDICATIONS
• The ideal extraction site for immediate implant placement
little or no periodontal bone loss on the tooth that is to be extracted, such as a tooth being extracted due to
endodontic involvement
root fracture, root resorption
periapical pathology
root perforation,
unfavorable crown-to-root ratio
CONTRAINDICATIONS
Presence of pusLack of bone beyond the
apex
Close proximity to anatomical vital structures
Clinical conditions preventing
primary closure
CLASSIFICATION OF EXTRACTION SITES
Type 1•ideal for immediate implantation, •3 to 4 wall sockets with minimal bone resorption, •sufficient bone beyond the apex,•manageable gingival recession and•esthetics is not essential.
Type 2• requiring orthodontic extrusive augmentation, •significant recession and esthetics is essential.
Type 3•not suitable owing to inadequate vertical and buccolingual dimensions, recession and•severe circumferential and angular defects.
J periodontol 1997;68;915-923
TREATMENT SEQUENCE AND PLANNING PROTOCOL
Clinical examination
Radiographic examination
Fabrication of surgical guide
Surgical and prosthetic phase
Maintenance
CLINICAL EXAMINATION
• PRE-SURGICAL
• Most researchers recommend
at least 3 to 5 mm of bone beyond the apex and
a bony length of 10 mm or greater for stability when placing immediate implants.
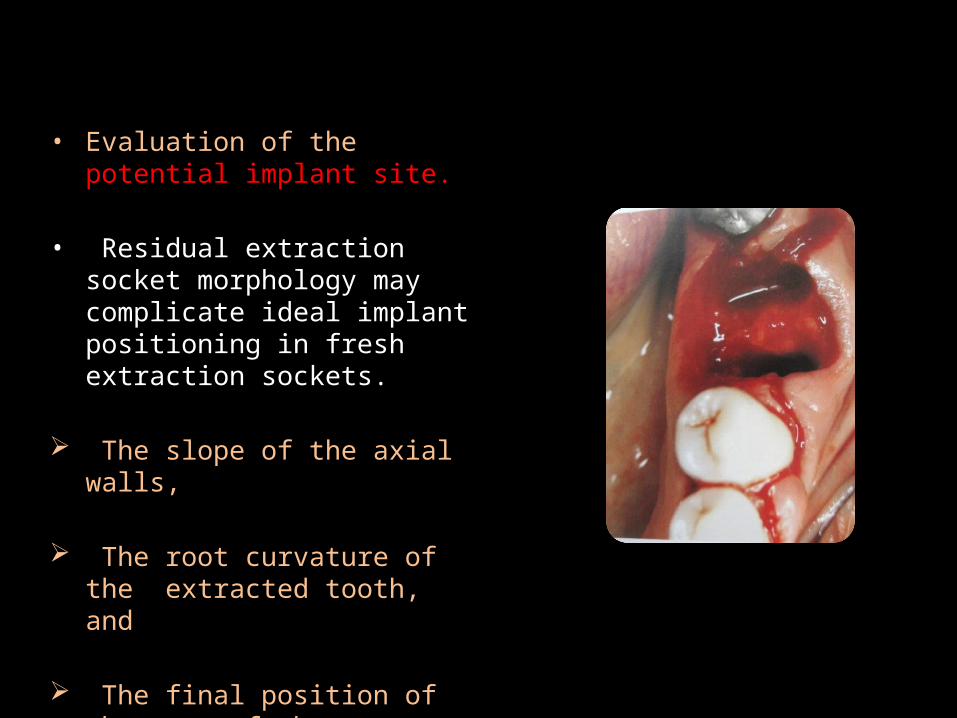
• Evaluation of the potential implant site.
• Residual extraction socket morphology may complicate ideal implant positioning in fresh extraction sockets.
The slope of the axial walls,
The root curvature of the extracted tooth, and
The final position of the apex of the extracted tooth in the alveolar housing
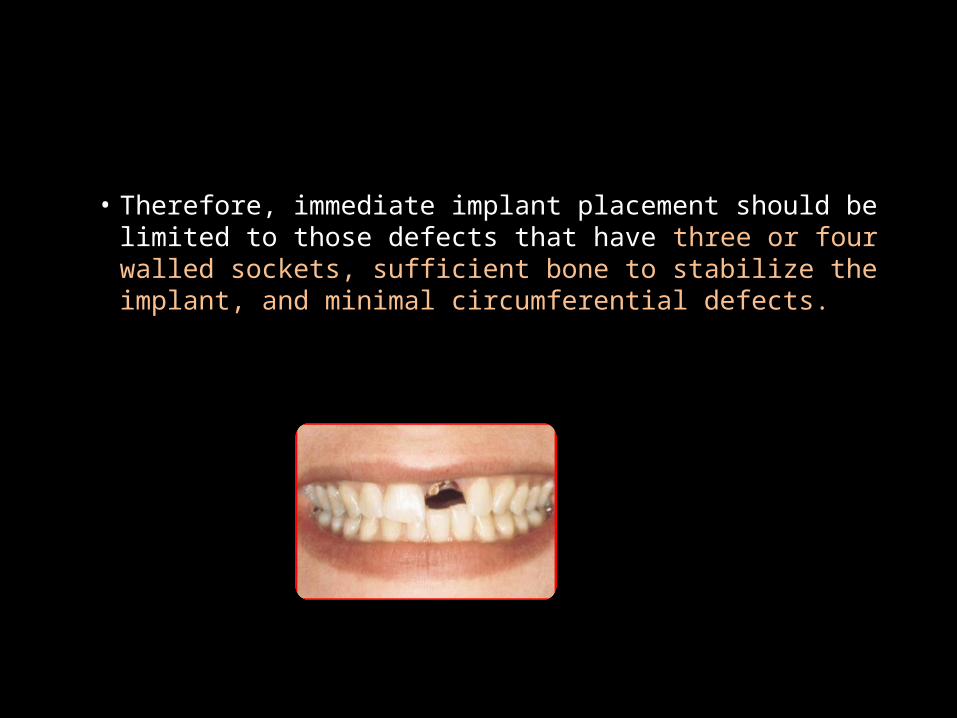
• Therefore, immediate implant placement should be limited to those defects that have three or four walled sockets, sufficient bone to stabilize the implant, and minimal circumferential defects.
• Wilson et al showed that the horizontal or circumferential component of the peri-implant defect was a critical factor and that the horizontal defects of less than 1.5 mm do not need membranes to obtain histologic osseointegration.
Wilson TG, Jr, Schenk R, Buser D, et al: Implants placed in immediate extraction sites: a report of histologic and histometric analyses of human biopsies. Int J Oral Maxillofac Implants 1998;13:333-341
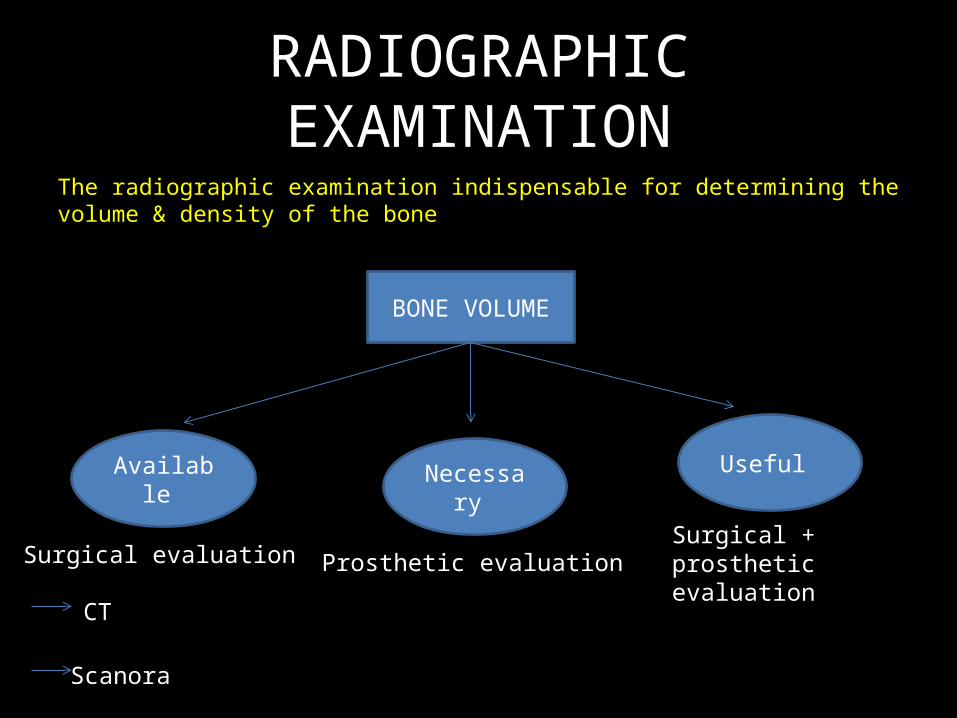
RADIOGRAPHIC EXAMINATIONThe radiographic examination indispensable for determining the volume & density of the bone
BONE VOLUME
Available Necessary Useful
Surgical evaluation Prosthetic evaluationSurgical + prosthetic evaluation
CT
Scanora
• Good evaluation of bone density allows the surgeon to do the following:
- Select proper implant diameter- Decide about optimal drilling - Determine the length of healing period- Evaluate the occlusal load capacity
CLASSIFICATION OF BONE QUALITY
LEKHOLM & ZARB (1985)
Mechanical aspect (bone density)
Type I- essentially cortical bone
Type II- dense corticocancellous bone
Type III- sparse corticocancellous bone
Type IV- thin cortical and very sparse medullary bone
Healing stand point (bone biology)
BHP 1- normal healing potential
BHP 2- moderately reduced healing potential
BHP 3- substantially reduced healing potential

SURGICAL GUIDE


SURGICAL PROCEDURE
• Atraumatic extraction using mini surgical blade or a periotome
• Maintain most of the alveolar housing of the tooth to be
extracted.
careful inspection of the extraction socket
walls are thoroughly curetted to remove all remnants of the periodontal ligament
Irrigated with normal saline
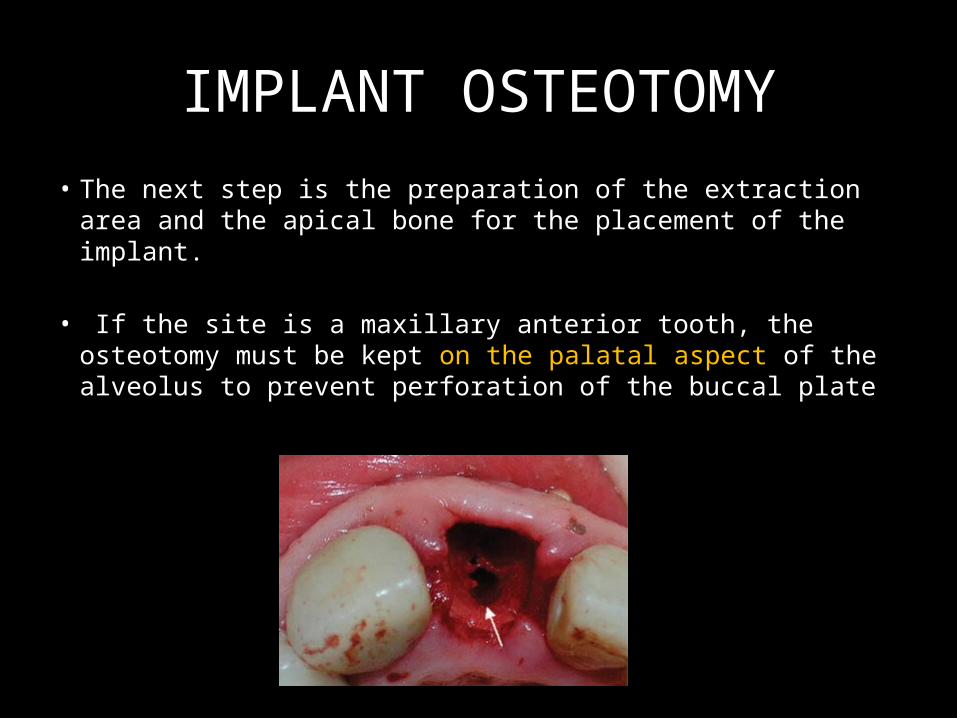
IMPLANT OSTEOTOMY
• The next step is the preparation of the extraction area and the apical bone for the placement of the implant.
• If the site is a maxillary anterior tooth, the osteotomy must be kept on the palatal aspect of the alveolus to prevent perforation of the buccal plate
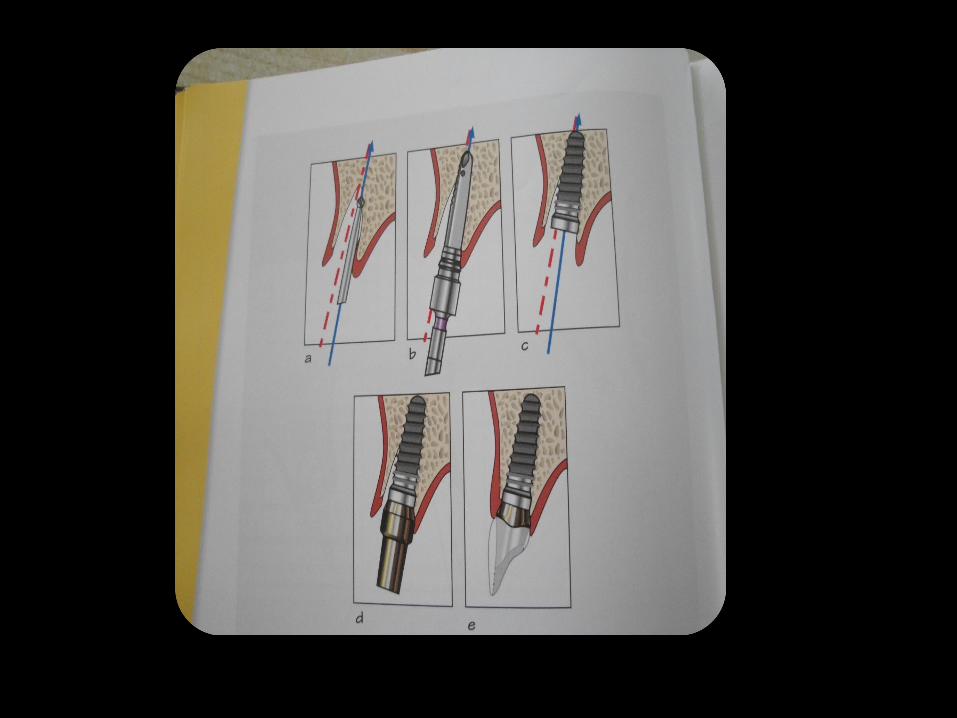
• Once the osteotomy is prepared to the desired depth with at least 3 to 5 mm of intimate implant-to-bone contact, an implant is placed.
• The implant must be stable within, with no mobility.
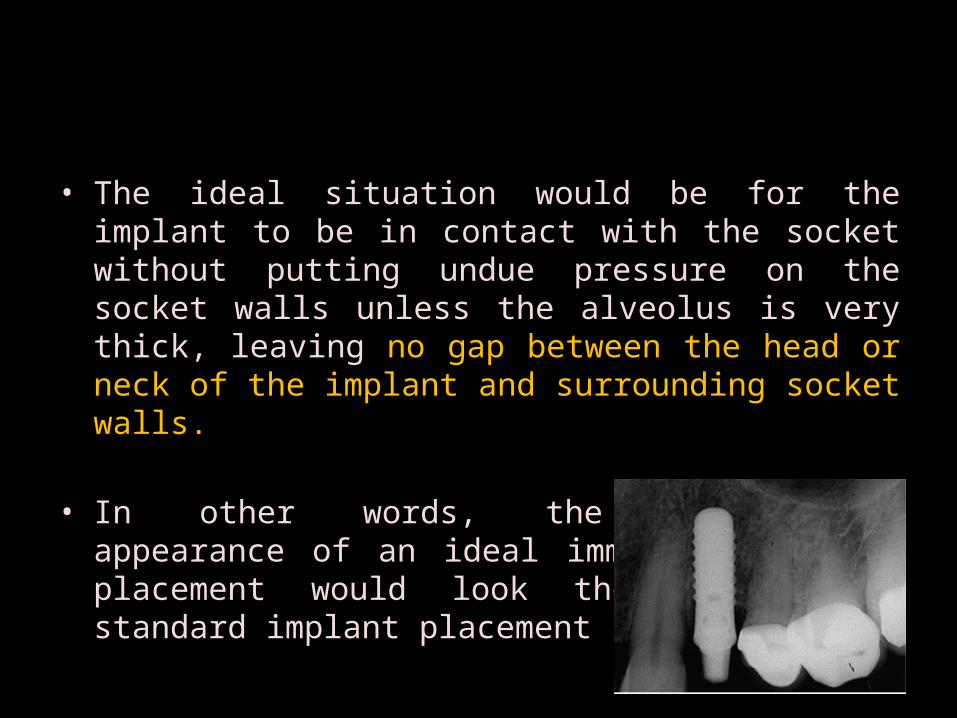
• The ideal situation would be for the implant to be in contact with the socket without putting undue pressure on the socket walls unless the alveolus is very thick, leaving no gap between the head or neck of the implant and surrounding socket walls.
• In other words, the radiographic appearance of an ideal immediate implant placement would look the same as a standard implant placement
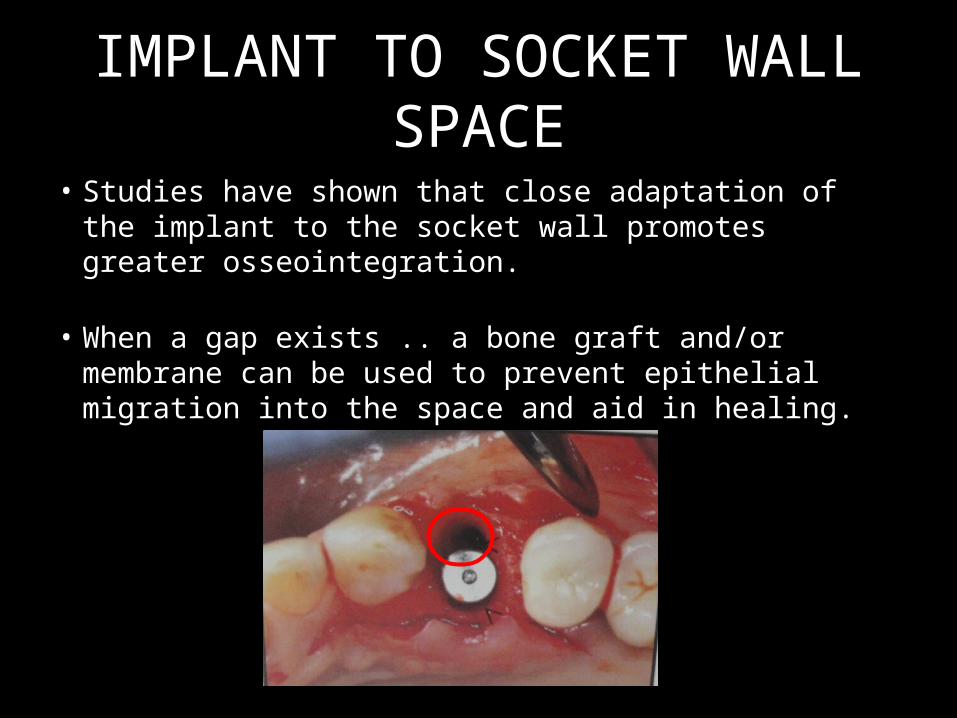
IMPLANT TO SOCKET WALL SPACE
• Studies have shown that close adaptation of the implant to the socket wall promotes greater osseointegration.
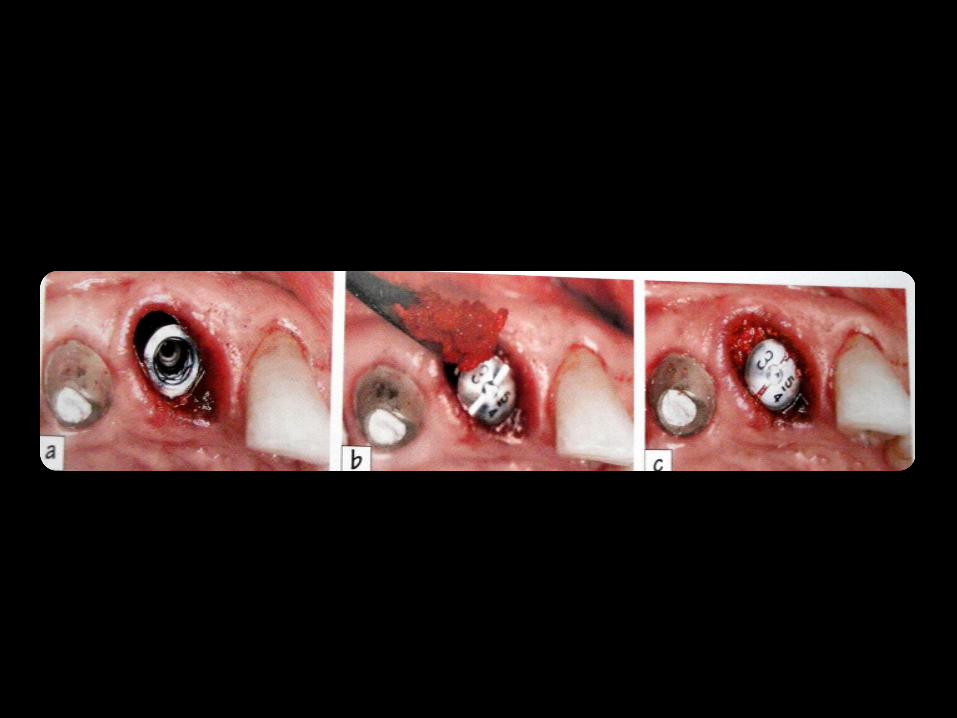
• When a gap exists .. a bone graft and/or membrane can be used to prevent epithelial migration into the space and aid in healing.
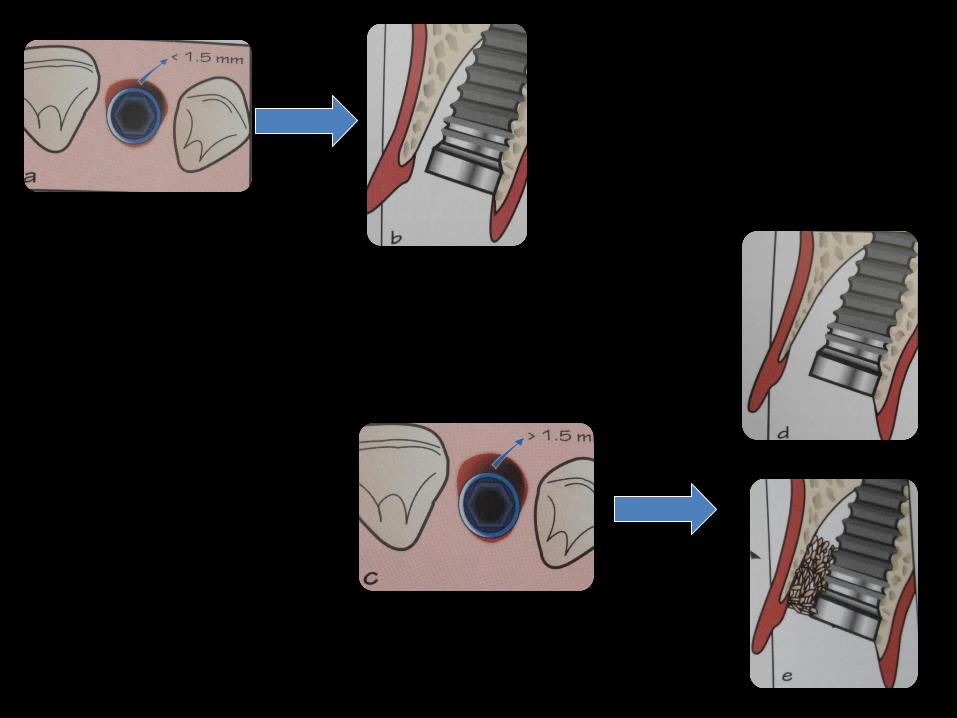
• If all four walls are intact after tooth extraction and the circumferential defect is less than 1.5 mm, an implant may be placed without the need for bone grafting or augmentation.
• Presence of three or more walls or a circumferential defect greater than 1.5 mm can support an immediate implant, but bone grafting and protection of the socket with a membrane is recommended.
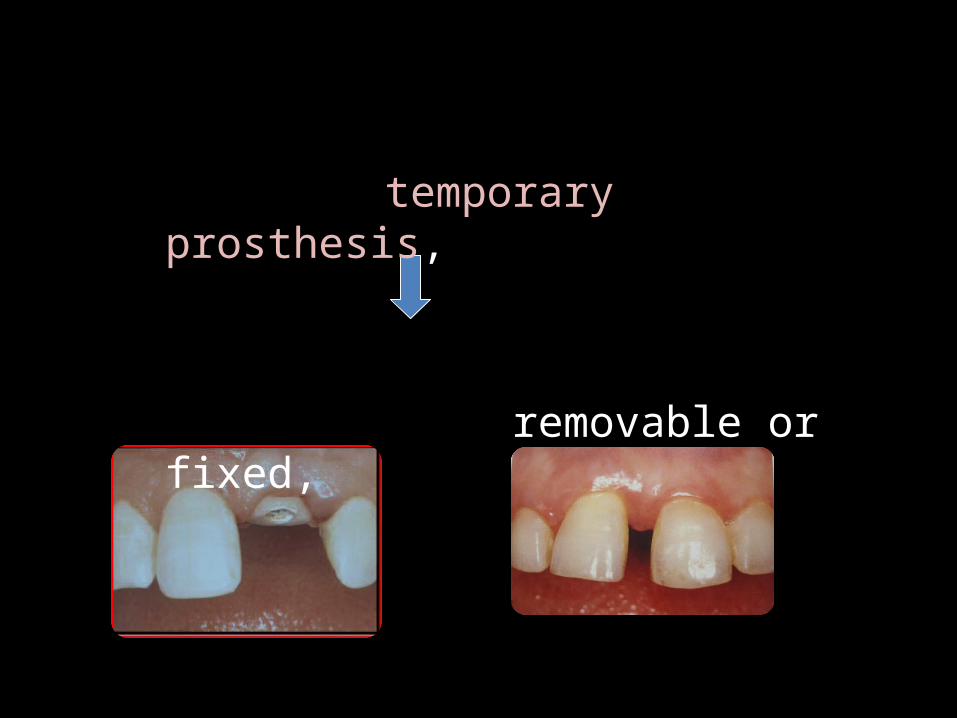
temporary prosthesis,
removable or fixed,
Studies have shown that close adaptation of the implant to the socket wall promotes greater osseointegration.
Bone healing in an implant osteotomy proceeds apical to coronal, much like that of an extraction socket;therefore, the coronal aspect becomes the most critical in the healing. Current research favors the use of an occlusive barrier membrane to protect the healing socket area.
• While immediate implant loading has been shown to be as successful as delayed loading, excessive loading can cause fibrous encapsulation around implants and subsequent failure.
DIFFERENT TREATMENT PROTOCOLS
Standard Protocol (option 1)
One-stage surgery (option 2)
Option 1 + impression at stage
1(option 3)
Immediate loading
(option 5)
One stage surgery + impression at stage 1 surgery
(option 4)
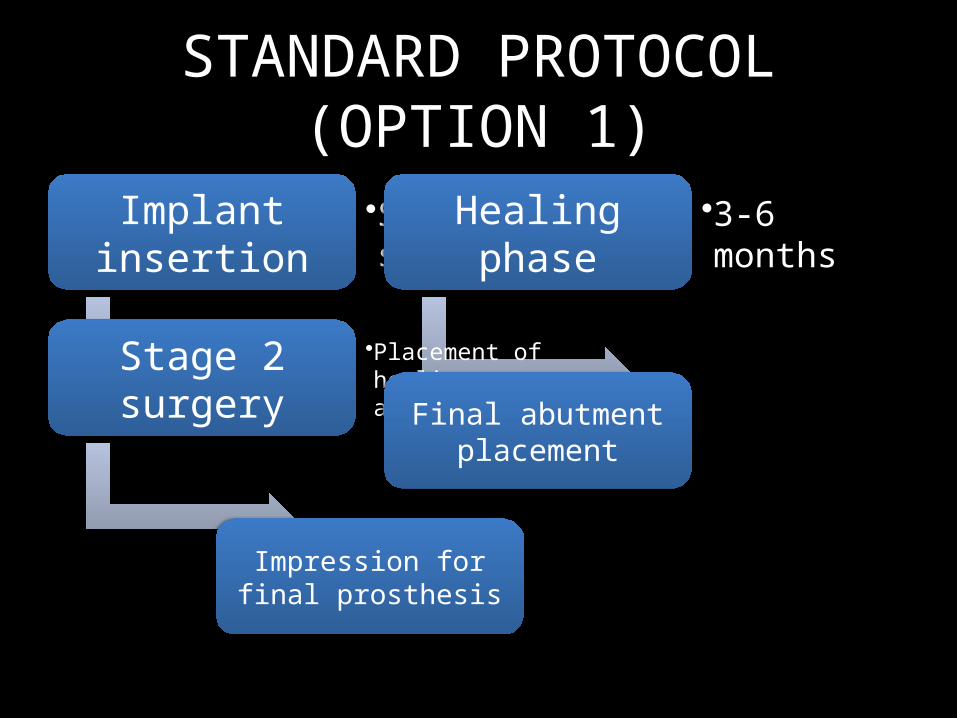
STANDARD PROTOCOL (OPTION 1)
Implant insertion
•Stage 1 surgeryHealing phase •3-6 months
Stage 2 surgery •Placement of healing abutmentFinal abutment
placement
Impression for final prosthesis
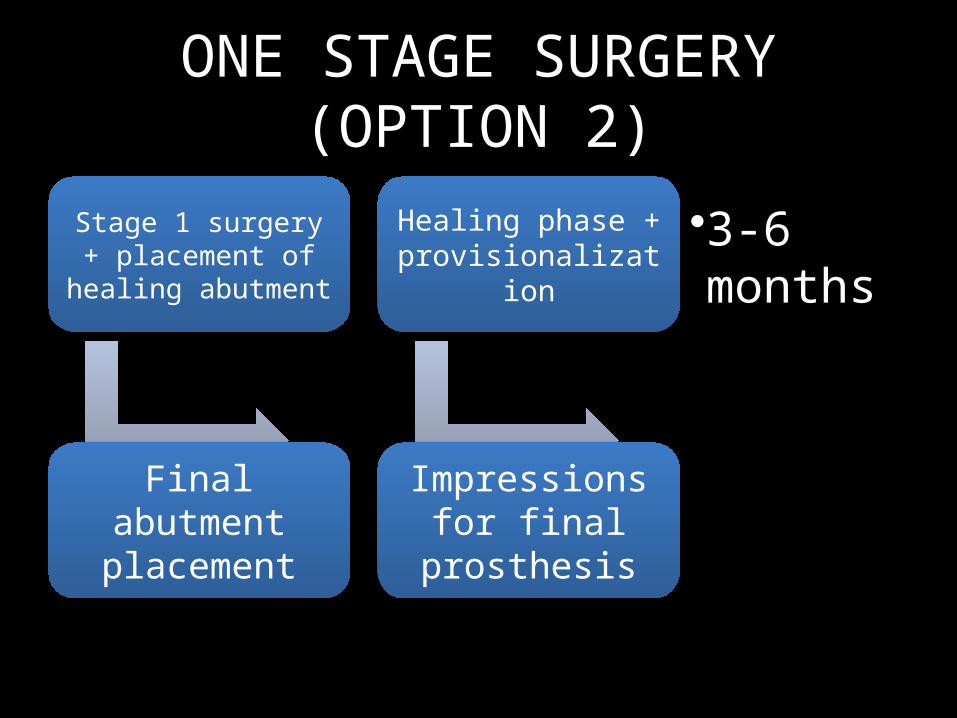
ONE STAGE SURGERY (OPTION 2)
Stage 1 surgery + placement of
healing abutment
Healing phase + provisionalization
•3-6 months
Final abutment placement
Impressions for final prosthesis
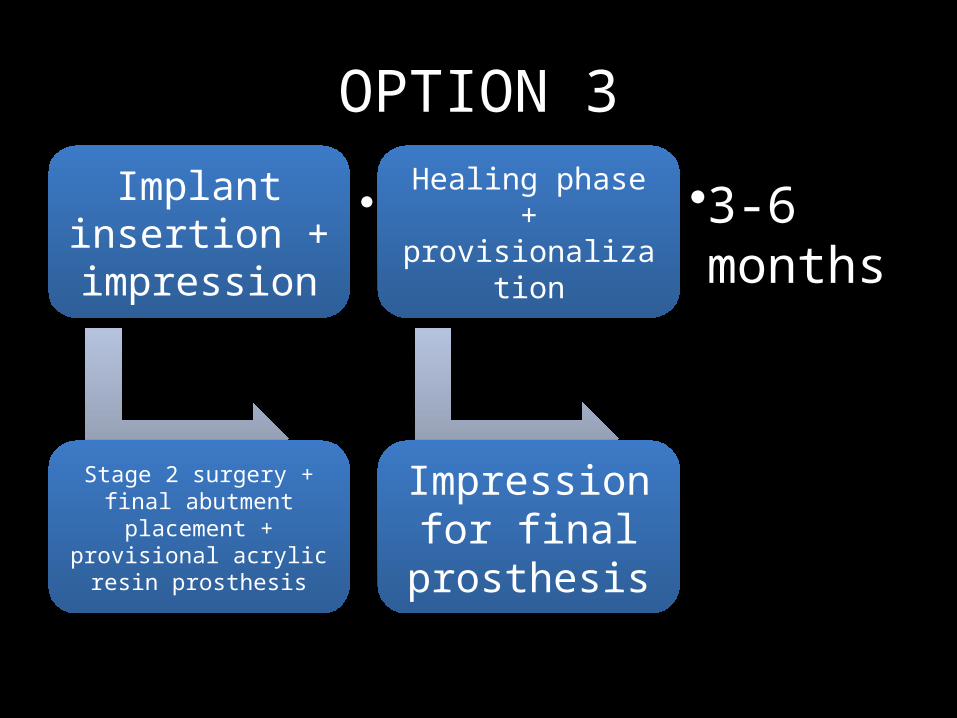
OPTION 3Implant
insertion + impression
•Stage 1 surgery
Healing phase + provisionalizati
on
•3-6 months
Stage 2 surgery + final abutment placement + provisional acrylic
resin prosthesis
Impression for final prosthesis
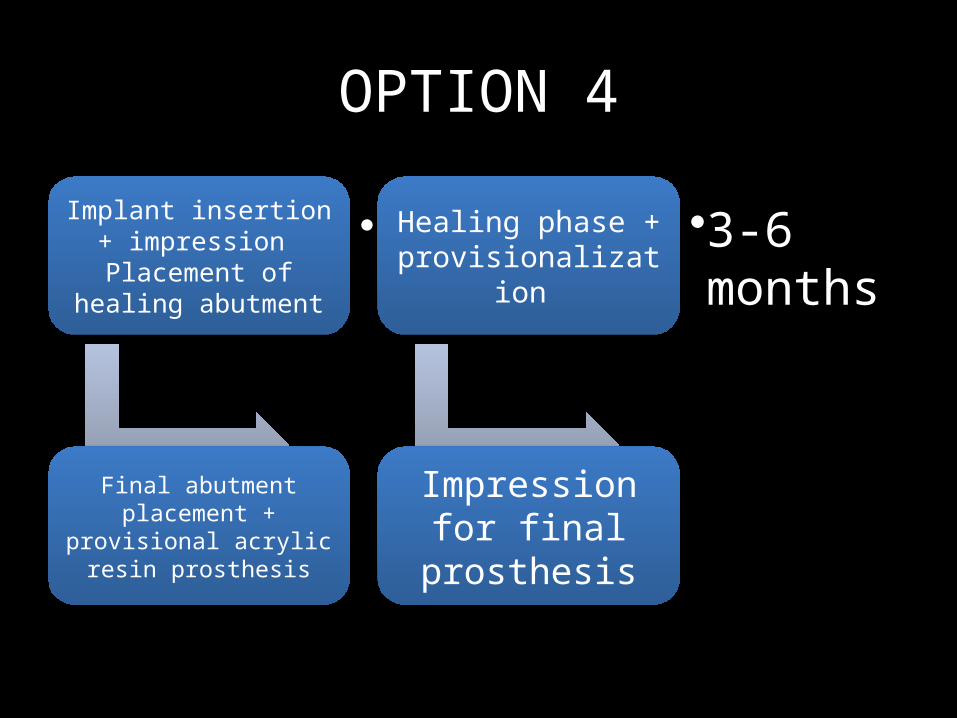
OPTION 4
Implant insertion + impression
Placement of healing abutment
•Stage 1 surgery
Healing phase + provisionalizatio
n
•3-6 months
Final abutment placement +
provisional acrylic resin prosthesis
Impression for final prosthesis
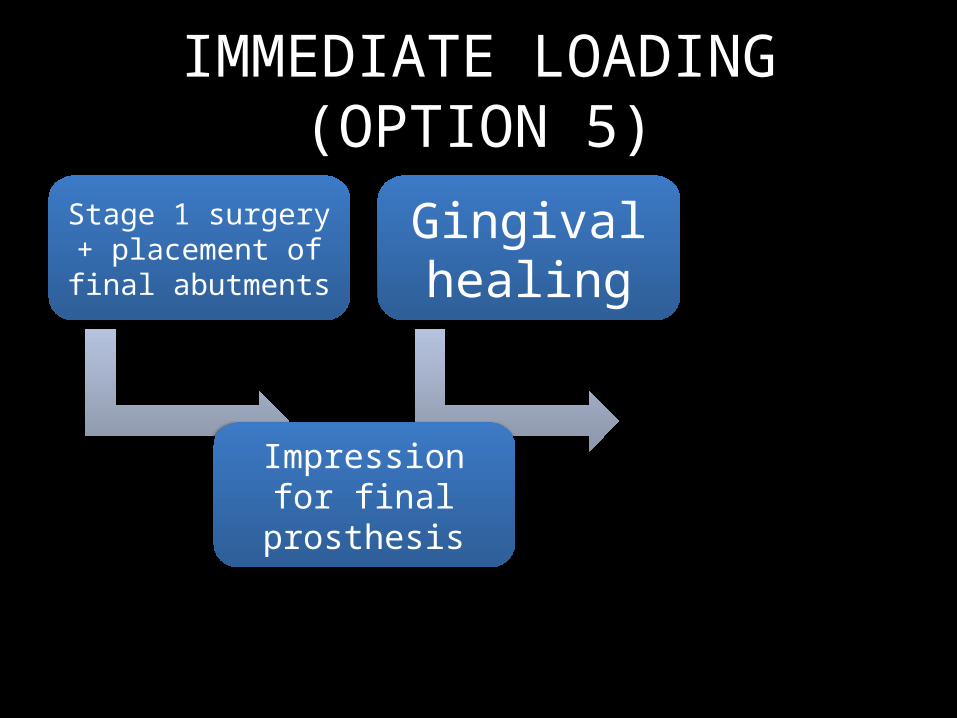
IMMEDIATE LOADING (OPTION 5)
Stage 1 surgery + placement of final
abutments
Gingival healing
Impression for final prosthesis
SOFT TISSUE MANAGEMENT
• One of the most critical factors in implant restorative esthetics is the gingival form.
• can be shaped and managed by the provisional prosthesis and by the provisional crown.
• The use of anatomic gingival formers or single stage implants and the placement of impIants without elevating a flap have significantly improved the clinician's ability to readily achieve excellent peri-implant gingival form.
POST-OP MANAGEMENT
• Antibiotics and analgesics• Oral hygiene and Chlorhexidene mouth wash
recommended
• Covani, Cornelini and Barone (2003)
Study concluded that the coronal bone remodeling around immediate showed a healing pattern with new bone apposition around the necks of the implants and, at the same time, bone resorption with horizontal width reduction of the bone ridge.
• Schropp, Kostopoulo and Wenzel (2003)conducted a study to compare bone healing and crestal bone changes following immediate (Im) versus delayed (De) placement of titanium dental implants
It was concluded that new bone formation occurs in infrabony defects associated with immediately placed implants in extraction sockets.
• Rosa, Rosa, Francischone and Maior (2014)conducted a study to evaluate the stability of esthetic treatment after single tooth replacement in compromised sockets using the immediate dentoalveolar restoration (IDR) concept
The mean mesial and distal papillary heights increased slightly over time. Stable periimplant soft tissues and satisfactory esthetic outcomes were achieved.
DISADVANTAGES
• Additional cost if membranes and grafts are used
• Sometimes may not be able to place implants, tooth ankylosis, fracture of the buccal plate, socket expansion during extraction, or extensive infection(patient should be imformed previosly)
• Difficulty obtaining primary stability
• Inadequate soft tissue coverage
• Difficulty in preparing the osteotomy due to bur movement (chatter) on the walls of the extraction site
Clinical trials • MOST REPORTS ON IIP DESCRIBES:
- Small peri-implant osseous defects result in a gap measurable from the wall of the socket to the surface of the implant
- Horizontal defect dimension (HDD)/ jumping distance
- If HDD is 2mm or less no augmentation is required
- HDD more than 2mm to achieve bone healing, use collagen barrier membrane & implants with a sand blasted & acid etched surface.
• Botticelli et al (2004) strongly indicated that immediate implant placment does not prevent the physiologic modeling/remodeling that occurs in ridge following extraction
The reduction in of the buccal dimension was 1.9mm after 4 months
• Araujo and Lindhe (2005)
After 3 months of healing
• Amount of resorption in edentulous sites was 2.2mm at the end of the study
• Of that of implants was around 2.4mm
• Araujo et al (2006) in 4 weeks of healing :- The buccal and lingual wall had undergone
substantial resorption- Height of the thin buccal wall was also
reduced After 4 – 12 weeks of healing the bone level was more than 2mm apical to the marginal border of the rough implant surface.
CLINICAL FACTORS TO BE CONSIDERED!!
• Primary stability• Adequate implant splinting where appropriate• Provisional restorations that promote splinting and
reduce or control the mechanical load applied to the implant
• Prevention of provisional restoration removal during the recommended period of implant healing
• Incorporation of team approachs and the use of surgical templates
CONCLUSION…..
REFERENCES
• Wilson TG, Buser D, et al. Implants placed in immediate extraction sockets. Int J Oral Maxillofac Implants 1998;13:333-41
• Lazzara RJ. Immediate implant placed into extraction sites – surgical and restorative advantages. Int J Periodontics Restorative Dent 1989;9:333-343
• Parel SM, Triplett RG. Immediate fixture placement. A treatment planning alternative. Int J Oral Maxillofac Implants 1990;5:337-45
• Becker W and Becker BE. Flap designs for minimization of recession adjacent to maxillary anterior implant sites: a clinical study. Int J Oral Maxillofac Implants 1996;11:46-54.
• Villa R and Rangert B. Early loading of inerforaminal implants immediately installed after extraction of teeth presenting endodontic and periodontal lesions. Clin Imp Dent and Related Res 2005;7:S28-S35.
• Langer B and Sullivan DY. Osseointegration: its impact on the interrelationship of periodontics and restorative dentistry. Part 3. Periodontal prosthesis redefined. Int J Periodont Rest Dent 1989;9:240-261.
• Carlsson L, Rostlund T, Albrektsson B and Albrektsson T. Implant fixation improved by close fit. Cylindrical implant-bone interface studied in rabbits. Acta Orthop Scand 1988;59:272-275.
• Botticelli D. The jumping distance revisited. An experimental study in the dog. Clin Oral Implants Res 2003;14:35-42











![Benefits of an immediate tissue-level implant protocol · The immediate implant placement protocol further helps to preserve the natural bone volume [1,2]. De-layed implant placement](https://img.pdfslide.us/doc/110x75/5f38184e0481442629236ad8/benefits-of-an-immediate-tissue-level-implant-protocol-the-immediate-implant-placement.jpg)