Embed Size (px)
Citation preview

Melatonin Agonists to Prevent and Treat ICU associated Delirium:Advancing Practice from Evidence
Base to Clinical Care
Christofer D. Barth, M.D.Director Cardiovascular Critical Care
Aurora Critical Care ServiceAurora St. Luke’s Medical Center

Background: Delirium, Sleep, and Melatonin
• Sleep disruption begins preoperatively and is ubiquitous. Sleep disruption begins prior to surgery and continues on postoperative days 1 and 2.
• Sleep disruption (circadian rhythm disturbances) and delirium appear associated and are common occurrences in the general ICU patient population.
• ICU Delirium adds to length of stay, cost of admission, and risk to mortality.
• Aurora Health Care ‘Delirium Protocol’ means we are starting to make improvements in terms of internal quantification of the Delirium:– However, we still have difficulty monitoring with CAM-ICU scoring system
and Ramsay Sedation Scale.

Background: Delirium, Sleep, and Melatonin• Melatonin is a naturally occurring sleep hormone secreted by the pineal gland
during night conditions (absence of lighting).• Melatonin agonists are clinically indicated for sleep and for disruption of day-night
sleep cycle.• Melatonin agonists:
– Permit and maintain natural REM sleep cycles– Randomized controlled trials(RCT) now demonstrate a large relative risk
reduction for delirium of hospitalized patients.– Melatonin ($0.10/pill): regulated under herbal/natural supplements provisions
and not regulated as a drug by the FDA. Half life ~ 2-3 hours, natural hormone with limited significant side effects.
– Ramelteon ($8/pill): moderate structural modifications to natural melatonin; it is FDA regulated. Half Life is 4-6 hrs, liver metabolism. May have drug interactions accordingly. Rarely causes life threatening angioedema/airway obstruction.
• Historically, we’ve used dexmedetomidine ($50-100/dose + ICU monitoring) or benzodiazepine/zolpidem (increased risk of delirium) in ICU’s.

Interventions: Melatonin Agonists to Prevent and Treat Delirium in ICU
• Prior to the evolution of the RCT evidence base, in the CVICU, we’ve used melatonin successfully at preventing and treating ICU delirium associated with sleep disruption. Also, during daily quality rounds (Outcome Facilitation Rounds) we often identify patients with sleep disruption and discuss therapeutic options.
• Ramelteon was added to the system wide 'Delirium Protocol’, through the Delirium subcommittee, after I directed a hospital level conversation, through the Quality (IHI) subcommittee of the Critical Care Committee, on how to integrate the evolving RCT evidence base of melatonin agonist therapy into our ‘Delirium Protocol’.
• System wide Pharmacy, Nutrition, Therapeutics Committee adopted ramelteon as formulary and melatonin as non-formulary, based on policy to avoid non-FDA regulated therapeutics. I worked with PNT to evaluate the ideal utilization of melatonin versus ramelteon given cost, adverse reactions, and limitations due to non-FDA regulated formulation of melatonin.
• I’ve educated my colleague in a multidisciplinary fashion (CCM, eICU, Geriatrics, Critical Care Nursing) our observed clinical success with melatonin agonists in the CVICU, correlating to RCT evidence base, in treating sleep disruption and preventing ICU delirium.

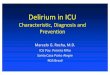
Melatonin Agonist Utilization at Aurora St. Luke’s Medical Center 2014

Melatonin Agonists and Delirium: Conclusions
• This project represented a simple intervention to prevent and treat ICU delirium based on known physiologic disturbance, observed clinical benefits, and correlating RCT evidence base.
• This treatment is simple, anecdotally appears to reduce delirium associated length of stay in the CVICU, reduces the need for nocturnal dexmedetomidine, virtually eliminates the need for nocturnal zolpidem/benzodiazepines, but clearly does not treat all ICU delirium issues.
• This could be expanded throughout the hospital and the system:– It would be anticipated to reduce length of stay, but LOS associated with delirium
would be difficult to quantify in our system.– It could be quantified on the transition away for zolpidem and dexmedetomidine
and toward melatonin agonists therapies.– Melatonin would likely cost less and avoid more harm than ramelteon, based on
the low risk of angioedema and drug interactions, but this would require finding a self regulated melatonin vendor and changing Aurora Health Care policy regarding avoiding non-FDA regulated pharmacotherapies.