Embed Size (px)
Citation preview

Dharam Prakash Saran
1

2
Intra aortic balloon counter pulsation( IABP):
Most common and widely available methods of mechanical circulatory support
Temporary support for the left ventricle by mechanically displacing blood within the aorta
Concepts: - Systolic unloading- Diastolic augmentation
Traditionally used in surgical and non surgical patients with cardiogenic shock

3
Indications for IABP
1. Cardiogenic shock:
2. In association with CABG :
Preoperative insertion- Patients with severe LV dysfunction - Patients with intractable ischemic arrhythmias
Postoperative insertion - Postcardiotomy cardiogenic shock
- Associated with acute MI - Mechanical complications of MI - MR , VSD
3. In association with nonsurgical revascularization:
-Hemodynamically unstable infarct patients-High risk coronary interventions
- severe LV dysfunction, LMCA, complex coronary artery disease
4. Stabilization of cardiac transplant recipient before insertion of VADPost infarction anginaVentricular arrhythmias relathed to ischemia

4

CONTRAINDICATIONSAbsolute-
▫ Significant aortic regurgitation▫ Aortic dissection▫ Aortic stents▫ Bilateral femoral popliteal bypass grafts for severe
PVD
Relative -▫ Abdominal aortic aneurysm▫ Uncontrolled septicemia▫ Uncontrolled bleeding diathesis▫ Severe bilateral peripheral vascular disease

6

7

8
Interpreting IABP waveforms

9
IABP –instrumentation and techniques

10
The IAB Counter pulsation system- two principal parts
A flexible catheter -2 lumen • first - for distal aspiration/flushing or pressure monitoring • second - for the periodic delivery and removal of helium gas to a
closed balloon.
A mobile console • system for helium transfer • computer for control of the inflation and deflation cycle

11

12
Expected changes with IABP support in hemodynamic profile in patients with Cardiogenic shock
- Decrease in SBP by 20 %
- Increase in aortic Diastolic Press. by 30 % ( raise coronary blood flow)
- Increase in MAP
- Reduction of the HR by 20%
-Decrease in the mean PCWP by 20 %
- Elevation in the COP by 20%

13
IABP catheter:
10-20 cm long polyurethane bladder
25cc to 50cc capacity
Optimal 85% of aorta occluded (not 100%)
The shaft of the balloon catheter contains 2 lumens: - one allows for gas exchange from console to
balloon- second lumen
- for catheter delivery over a guide wire - for monitoring of central aortic pressure
after installation.

14
Intra Aortic Balloon

15
Balloon sizing
Sizing based on patients height
Four common balloon sizes
Balloon length and diameter increases with each larger size
40 cm³ balloon is most commonly used
Paediatric balloons also available : sizes 2.5, 5.0, 12.0 and 20 cm³
Balloon size Height
50 cm³ > 6 feet
40 cm³ 5 feet 4 inch
to 6 feet
34 cm³ 5 feet to 5
feet 4 inch
25 cm³ < 5 feet

16
Benefits of larger volume IABs• More blood volume displacement• More diastolic augmentation• More systolic unloading

17
Introducer needle• Guide wire• Vessel dilators• Sheath• IABP (34 or 40cc)• Gas tubing• 60-mL syringe• Three-way stopcock
IABP Kit Contents

18
Connect ECG
Set up pressure lines
Femoral access – followed by insertion of the supplied sheath
0.030 inch supplied J-shaped guide wire to the level of the aortic arch (LAO view)
- IABP insertion

19
Take the entire catheter and T handle as one unit
(DO NOT disconnect one-way valve when removing the extracorporeal tubing from the tray.)
Pull out the T- handle only as shown

20
• Remove stylet/aspirate/Flush
• Insert the balloon only over the guide wire
• Hold the catheter close to skin insertion point
• Advance in small steps of 1 to 2 cm at a time and stop if any resistance.
• The IABP should advance freely
Inserting the Balloon catheter
- Many vascular complications occur during insertion itself
- Resistance during insertion either indicates PVOD, or dissection
- Kinking of IABP » improper inflation/deflation

21
- The end of the balloon should be just distal (1-2 cm) to the takeoff of the left subclavian artery
- Position should be confirmed by fluoroscopy or chest x-ray
Positioning

22
Connecting to console: - Connect helium gas tube to the console via a long extender - Open helium tank.
- The central lumen of the catheter is flushed and connected to pressure tubing with 3 way and then to a pressure transducer to allow for monitoring of central aortic pressure.
- Zero the transducer
Initial set-up:- Once connected properly the console would show ECG and pressure
waveforms.- Check Basal mean pressure- Make sure the setting is at “auto”- Usually IABP started at 1:1 or 1:2 augmentation- Usually Augmentation is kept at maxim

23

24

25
Trigger modesTrigger :
- Event the pump uses to identify the onset of cardiac cycle (systole)- Pump must have consistent trigger in order to provide patient assist- If selected trigger not detected, counter pulsation will interrupted
1.ECG- uses the slope of QR segment to detect triggering point
2. AP(Arterial pressure wave)- Systolic upstroke of the arterial pressure wave form is the trigger

26
ECG signal – most common• Inflation
- middle of T wave• Deflation
– peak of R wave
• Pacer (v/a)
• Arterial waveform
• An intrinsic pump rate (VF, CPB)

27

28

29

30
Increased coronaryperfusion
The “normal” augmented waveform

31
Not all Sub optimal augmentation is due to Timing errors/kinks

32
Factors affecting diastolic augmentation
Patient- Heart rate- Mean arterial pressure- Stroke volume- Systemic vascular resistance
Intra aortic balloon catheter- IAB in sheath- IAB not unfolded- IAB position- Kink in the IAB catheter - IAB leak- Low helium concentration
Intra aortic balloon pump- Timing- Position of IAB augmentation control

33
How to check waveform is acceptable ?
First change from 1:1 to 1:2 augmentation Check the dicrotic notch See if augmentation starts at that point
This should produce a sharp “V” at inflation.

34
How to check waveform is acceptable ?
First change from 1:1 to 1:2 augmentation Check the dicrotic notch See if augmentation starts at that point
This should produce a sharp “V” at inflation. Check if diastolic augmented wave is › systolic wave

35
How to check waveform is acceptable ?
First change from 1:1 to 1:2 augmentation Check the dicrotic notch See if augmentation starts at that point
This should produce a sharp “V” at inflation. Check if diastolic augmented wave is › systolic wave
Confirm if end diastolic wavefollowing the augmented wave is less than an non augmented wave.
Is Deflation slope ok

36

37
Late Inflation Inflation of the IAB markedly after closure of the aortic valve.Waveform Characteristics:
• Inflation of IAB after the dicrotic notch.• Absence of sharp V.• Sub optimal diastolic augmentation

38
Early Deflation Premature deflation of the IAB during the diastolic phase.

39
Late Deflation Late deflation of the IAB during the diastolic phase.
Waveform Characteristics:• Assisted aortic end diastolic pressure may be equal to the
unassisted aortic end diastolic pressure.• Rate of rise of assisted systole is prolonged.• Diastolic augmentation may appear widened

40

41
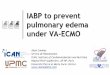
Variation in balloon pressure wave forms
Increased duration ofplateau due to longer
diastolic phase
Decreased durationof plateau due to
shortened diastolicphase

42
Variation in balloon pressure wave forms
Varying R-R intervalsresult in irregularplateau durations

43
Variation in balloon pressure wave forms
Increased heightor amplitude ofthe waveform
Decreased heightor amplitude of thewaveform

44
Variation in balloon pressure wave forms
Gas leak
Leak in the closed system causing theballoon pressure waveform to fall belowzero baseline..
- due to a loose connection- a leak in the IAB catheter- H2O condensation in the external tubing- a patient who is tachycardiac and febrile which causes increased gas
diffusion through the IAB membrane

45
Catheter Kink
Rounded balloon pressure waveform- Loss of plateau resulting from a kink or
obstruction of shuttle gas
- Kink in the catheter tubing- Improper IAB catheter position- Sheath not being pulled back to allow
inflation of the IAB- IAB is too large for the aorta- IAB is not fully unwrapped- H2O condensation in the external tubing

46
“Balloon too large”
syndrome

47
Patient Management During IABP support
Anticoagulation-- maintain apTT at 50 to 70 seconds
CXR daily – to R/O IAB migration
Check lower limb pulses - 2 hourly. - If not palpable » ? - vascular obstruction
- thrombus, embolus, or dissection (urgent surgical consultation)
Prophylactic antibiotics NOT INDICATED
Hip flexion is restricted, and the head of the bed should not beelevated beyond 30°.

48
Never leave in standby by mode for more than 20 minutes > thrombus formation
Daily– Haemoglobin (risk of bleeding or haemolysis)– Platelet count (risk of thrombocytopenia) – Renal function (risk of acute kidney injury secondary to distal
migration of IABP catheter)
Wean off the IABP as early as possible as longer duration is associatedwith higher incidence of limb complications
Patient Management During IABP support

49

50
Weaning of IABP
Timing of weaning:
- Patient should be stable for 12 – 24 hours- Decrease inotropic support- Decrease pump ratio
– From 1:1 to 1:2 or 1:3- Decrease augmentation- Monitor patient closely
– If patient becomes unstable, weaning should beimmediately discontinued

51
IABP Removal
-Discontinue heparin 1 hour prior to removal
-Disconnect the IAB catheter from the IAB pump
- Patient blood pressure will collapse the balloon membrane for withdrawal
- Withdraw the IAB catheter through the introducer sheath until resistance is met.
- NEVER attempt to withdraw the balloon membrane through the introducer sheath.
-Remove the IAB catheter and the introducer sheath as a unit
- Check for adequacy of limb perfusion after hemostasis is achieved.

ACC/AHA 2013Practice Guidelines (ESC
2012- IIb)
52

ESC 2014 GUIDELINES
53

IABP IN UA/NSTEMI (2007, 2012
update)
(Current Practices)(Class IIa LOE-©)
54
The placement of an IABP could be useful in patients with recurrent ischemia despite maximal medical management and in those with hemodynamic instability until coronary angiography and revascularization can be completed.

TRIALS OF IABP
55

Benchmark registry
• n = 17,000( june 1996- aug 2000)
• 203 hospitals- 90% US
• 18.8% of IABP used for cardiogenic shock
• Device related death – 0.5%
• Major complication – 2.6%
• Minor complication – 4.2%
56

Balloon-pump assisted Coronary Intervention
Study (BCIS-1):
• The first randomized controlled trial of elective
Intra-Aortic Balloon Pump (IABP) insertion prior to
high-risk PCI vs. PCI with no planned IABP use
• 17 UK centres
• n=301 (150 in each arm)
57

58IABP in high risk PCI(BCIS-1 TRIAL)
N= 301 Elective IABP(
151)
No elective
IABP(150)
P VALUE
MACE 15.2% 16% 0.85
All cause mortality
at 6 mths
4.6% 7.4% 0.32
Major procedural
complications
1.3% 10.7% <0.001
Major or minor
bleeding
19.2% 11.3% 0.06
Access site
complications
3.3% 0% 0.06
Patients (n = 301) had severe left ventricular dysfunction (ejection fraction ≤ 30%) and extensive coronary disease (Jeopardy Score ≥ 8/12); those with contraindications to or class I indications for IABP therapy were excluded
JAMA. 2010;304(8):867-874

59
Conclusions of long term results of
BCIS1 trial(2012-2013)
In patients with severe ischemic cardiomyopathy treated
with PCI, all cause-mortality was 33% at 51 months
(median)
Elective IABP use during PCI was associated with an
observed 34% reduction in long-term all-cause mortality

60
Counterpulsation Reduces Infarct Size Acute Myocardial Infarction (CRISP AMI) trial.
Intra-aortic balloon pump counterpulsation prior to PCI in patients with ST segment elevation MI without shock does not reduce infarct size as measured by MRI

Shock trial and registry
61

62
N-302 pts
N- 152 pts N- 150 pts

63
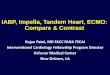
SHOCK Trial
Primary and Secondary Endpoints
0
20
40
60
80
30 Days 6 months
Immediate
Revascularization
Strategy
Medical Stabilization
as an Initial Strategy
Primary Endpoint
Secondary Endpoint
Mo
rta
lity
(%
)
46.7%
56.0% 50.3
%
63.1%
P=.11
P= .027
Hochman et al, NEJM 1999; 341:625.

64
Impact of thrombolysis, intra-aortic balloonpump counterpulsation, and theircombination in cardiogenic shockcomplicating acute myocardial infarction: areport from the SHOCK Trial Registry

65
SHOCK Registry: Impact of Thrombolytics and IABP
0
20
40
60
80
47%
52%%
P<0.0001
63%
77%
Thrombolytics
+ IABP
No Thrombolytics
+ IABP
Thrombolytics
+ No IABP
Neither
Hochman et al, NEJM 1999; 341:625.

66
Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock
IABP Shock II Trial

Conclusion
• The use of intraaortic balloon counterpulsation did not significantly reduce 30-day mortality in patients with cardiogenic shock complicating acute myocardial infarction for whom an early revascularization strategy was planned.
67

MCQs
68

• 1. Major physiological effects of counter pulsation include?
▫ A) increased coronary artery perfusion, increased preload, decreased after load, decreased myocardial oxygen consumption
▫ B) increased coronary artery perfusion, increased preload, increased after load, decreased myocardial oxygen consumption
▫ C) increased coronary artery perfusion, decreased preload,
decreased after load, increased myocardial oxygen consumption
▫ D) increased coronary artery perfusion, decreased preload, decreased after load, decreased myocardial oxygen consumption
69

2. The dicrotic notch on the arterial wave form reflects
A) aortic valve opening
B) aortic valve closure
C) isovolumetric contraction
D)rapid ejection
70

3. Expected changes with IABP support in hemodynamic profile in patients with Cardiogenic shock include all except?
A) Decrease in SBP by 20 %
B) Increase in aortic DP by 30 %
C) Decrease in MAP by 10%
D) Reduction of the HR by 20%
E)Decrease in the mean PCWP by 20 %
71

4. late inflation of the balloon can result in?
A) premature augmentation
B) increased augmentation
C) decreased augmentation
D) increased coronary perfusion
72

5. A rounded balloon pressure wave form indicate?
A) helium leak
B) power failure
C) hypovolemia
D) balloon occluding the aorta
73

6. width of balloon pressure wave form corresponds to
A) length of systole
B) length of diastole
C) arterial pressure
D) helium level
74

7. true statement
a) Dicrotic notch- land mark used to set deflation
b) Deflation is timed to occur during period of isovolumetric contraction
c) Most common trigger used is arterial pressure wave method
d) Internal trigger mode is acceptable to use in a patient with normal sinus rhythm
75

8. true statement
A) pacing spikes are automatically rejected in ECG triggered modes
B) pacing trigger modes can be used in a patient of 50% paced rhythm
C) Varying R-R interval result in regular plateau durations in Balloon pressureWave form
76

9. Identify the tracing abnormality
77

10. Identify the tracing abnormality
78

79

• 1. Major physiological effects of counter pulsation include?
▫ A) increased coronary artery perfusion, increased preload, decreased after load, decreased myocardial oxygen consumption
▫ B) increased coronary artery perfusion, increased preload, increased after load, decreased myocardial oxygen consumption
▫ C) increased coronary artery perfusion, decreased preload,
decreased after load, increased myocardial oxygen consumption
▫ D) increased coronary artery perfusion, decreased preload, decreased after load, decreased myocardial oxygen consumption
80

2. the dicrotic notch on the arterial wave form reflects
A) aortic valve opening
B) aortic valve closure
C) isovolumetric contraction
D)rapid ejection
81

3. Expected changes with IABP support in hemodynamic profile in patients with Cardiogenic shock include all except?
•A) Decrease in SBP by 20 %
•B) Increase in aortic DP by 30 %
•C) Decrease in MAP by 10%
•D) Reduction of the HR by 20%
•E)Decrease in the mean PCWP by 20 %
82

4. late inflation of the balloon can result in?
• A) premature augmentation
• B) increased augmentation
• C) decreased augmentation
• D) increased coronary perfusion
83

5. A rounded balloon pressure wave form indicate?
• A) helium leak
• B) power failure
• C) hypovolemia
• D) balloon occluding the aorta
84

6. width of balloon pressure wave form corresponds to
• A) length of systole
• B) length of diastole
• C) arterial pressure
• D) helium level
85

7. true statement
a) Dicrotic notch- land mark used to set deflation
b) Deflation is timed to occur during period of isovolumetric contraction
c) Most common trigger used is arterial pressure wave method
d) Internal trigger mode is acceptable to use in a patient with normal sinus rhythm
86

8. true statement
A) pacing spikes are automatically rejected in ECG triggered modes
B) pacing trigger modes can be used in a patient of 50% paced rhyth
C) Varying R-R interval result in regular plateau durations in Balloon press. Wave form
87

9.
88

10.
89