Embed Size (px)
DESCRIPTION
Vitrag24 www.medicalgeek.com For PPT, visit below link http://www.medicalgeek.com/lecture-notes/29365-hypothyroidism-presentation.html#post80980
Citation preview

Dr.Vitrag Shah
Second Year Resident
MD, Medicine
GMC,Surat
Hypothyroidism
vitrag24 - www.medicalgeek.com

Introduction According to a projection from various studies on thyroid
disease, it has been estimated that about 42 million people in India suffer from thyroid diseases.
Congenital hypothyroidism is common in India, the disease occurring in 1 out of 2640 neonates.
The prevalence of hypothyroidism was 3.9%
Second only to DM as most common endocrine disorder.
Incidence increases with age.
More common in females.
2-3% of older women.
The term myxedema, formerly used as a synonym for hypothyroidism, refers to the appearance of the skin and subcutaneous tissues in the patient who is in a severely hypothyroid state.
vitrag24 - www.medicalgeek.com

Thyroid Regulation
PLASMA T4 + FT4
HYPOTHALAMUS - TRH
ANT. PITUITARY - TSH
THYROID T4 and T3
PLASMA T3 + FT3
TISSUES FT4 to FT3, rT3
TSH -R
vitrag24 - www.medicalgeek.com

In the Thyroid Gland
There the following 5 steps in the hormonogenesis
1. Trapping of inorganic Iodine from dietary Iodides
2. Activation of Iodine to high valance I2
3. Incorporation of I2 into Tyrosine of Thyroid Globulin
4. Coupling of formed MIT and DIT to form T4 & T3
5. Proteolysis of Thyroglobulin to release T4 & T3
vitrag24 - www.medicalgeek.com

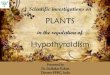
Thyroid hormone biosynthesis
Thyroid hormone synthesis includes the following steps: (1) iodide (I-) trapping by the thyroid follicular cells; (2) diffusion of iodide to the apex of the cells; (3) transport of iodide into the colloid; (4) oxidation of inorganic iodide to iodine and incorporation of iodine into tyrosine residues within thyroglobulin molecules in the colloid; (5) combination of two diiodotyrosine (DIT) molecules to form tetraiodothyronine (thyroxine, T4) or of monoiodotyrosine (MIT) with DIT to form triiodothyronine (T3); (6) uptake of thyroglobulin from the colloid into the follicular cell by endocytosis, fusion of the thyroglobulin with a lysosome, and proteolysis and release of T4, T3, DIT, and MIT; (7) release of T4 and T3 into the circulation; and (8) deiodination of DIT and MIT to yield tyrosine. T3 is also formed from monodeiodination of T4 in the thyroid and in peripheral tissues. Modified from Scientific American Medicine, Scientific American, New York, 1995.
vitrag24 - www.medicalgeek.com

The Thyronines
Mono Iodo Tyrosine – MIT
Di Iodo Tyrosine – DIT
Tri Iodo Thyronine – T3 – half life 6 hours
Tetra Iodo Thyronine – T4 half life 7 days
Reverse T3 - metabolically inactive
T4 is 99.9% protein bound to TBG, TPA, TA
T3 is 99.5% protein bound to TBG, TPA, TA
Bound hormones are inactive – should not be measured
Only Free T4 and Free T3 are metabolically active
vitrag24 - www.medicalgeek.com

The Thyroxines
Tri Iodo Thyronine – T3
- 10% is from thyroid gland
- 90% derived from conversion of T4 to T3
Tetra Iodo Thyronine – T4
- Is exclusively from thyroid gland
From the thyroid gland
- 80% of hormone secreted is T4
- 20% of hormone secreted is T3
vitrag24 - www.medicalgeek.com

Classification of Hypothyroidism Primary hypothyroidism(90%) is characterized by a high
serum thyrotropin (TSH) concentration and a low serum free thyroxine (T4) concentration.
Subclinical hypothyroidism is defined biochemically as a normal free T4 concentration in the presence of an elevated TSH concentration. Other terms for this condition are mild hypothyroidism, early thyroid failure, preclinical hypothyroidism, and decreased thyroid reserve.
Secondary (central) hypothyroidism is characterized by a low serum T4 concentration and a serum TSH concentration that is not appropriately elevated.
Transient or temporary hypothyroidism can be observed as a phase of subacute thyroiditis.
Consumptive hypothyroidism, identified in an increasing number of clinical settings, is the result of accelerated inactivation of thyroid hormone by the type 3 iodothyronine deiodinase (D3).
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

GOITROGENS
DRUGS Anti-thyroid
Cough medicines
Sulfonamides
Lithium
Phenylbutazone
PAS
Oral hypoglycemic agents
vitrag24 - www.medicalgeek.com

GOITROGENS
FOOD Soybeans
Millet
Cassava
Cabbage
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Congenital Hypothyroidism The majority of infants appear normal at birth, and
<10% are diagnosed based on clinical features, which include prolonged jaundice, feeding problems, hypotonia, enlarged tongue, delayed bone maturation, and umbilical hernia.
Importantly, permanent neurologic damage results if treatment is delayed.
Typical features of adult hypothyroidism may also be present.
Other congenital malformations, especially cardiac, are four times more common in congenital hypothyroidism.
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Congenital Hypothyroidism
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Diagnosis & Treatment Because of the severe neurologic consequences of untreated
congenital hypothyroidism, neonatal screening programs have been established based on measurement of TSH or T4 levels in heel-prick blood specimens.
When the diagnosis is confirmed, T4 is instituted at a dose of 10–15 µg/kg per day, and the dose is adjusted by close monitoring of TSH levels.
T4 requirements are relatively great during the first year of life, and a high circulating T4 level is usually needed to normalize TSH.
Early treatment with T4 results in normal IQ levels, but subtle neurodevelopmental abnormalities may occur in those with the most severe hypothyroidism at diagnosis or when treatment is delayed or suboptimal.
vitrag24 - www.medicalgeek.com

Autoimmune Hypothyroidism
Autoimmune hypothyroidism may be associated with a goiter (Hashimoto's, or goitrous thyroiditis) or, at the later stages of the disease, minimal residual thyroid tissue (atrophic thyroiditis).
Because the autoimmune process gradually reduces thyroid function, there is a phase of compensation when normal thyroid hormone levels are maintained by a rise in TSH. Though some patients may have minor symptoms, this state is called subclinical hypothyroidism.
Later, unbound T4 levels fall and TSH levels rise further; symptoms become more readily apparent at this stage (usually TSH >10 mIU/L), which is referred to as clinical hypothyroidism or overt hypothyroidism.
vitrag24 - www.medicalgeek.com

Epidemiology The mean age at diagnosis is 60 years, and the
prevalence of overt hypothyroidism increases with age.
Iodine deficiency is most common cause of hypothyroidism worldwide while Autoimmune hypothyroidism is most common cause in iodine sufficient regions.
vitrag24 - www.medicalgeek.com

Pathogenesis In Hashimoto's thyroiditis, there is a marked
lymphocytic infiltration of the thyroid with germinal center formation, atrophy of the thyroid follicles accompanied by oxyphil metaplasia, absence of colloid, and mild to moderate fibrosis.
In atrophic thyroiditis, the fibrosis is much more extensive, lymphocyte infiltration is less pronounced, and thyroid follicles are almost completely absent. Atrophic thyroiditis likely represents the end stage of Hashimoto's thyroiditis rather than a distinct disorder.
Genetic Associations: HLA-DR (3,4,5) & CTLA-4 (Cytotoxic T Lymphocyte associated antigen 4) polymorphism
Modifying Environmental Factor : Chronic exposure to high iodine diet
No role of infection except Congenital Rubella Syndrome
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Associated conditions Other Autoimmune disorders: (MC) Type 1 diabetes mellitus Addison's disease Pernicious anemia Vitiligo Alopecia areata Celiac disease Dermatitis Herpatiformis Chronic Active Hepatitis RA, SLE, Sjogren syndrome Thyroid associated ophthalmopathy( in 5% of pt)
Turner syndrome, Down’s syndrome
Type 1 or 2 polyglandular autoimmune syndrome
vitrag24 - www.medicalgeek.com

Other causes of hypothyroidism Iatrogenic hypothyroidism is a common cause of
hypothyroidism.
In the first 3–4 months after radioiodine treatment, transient hypothyroidism may occur due to reversible radiation damage. Low-dose thyroxine treatment can be withdrawn if recovery occurs.
Because TSH levels are suppressed by hyperthyroidism, unbound T4 levels are a better measure of thyroid function than TSH in the months following radioiodine treatment.
Mild hypothyroidism after subtotal thyroidectomy may also resolve after several months, as the gland remnant is stimulated by increased TSH levels.
vitrag24 - www.medicalgeek.com

Iodine deficiency is responsible for endemic goiter and cretinism but is an uncommon cause of adult hypothyroidism unless the iodine intake is very low or there are complicating factors, such as the consumption of thiocyanates in cassava or selenium deficiency.
Paradoxically, chronic iodine excess (Rx with amiodarone, lithium) can also induce goiter and hypothyroidism, individuals with autoimmune thyroiditis are especially susceptible.
Secondary hypothyroidism is usually diagnosed in the context of other anterior pituitary hormone deficiencies; isolated TSH deficiency is very rare. TSH levels may be low, normal, or even slightly increased in secondary hypothyroidism; the latter is due to secretion of immunoactive but bioinactive forms of TSH. The diagnosis is confirmed by detecting a low unbound T4 level.
vitrag24 - www.medicalgeek.com

Clinical Manifestations The onset is usually insidious, and the patient may become aware
of symptoms only when euthyroidism is restored. Patients with Hashimoto's thyroiditis may present because of
goiter rather than symptoms of hypothyroidism. The goiter may not be large, but it is usually irregular and firm in consistency.
Hypothyroidism is less prominent clinically and better tolerated when there is a gradual loss of thyroid function (as in most cases of primary hypothyroidism) than when it develops acutely after thyroidectomy or abrupt withdrawal of exogenous thyroid hormone.
The symptoms of central hypothyroidism are usually milder & less obvious than in primary hypothyroidism because of concurrent symptoms of coexisting hormone deficiencies. i.e. hot flashes due to hypogonadism may mask the cold intolerance of hypothyroidism.
When hypothyroidism follows treatment of Graves' hyperthyroidism, some manifestations of Graves' disease, such as ophthalmopathy and vitiligo, may persist throughout the patient's life. vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Differentian between Primary & secondary hypothyroidism
Features Primary Secondary
Skin Thick, without wrinkles Thin with fine wrinkles
Hair Coarse Fine
Menstrual disturbances Menorrhagia Amenorrhea
Secondary sexual characteristics
Normal Poor
Heart size May be enlarged Normal
Goiter May be present Absent
Soft tissue edema Marked Absent
BP Normal/High Low
Cholesterol Increased Normal
TSH High Low
Plasma Cortisol Normal Low
TRH stimulation test Exaggerated response No response
Thyroid Autoantibodies May be present Absent vitrag24 - www.medicalgeek.com

CLINICAL MANIFESTATIONS
Many of the manifestations of hypothyroidism reflect one of two changes induced by lack of thyroid hormone:
A generalized slowing of metabolic processes. This can lead to abnormalities such as fatigue, slow movement and slow speech, cold intolerance, constipation, weight gain (but not morbid obesity), delayed relaxation of deep tendon reflexes, and bradycardia.
Accumulation of matrix glycosaminoglycans in the interstitial spaces of many tissues. This can lead to coarse hair and skin, puffy facies, enlargement of the tongue, and hoarseness. These changes are often more easily recognized in young patients, and they may be attributed to aging in older patients.
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

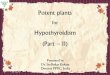
Skin
The skin is cool and pale in patients with hypothyroidism because of decreased blood flow.
The epidermis has an atrophied cellular layer and hyperkeratosis that results in the characteristic dry roughness of the skin.
Sweating is decreased because of decreases in calorigenesis and acinar gland secretion.
A yellowish tinge may be present if the patient has carotenemia, while hyperpigmentation may be seen when primary hypothyroidism is associated with primary adrenal failure
Hair may be coarse, hair loss is common, and the nails become brittle.
Nonpitting edema (myxedema) occurs in severe hypothyroidism and may be generalized. It results from infiltration of the skin with glycosaminoglycans with associated water retention.
Vitiligo and alopecia areata may be present in patients with hypothyroidism after treatment of Graves‘ hyperthyroidism. vitrag24 - www.medicalgeek.com

Myxoedema with Carotineamia
vitrag24 - www.medicalgeek.com

Eyes Periorbital edema
Thinning of outer third of eyebrows (Madarosis)
Graves' ophthalmopathy may persist when hypothyroidism develops after treatment of Graves' hyperthyroidism
vitrag24 - www.medicalgeek.com

Hematologic Decrease in red blood cell mass
Normochromic, normocytic hypoproliferative anemia
Pernicious anemia occurs in 10 percent of patients with hypothyroidism caused by chronic autoimmune thyroiditis : macrocytic anemia with marrow megaloblastosis
Women in the childbearing years may develop iron deficiency anemia, secondary to menorrhagia. In patients with IDA and hypothyroidism, combined therapy with levothyroxine and oral iron supplements results in correction of the anemia, which may be refractory to treatment with iron alone
vitrag24 - www.medicalgeek.com

Cardiovascular system Decrease in cardiac output that is mediated by reductions in
heart rate and contractility Thyroid hormoneregulation of genes coding for specific
myocardial enzymes involved in myocardial contractility and relaxation is responsible for the decrease in contractility.
Reduced cardiac output probably contributes to decreased exercise capacity and shortness of breath during exercise.
Pericardial effusion Hypercholesterolemia, which is caused by a decrease in the
rate of cholesterol metabolism Hyperhomocystemia Diastolic Hypertension, because of an increase in peripheral
vascular resistance. In normotensive patients, blood pressure increases are small (<150/100).
ECG : Low voltage, sinus bradycardia, non-specific ST-T changes
vitrag24 - www.medicalgeek.com

Respiratory system Fatigue, shortness of breath on exertion, rhinitis,
and decreased exercise capacity
Hypoventilation occurs because of respiratory muscle weakness and reduced pulmonary responses to hypoxia and hypercapnia
Sleep apnea occurs in some patients with hypothyroidism, mostly as a result of macroglossia.
vitrag24 - www.medicalgeek.com

Gastrointestinal disorders Decreased gut motility results in constipation
Decreased taste sensation.
Gastric atrophy due to the presence of antiparietal cell antibodies
Celiac disease is four times more common in hypothyroid patients
Modest weight gain (despite poor appetite)due to decreased metabolic rate and accumulation of fluid
Ascites is a rare finding
vitrag24 - www.medicalgeek.com

Reproductive abnormalities Decreased fertility
Early abortion
Hypermenorrhea-menorrhagia (More common). Or oligo- or amenorrhea (later stage)
Low serum sex hormone-binding globulin concentration
Hyperprolactinemia may occur, and is occasionally sufficiently severe to cause amenorrhea or galactorrhea
Decreased libido, erectile dysfunction
vitrag24 - www.medicalgeek.com

Neurological dysfunction Affects both CNS & PNS
Slow growth and delayed facial maturation, delayed appearance of permanent teeth
Myopathy, with muscle swelling, is more common in children than in adults.
In most cases, puberty is delayed, but precocious puberty sometimes occurs
Intellectual impairment if the onset is before 3 years and the hormone deficiency is severe.
Carpal tunnel and other entrapment syndromes
Slow relaxation of tendon reflexes and pseudomyotonia
Memory and concentration are impaired, Bradylalia
Rare neurologic problems include reversible cerebellar ataxia, dementia, psychosis, and myxedema coma. vitrag24 - www.medicalgeek.com

Hashimoto's encephalopathy Hashimoto's encephalopathy has been defined as a
steroid-responsive syndrome associated with TPO antibodies, myoclonus, and slow-wave activity on electroencephalography.
Hashimoto's encephalopathy is believed to be an immune-mediated disorder rather than representing the direct effect of an altered thyroid state on the central nervous system.
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Musculoskeletal symptoms Joint pains, aches, and stiffness
Increased prevalence of hyperuricemia and gout
Elevated AST, CK, LDH
vitrag24 - www.medicalgeek.com

Metabolic abnormalities Hyponatremia may result from a reduction in free
water clearance. Hypothyroidism must be excluded in any hyponatremic patient before making the diagnosis of the syndrome of inappropriate antidiuretic hormone secretion.
Reversible increases in serum creatinine
Hypercholesterolemia and hypertriglyceridemia
Hyperhomocysteinemia
vitrag24 - www.medicalgeek.com

Drug clearance The clearance of many drugs, including
antiepileptic, anticoagulant, hypnotic and opioid drugs, is decreased in hypothyroidism
vitrag24 - www.medicalgeek.com

Myxedema coma Myxedema coma is defined as severe hypothyroidism leading to
decreased mental status, hypothermia, and other symptoms related to slowing of function in multiple organs.
It is a medical emergency with a high mortality rate.
There may be a history of treated hypothyroidism with poor compliance, or the patient may be previously undiagnosed.
Myxedema coma almost always occurs in the elderly and is usually precipitated by factors that impair respiration, such as drugs (especially sedatives, anesthetics, antidepressants), pneumonia, congestive heart failure, myocardial infarction, gastrointestinal bleeding, or cerebrovascular accidents, sepsis.
Hypoventilation leading to hypoxia and hypercapnia, plays a major role in pathogenesis;
Exposure to cold, Hypoglycemia and dilutional hyponatremia also contribute to the development of myxedema coma.
The diagnosis should be considered in any patient with coma or depressed mental status who also has hypothermia, hyponatremia, and/or hypercapnia. Additional clues to the possible presence of myxedema coma in a poorly responsive patient are the presence of a thyroidectomy scar or a history of I-131 therapy or hypothyroidism.
vitrag24 - www.medicalgeek.com

Lab Evaluation Thyroid Function Tests
Total T4 (thyroxine), Total T3 (triiodothyronine)
Free T4 , Free T3
TSH
T3 -Uptake
Free T4 Index, Free T3 Index
Anti-Thyroid Antibodies
Nuclear Scintigraphy
FNAC of nodule
vitrag24 - www.medicalgeek.com

Thyroid Antibodies
Anti Microsomal (TM ) Antibodies
Anti Thyroglobulin (TG) Antibodies
Anti Thyroperoxidase (TPO) Ab
Anti Thyroxine antibodies
Thyroid Stimulating (TSA) Antibodies
High titres TPO Ab in Hashimoto’s & Reidle’s thyroiditis
Anti thyroxine Ab in peripheral resistance to Thyroxine
TSA (TSI) in Graves’ Hyperthyroidism
vitrag24 - www.medicalgeek.com

Tests of thyroid function Test Reference Ranges*
TSH 0.3- 4.0 mU/ L
Free T4 0.7- 2.1 ng/ dL
T4 4- 11 μg/ dL
T3 75- 175 ng/ dl
Adopted from: Stockigt JR . In : Werner and Ingbar’s The Thyroid , 7th ed . 1996: 399 *Reference ranges may vary according to laboratory Tests
Laboratory tests of thyroid function can be abnormal in 70% of hospitalized patients and in up to 90% of critically ill patients. In most cases, the abnormality represents an adaptive response to non-thyroidal (systemic) illness and is not a sign of pathologic thyroid disease.
vitrag24 - www.medicalgeek.com

Thyroxine (T4) and Triiodothyronine (T3) Thyroxine (T4) is the principal hormone secreted by the
thyroid gland, but the active form is triiodothyronine (T3), which is formed by deiodination of thyroxine in extrathyroidal tissues.
Both T3 and T4 are extensively (.99%) bound to plasma proteins, especially thyroxine-binding globulin.
Approximately 0.2% of the total T3 is in the unbound or physiologically active form.
Because of the minor representation of unbound T3 and T4 in plasma, and the potential for plasma protein concentrations to vary in ICU patients, only measurements of free T3 and T4 should be performed in ICU patients.
vitrag24 - www.medicalgeek.com

What tests should I order ?
As per the Guidelines of the AACE and ATA, ITS
1. TSH alone if Hypothyroidism is suspected
2. TSH and Free T4 only if Hyperthyroidism is
suspected or for routine evaluation
3. Free T3 if T3 toxicosis is suspected
4. For follow-up of treatment only TSH
5. Don’t order for Total T4 or Total T3
6. Never order RIU in pregnancy or lactation
vitrag24 - www.medicalgeek.com

1. Depends on the method of estimation of hormones
2. Equilibrium Dialysis is the gold Standard for TSH
3. Radio-immuno assay - 3rd or 4th gen. RIA is the best
4. Reliability of ELISA is not adequate
5. Chemiluminescence immuno assay - CIA is the gold
standard for FT4 but expensive and less widely
available
Choose a lab which offers 3rd or 4th generation RIA method
Which Lab to choose ?
vitrag24 - www.medicalgeek.com

Indications to test for hypothyroidism Clinical symptoms and signs
Fatigue
Cold intolerance
Constipation
Impaired memory
Slowed mental processing
Depression
Nerve entrapment syndromes
Ataxia
Muscle weakness
Muscle cramps
Menstrual disturbance
Infertility
Bradycardia
Diastolic hypertension
Hoarseness
Goitre
Periorbital oedema
Weight gain
Galactorrhoea
Laboratory test abnormalities
Hypercholesterolaemia
Hyponatraemia
Hyperprolactinaemia
Hyperhomocysteinaemia
Anemia
Creatine phosphokinase elevation
Radiological abnormalities
Pericardial and pleural effusions
Pituitary gland enlargement
vitrag24 - www.medicalgeek.com

Indications to test for hypothyroidism
Autoimmune thyroiditis
Established serological or tissue diagnosis
Diffuse goitre
Previous Graves' disease, de Quervain's thyroiditis, or painless (postpartum) thyroiditis
Family history of autoimmune thyroid disease
Down's syndrome
Personal or family history of associated autoimmune disorders (eg, vitiligo, pernicious anaemia, adrenal insufficiency, diabetes mellitus type 1, ovarian failure, coeliac disease, Sjögren's syndrome)
Primary pulmonary hypertension
Multiple Sclerosis
Risk factors for hypothyroidism
Previous thyroid injury
Thyroidectomy or other neck surgery
Radioactive iodine therapy
External radiotherapy
Exposure to polybrominated and polychlorinated biphenyls, and resorcinol
Postpartum status
Drugs impairing thyroid function
Lithium carbonate
Amiodarone
Aminoglutethimide
Interferon α
Thalidomide
Betaroxine
Stavudine
Hypothalamic disorders
Pituitary disorders vitrag24 - www.medicalgeek.com

The Nine Square Game
To evaluate our Thyroid patient
As per the AACE and ITS Guidelines
How to interpret results ?
vitrag24 - www.medicalgeek.com

LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
FR
EE
T
HY
RO
XIN
E
or
FT
4
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
EUTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
PRIMARY
HYPOTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
PRIMARY
HYPERTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
SECONDARY
HYPOTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
SECONDARY
HYPERTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
SUB-CLINICAL
HYPERTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
SUB-CLINICAL
HYPOTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
NON THYROID
ILLNESS or NTI
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
NTI or Pt.
on ELTROXIN
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

FR
EE
T
HY
RO
XIN
E
or
FT
4
EUTHYROID SUB-CLINICAL
HYPERTHYROID
NON THYROID
ILLNESS - NTI
NTI or Pt.
on ELTROXIN
SUB-CLINICAL
HYPOTHYROID
SECONDARY
HYPERTHYROID
SECONDARY
HYPOTHYROID
PRIMARY
HYPERTHYROID
PRIMARY
HYPOTHYROID
LOW NORMAL HIGH
THYROID STIMULATING HORMONE - TSH
BASIC THYROID EVALUATION
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Common Patterns of Thyroid Function Tests in Critically Ill Patients
Non-Thyroidal Ilness Free T4 Free T3 TSH
Early systemic illness Normal ↓ Normal
Early critical illness ↓ ↓ Normal
Chronic critical illness (>2 days)
↓ ↓ Normal/↓
Sick Euthyroid Syndrome
Euthyroid sick syndrome, sick euthyroid syndrome, non-thyroidal illness syndrome or low T3 low T4 syndrome is a state of adaptation or dysregulation of thyrotropic feedback control where the levels of T3 and/or T4 are at unusual levels, but the thyroid gland does not appear to be dysfunctional. This condition is often seen in starvation, critical illness or patients in intensive care unit. vitrag24 - www.medicalgeek.com

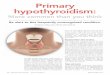
T.F.T. in Progressive Hypothyroidism
TSH
Moderate Severe Mild
Normal Range
Free T4
Free T3
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Algorithm for Hypothyroidism
Measure TSH
Elevated TSH Normal TSH
Measure FT4 Considering Pituitary
Normal Low No Yes
Sub-clinical hypo
TPO + TPO -
T4 repl Annual FU
Primary hypothyroid
TPO + TPO -
No tests Measure FT4
Low Normal
No tests Evaluate Pituitary
Sick Euthyroid
Drugs effect
Hashimoto
Others vitrag24 - www.medicalgeek.com

Treatment Goal : Normalize TSH level regardless of cause of
hypothyroidism
Treatment of choice is thyroxine
Brand consistency recommended
Not recommended for routine use : Desiccated thyroid hormone
Combination of thyroid hormones
T3
TSH should be measured at 6 to 8 weeks after any change in L-thyroxine brand or dose
vitrag24 - www.medicalgeek.com

Determinants of Thyroxine Requirements
Age
Severity and duration of hypothyroidism
Weight
Malabsorption
Pregnancy
Presence of cardiac disease
Concomitant drug therapy
vitrag24 - www.medicalgeek.com

Treatment : Outline Goal : normalize TSH level, , ideally in the lower half of
the reference range.
Single daily dose of levothyroxine as half life is 7 days.
Always take on empty stomach
Starting dose for healthy patients <50 years should be at 1.6 μg/kg/day
Starting dose for healthy patients >50 years should be <50 μg/day. Dose should be increased by 12.5-25 μg/day, if needed, at 6 to 8 weeks intervals. (Start low and go slow)
Starting dose for patients with heart disease should be 12.5 to 25 μg/day and increase by 12.5 to 25 μg/day, if needed, at 6 to 8 weeks intervals
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com

Treatment : Clinical Hypothyroidism If there is no residual thyroid function, the daily replacement dose
of levothyroxine is usually 1.6 µg/kg body weight (typically 100–150 µg). In many patients, however, lower doses suffice until residual thyroid tissue is destroyed.
In patients who develop hypothyroidism after the treatment of Graves' disease, there is often underlying autonomous function, necessitating lower replacement doses (typically 75–125 µg/d).
TSH responses are gradual and should be measured about two months after instituting treatment or after any subsequent change in levothyroxine dosage.
The clinical effects of levothyroxine replacement are slow to appear. Patients may not experience full relief from symptoms until 3–6 months after normal TSH levels are restored.
Adjustment of levothyroxine dosage is made in 12.5- or 25 µg increments if the TSH is high; decrements of the same magnitude should be made if the TSH is suppressed.
Once full replacement is achieved and TSH levels are stable, follow-up measurement of TSH is recommended at annual intervals and may be extended to every 2–3 years if a normal TSH is maintained over several years.
vitrag24 - www.medicalgeek.com

Follow-up After 6 to 8 Weeks of Thyroxine Therapy
If Repeat TSH is Then
> 4.0 mU/L Increase daily thyroxine dose by 12.5-25 μg/d & repeat TSH in 6 to 8 week
0.3 to 4.0 mU/L Continue dose; repeat TSH in 6 months and then annually or if symptomatic If TSH remain normal for several years, then monitor every 2-3 years
<0.4 mU/L Decrease daily thyroxine dose by 12.5 to 25 μg/d and repeat in 6 to 8 weeks
vitrag24 - www.medicalgeek.com

There is no place for liothyronine alone as long-term replacement, because the short half-life necessitates three or four daily doses and is associated with fluctuating T3 levels.
It is important to ensure ongoing adherence, however, as patients do not feel any symptomatic difference after missing a few doses of levothyroxine, and this sometimes leads to self-discontinuation.
In patients of normal body weight who are taking 200 µg of levothyroxine per day, an elevated TSH level is often a sign of poor adherence to treatment. Such patients often have normal or high unbound T4 levels, despite an elevated TSH, because they remember to take medication for a few days before testing; this is sufficient to normalize T4, but not TSH levels.
Because T4 has a long half-life (7 days), patients who miss a dose can be advised to take two doses of the skipped tablets at once. vitrag24 - www.medicalgeek.com

Over - and Under-Replacement Risks Over-replacement Risks
Reduced bone density/osteoporosis
Tachycardia, arrhythmia : Atrial fibrillation
In elderly or patients with heart disease, angina, arrhythmia, or myocardial infarction
Under-replacement Risks
Continued hypothyroid state
Long-term end-organ effects of hypothyroidism
Increased risk of hyperlipidemia
vitrag24 - www.medicalgeek.com

Recovery after L-Thyroxine
vitrag24 - www.medicalgeek.com

Recovery after L-Thyroxine
vitrag24 - www.medicalgeek.com

Treatment : Subclinical Hypothyroidism By definition, subclinical hypothyroidism refers to
biochemical evidence of thyroid hormone deficiency in patients who have few or no apparent clinical features of hypothyroidism.
Routine treatment not recommended when TSH levels are below 10 mU/L.
Any elevation of TSH must be sustained over a 3-month period before treatment is given.
Treatment is administered by starting with a low dose of levothyroxine (25–50 µg/d) with the goal of normalizing TSH. If thyroxine is not given, thyroid function should be evaluated annually.
There is a risk that patients will progress to overt hypothyroidism, particularly when the TSH level is elevated and TPO antibodies are present. vitrag24 - www.medicalgeek.com

Special Treatment Considerations Women with a history or high risk of hypothyroidism should
ensure that they are euthyroid prior to conception and during early pregnancy as maternal hypothyroidism may adversely affect fetal neural development and cause preterm delivery.
Thyroid function should be evaluated immediately after pregnancy is confirmed and at the beginning of the second and third trimesters. The dose of levothyroxine may need to be increased by 50% during pregnancy and returned to previous levels after delivery.
Elderly patients may require 20% less thyroxine than younger patients. In the elderly, especially patients with known coronary artery disease, the starting dose of levothyroxine is 12.5–25 µg/d with similar increments every 2–3 months until TSH is normalized. In some patients, it may be impossible to achieve full replacement despite optimal antianginal treatment.
Emergency surgery is generally safe in patients with untreated hypothyroidism, although routine surgery in a hypothyroid patient should be deferred until euthyroidism is achieved.
vitrag24 - www.medicalgeek.com

Treatment : Myxedema coma Levothyroxine can initially be administered as a single IV
bolus of 500 µg, which serves as a loading dose. Although further levothyroxine is not strictly necessary for several days, it is usually continued at a dose of 50–100 µg/d.
If suitable IV preparation is not available, the same initial dose of levothyroxine can be given by nasogastric tube (though absorption may be impaired in myxedema).
An alternative is to give liothyronine (T3) intravenously or via nasogastric tube, in doses ranging from 10 to 25 µg every 8–12 h. This treatment has been advocated because T4 to T3 conversion is impaired in myxedema coma. However, excess liothyronine has the potential to provoke arrhythmias.
Another option is to combine levothyroxine (200 µg) and liothyronine (25 µg) as a single, initial IV bolus followed by daily treatment with levothyroxine (50–100 µg/d) and liothyronine (10 µg every 8 h).
Recovery within 24 hours is usual.
vitrag24 - www.medicalgeek.com

Supportive Treatment : Myxedema coma External warming is indicated only if the temperature is <30°C,
as it can result in cardiovascular collapse. Space blankets should be used to prevent further heat loss.
Parenteral hydrocortisone (50 mg every 6 h) should be administered, because there is impaired adrenal reserve in profound hypothyroidism.
Any precipitating factors should be treated, including the early use of broad-spectrum antibiotics, pending the exclusion of infection.
Ventilatory support with regular blood gas analysis is usually needed during the first 48 hours.
Hypertonic saline or IV glucose may be needed if there is severe hyponatremia or hypoglycemia; hypotonic IV fluids should be avoided because they may exacerbate water retention secondary to reduced renal perfusion and inappropriate vasopressin secretion.
The metabolism of most medications is impaired, and sedatives should be avoided if possible or used in reduced doses. Medication blood levels should be monitored, when available, to guide dosage. vitrag24 - www.medicalgeek.com

Diet in Iodine deficiency
Iodized salt
Selenium supplementation
Avoid Cassava
Avoid cabbage (goitrogens)
Avoid formula milk
Fish, meat, milk & eggs
vitrag24 - www.medicalgeek.com

References Williams Textbook of Endocrinology – 12th Edition
Harrison’s Principles of internal medicine – 18th Edition
AFP journal
UpToDate 19.3
eMedicine
Publications from the American Thyroid
Association, American Association of Clinical
Endocrinologists, and the Endocrine Society
The ICU Book, 3rd Edition - Paul L. Marino
vitrag24 - www.medicalgeek.com

vitrag24 - www.medicalgeek.com