Embed Size (px)
Citation preview

HOW READ CHEST XR -10
ANAS SAHLE ,MD

Brief review

PATCHY
INFILTIRATION
NODULE
MASS
CAVITARY
OPACITY

Consolidation
Infection causes
Pneumonia
Non-infection causes
Lymphoma
Broncho-
alveolar
carcinoma
COP
WEGNER disease
Sarcoi
d
Cardiac failu
re

Solitary Pulmonary Nodule(SPN)
Comparison with a previous x-ray toAssess growth over time.

Cavitary lesion
Air + tissue
Air-fluid level
StraightAbscess
Wavy ruptured
Hydatid cyst
Air only
ThickIrregular
inner wall
Cavitating
neoplasm
Regular
inner wall
Chronic
abscess
ThinPeriph
eral Emphesemato
us bulla
Centralpneu
matocele
Wall thickness
site1. Fungal ball.2. Rupture hydatid cyct3. Necrotic tumor4. Blood glot

LINEAR PATTERN
1 )Linear (reticular) abnormality is due to pathology involving:
• airways, • lymphatics, • veins, • interstitium of the lung.
2 )Volume loss is a key finding in fibrosis.

LINEAR PATTERNLINEAR PATTERN
Perihilar and peripheral basal septal lines,changes acutely and resolves with diuretics
LEFT VENTRICULAR FAILURE
Coarsening of lung markings in lower zones, nochange on review of recent films
Normal ageing
Coarse nodular and linear thickening ofmarkings, known malignancy, often associatedwith pleural effusion, rapid clinicaldeterioration of patient
Lymphangitis

LINEAR PATTERN
LINEAR PATTERNShort thin lines, often basal, new on review ofprevious films
Atelectasis
Longer thicker bands, often perihilar or basal,suggest recent infection or infarction
Subsegmentalcollapse
Any length, persist over time unchanged
Volume loss is key, persists over time
Scarring
Fibrosis

Causes of fibrosisMid zone lung Lower zone lung Upper zone lung
tuberculosis Drug indused fibrosis(most common)
sarcoidosis
Chronic extrinsic allergic alveolitis
UIP
Radio-therapy Asbestose-related fibrosis
Ankylosing spondylitis
Progressive massive fibrosis
histoplasmosis

Case-1• A 49-year-old white woman presents with progressive cough and
dyspnea.• She denies any history of arthritis, skin lesions, or eye complaints.• On physical examination, vital signs are:
– pulse 90 bpm; – temperature 98°F;– respirations 32/min;– blood pressure 119/76 mm Hg.
• General exam: patient is in moderate distress, and pertinent physical findings reveal clubbing of the fingers and bilateral “Velcro” rales on lung auscultation.
• ABGs on room air: pH 7.47; PCO2 32 mm Hg; PO2 60 mm Hg with further de-saturation on mild exertion

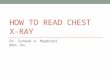
Case-1

POSITION •PA CXR
QUALITY •Good Technical Quality
LESION •Bilateral reticular infitration •At lower zone and left mid zone
MEDIASTINAL\Hilum
•Central trachea and mediasteinal.
ANGELS •Hazy left angle .
OTHER •No

Case-1
:1-Least likely to be associated with this condition isa. Positive antinuclear antigenb. Positive rheumatoid factorc. Increased erythrocyte sedimentation rated. Increased IgE
2 -What is the most likely diagnosis?a. Idiopathic pulmonary fibrosisb. Langerhans granulomatosis/histiocytosis-X disordersc. Rheumatoid lungd. Sarcoidosis
3 -PFTS would be expected to showa. An obstructive patternb. A restrictive patternc. A normal patternd. A reversible obstructive pattern

Case-2
• A 65-year-old woman from Honduras complains of arthralgias and difficulty getting out of a chair and doing her daily chores at home.
• She has muscle aches and generalized weakness, dyspnea, and cough.
• On physical• examination, vital signs are:
– pulse 98 bpm; – temperature normal; – Respirations 23/min– bilateral crackles on lung exam.
• Neuro exam reveals proximal muscular weakness with no sensory deficit.
• CPK and aldolase are increased: • sedimentation rate is 120 mm/min. • PFT: restrictive pattern.

Case-2

POSITION •PA CXR
QUALITY •Poor Technical Quality
LESION •Bilateral reticular infitration •Diffuse bilateral lung especially left lower zone.
MEDIASTINAL\Hilum
•Central trachea and mediasteinal.
ANGELS •Free .
OTHER •Right hemi-diaphragm elevated

Case-2
1 .What is the most likely diagnosis?a. Paraneoplastic syndromeb. Polymyositisc. Sjِgren syndrome
d. Scleroderma
2 .There is an increased association of one of the following with this conditiona. Carcinoma of the pancreasb. Diabetes mellitusc. Diabetes insipidusd. Alzheimer’s disease

Case-3
• A 48-year-old female nurse is seen with complaints of cough.
• She has been treated for “bronchitis” without much improvement.
• On exam, she is afebrile and has crackles in the upper zones of the lung field.
• PPD is negative and sputum for AFB is negative.

Case-3

POSITION •PA CXR
QUALITY •Good Technical Quality
LESION •Bilateral reticular infitration •Diffuse bilateral lung especially middle,upper zone.
MEDIASTINAL\Hilum
•Central trachea and mediasteinal.•Bilateral hilar enlargement\parathraceal
ANGELS •Disappear.
OTHER •No

Case-3
• 1. The most likely diagnosis is:• a. Tuberculosis• b. Blastomycosis• c. Sarcoidosis• d. Silicosis• 2. All of the following findings may be seen in this
patient except• a. Uveitis• b. Skin lesion• c. Bony cysts• d. Hypocalcemia

Case-4• A 56-year-old black male non-smoker is seen with a history of dyspnea• on walking two blocks and chronic chest congestion and cough. • He has been followed for progressive shortness of breath after his
CABG. • Recently, he was ill with a flulike illness, but he denies any fever or
chills presently.• Past history: reveals a GI clinic follow-up for inflammatory bowel disease
for• which he has been on chronic steroid therapy off and on. • On physical examination, vital signs are:
• pulse 110 bpm; • temperature normal; • respirations24/min; • blood pressure 120/78 mm Hg.
• General exam: patient appears frail but in no distress. • Pertinent findings:
• coarse rhonchi and scattered expiratory wheeze with squeaks. • Heart exam reveals normal S1-S2 with no gallop.• There is no hepatomegaly or pedal edema.

Case-4
• Laboratory data: • Hb 11 g; Hct 33%; • WBCs 15.0/μL; differential normal.
• PFTs/spirometry: • FVC 3.43 L (78% of predicted); • FEV1: 2.15 L (63% of predicted); • FEV1/FVC% 72%;• TLC 5.34 L (69% of predicted);• DLCO 14 cc/min/mm Hg (57% of predicted).
• Echocardiogram shows an:• ejection fraction of 55%.• no focal dyskinesia.

Case-4

POSITION •PA CXR
QUALITY •Poor Technical Quality
LESION •Bilateral reticular infitration •Diffuse bilateral lung especially peripherial lower right zone.
MEDIASTINAL\Hilum
•Central trachea and mediasteinal.
ANGELS •Free .
OTHER •No

Case-4
• 1. What is the most likely diagnosis?• a. Congestive heart failure• b. COPD• c. Nonspecific pneumonitis• d. Bronchiolitis obliterans with organizing pneumonia (BOOP)• 2. There may be an increased risk of one of the
following during therapy in this patient:• a. Pulmonary embolism• b. Staphylococcal infection• c. Mycobacterial infection• d. HIV infection

Case-5
• A 50-year-old woman is admitted with progressive shortness of breath.
• She was well until about 2 mo ago, when she noted that she was getting tired and fatigued easily.
• She gives a history of working as a domestic worker and “cleaning lady” for many years.
• Recently, she was working for a company that did maintenance work on boats in a marina area.
• She now has cough, shortness of breath, and low-grade fever with malaise.
• This has continued despite symptomatic treatment.

Case-5
• On exam she is found to be in:• mild to moderate distress • with harsh vesicular breath sounds, • Diffuse rhonchi• bilateral basilar crackles on lung exam, more
on the right.• Routine labs are normal, • PPD is 5 mm.• sputum is negative for fungal.• AFB smear with cultures pending.

Case-5

POSITION •AP CXR
QUALITY •Poor Technical Quality
LESION •Bilateral reticular (linar) infitration •bilateral lower lung zone.
MEDIASTINAL\Hilum
•Central trachea and mediasteinal.
ANGELS •Bilateral hazy angels .
OTHER •No

Case-5
• 1. The most likely diagnosis is• a. Silicosis• b. Asbestosis• c. Extrinsic allergic alveolitis• d. Nontuberculous mycobacterial infection• 2. Associated with this condition is• a. Increased lung volumes• b. Decreased diffusion• c. Peripheral eosinophilia• d. Inorganic dust exposure