Embed Size (px)
Citation preview

03-03-2015 1
GOOD MORNING
Host Microbial Interaction
Part – I
03-03-2015 2
Contents
1. Introduction.
2. Microbial Virulence.
3. Bacterial adherence in periodontal environment.
4. Host tissue invasion.
5. Bacterial evasion of host defense mechanism.
6. Bacterial enzymes capable of tissue destruction.
7. Immunological aspects of host microbial interaction.
8. Host defense processes
9. Host responses to bacterial invasion.
10. Inflammatory responses
11. Molecules, Cells and Processes in Host Response.
12. Connective Tissue Alterations
13. Bone Destruction
14. Healing processes in periodontitis.
03-03-2015 3
1. Introduction
• Periodontal disease is initiated and sustained
by factors (substances) produced by the
subgingival microbiota (the biofilm).
1. Direct injury to host cells and tissues.
2. Activation of inflammatory or cellular and
humoral immune systems that cause damage
to the periodontal tissues.
03-03-2015 4
2. Microbial Virulence
• The properties of a microbe that enable it to
cause disease are referred to as virulence
factors.
• To function as pathogen, bacteria must:
1. Colonize at appropriate host tissue site.
2. Cause destruction of the host tissues.
03-03-2015 5
3. Bacterial Adherence in
Periodontal Environment
• Attachment to Acquired pellicle or saliva
coated tooth surfaces.
• Critical process in tissue invasion
03-03-2015 6
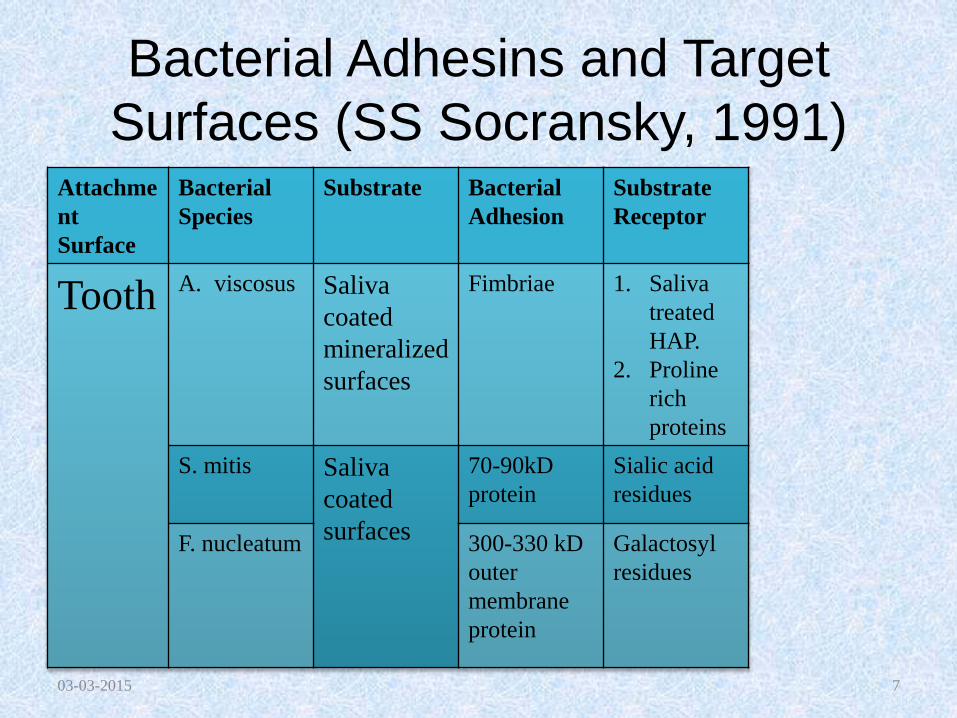
Bacterial Adhesins and Target
Surfaces (SS Socransky, 1991)Attachme
nt
Surface
Bacterial
Species
Substrate Bacterial
Adhesion
Substrate
Receptor
Tooth A. viscosus Saliva
coated
mineralized
surfaces
Fimbriae 1. Saliva
treated
HAP.
2. Proline
rich
proteins
S. mitis Saliva
coated
surfaces
70-90kD
protein
Sialic acid
residues
F. nucleatum 300-330 kD
outer
membrane
protein
Galactosyl
residues
03-03-2015 7
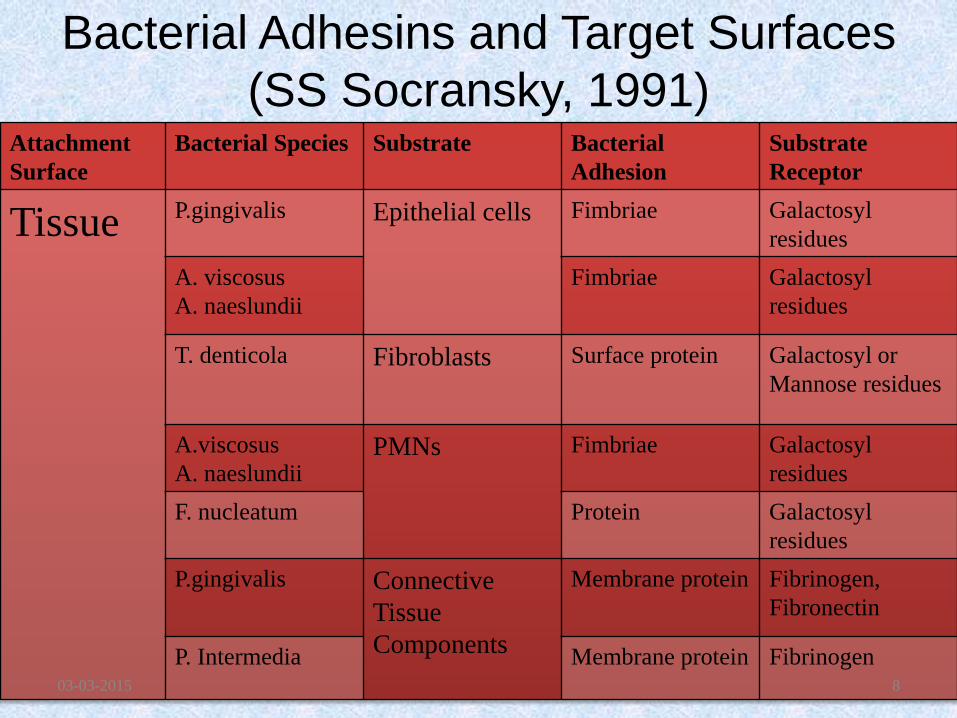
Bacterial Adhesins and Target Surfaces
(SS Socransky, 1991)Attachment
Surface
Bacterial Species Substrate Bacterial
Adhesion
Substrate
Receptor
Tissue P.gingivalis Epithelial cells Fimbriae Galactosyl
residues
A. viscosus
A. naeslundii
Fimbriae Galactosyl
residues
T. denticola Fibroblasts Surface protein Galactosyl or
Mannose residues
A.viscosus
A. naeslundiiPMNs Fimbriae Galactosyl
residues
F. nucleatum Protein Galactosyl
residues
P.gingivalis Connective
Tissue
Components
Membrane protein Fibrinogen,
Fibronectin
P. Intermedia Membrane protein Fibrinogen03-03-2015 8
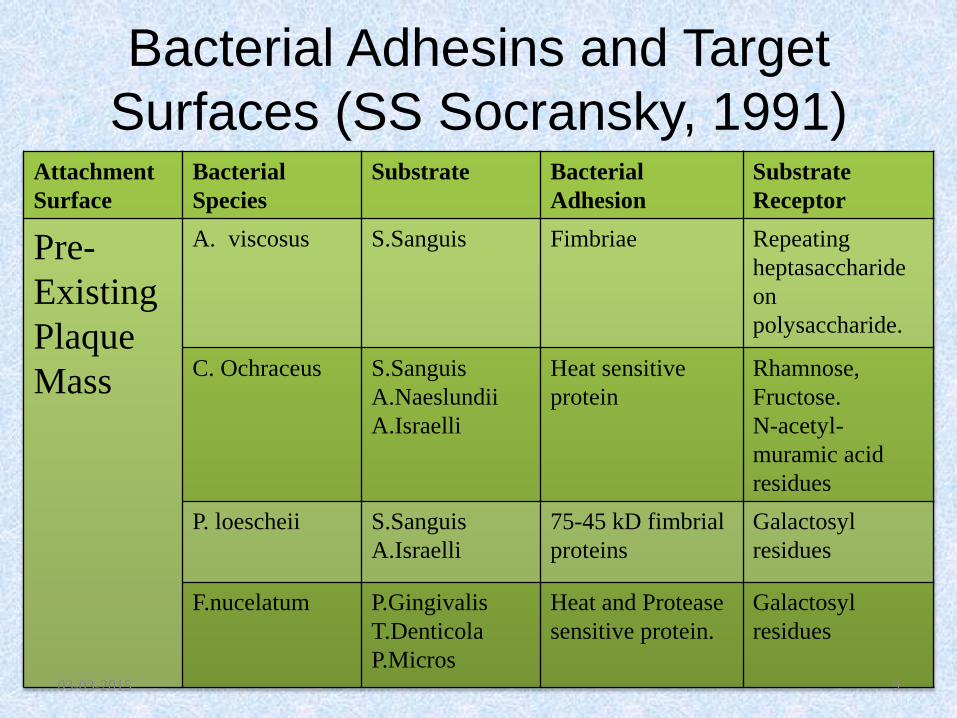
Bacterial Adhesins and Target
Surfaces (SS Socransky, 1991)Attachment
Surface
Bacterial
Species
Substrate Bacterial
Adhesion
Substrate
Receptor
Pre-
Existing
Plaque
Mass
A. viscosus S.Sanguis Fimbriae Repeating
heptasaccharide
on
polysaccharide.
C. Ochraceus S.Sanguis
A.Naeslundii
A.Israelli
Heat sensitive
protein
Rhamnose,
Fructose.
N-acetyl-
muramic acid
residues
P. loescheii S.Sanguis
A.Israelli
75-45 kD fimbrial
proteins
Galactosyl
residues
F.nucelatum P.Gingivalis
T.Denticola
P.Micros
Heat and Protease
sensitive protein.
Galactosyl
residues
03-03-2015 9
4. Host Tissue Invasion
1. Bacteria may enter host tissues through ulcerations in the epithelium of gingival sulcus or pocket that are visible in the intercellular spaces of the gingival tissues.
2. Direct penetration of bacteria into host epithelial or connective tissue cells.
(Aac: Sreenivasan PK, 1993;
P.gingivalis: Sandros J, 1993;
F.nucleatum: Wang B, 1993;
T.denticola: Han YW,2000)
03-03-2015 10
Host Tissue Invasion
3. This ability of the bacteria to invade the host
tissue is one of the key characteristic in
distinguishing pathogenic from non pathogenic
strains.
4. Localization of bacteria in the tissues provides
an ideal position from which the bacteria can
deliver toxic molecules and enzymes to the host
tissue cells and this may be the significance of
invasion as a virulence factor.
03-03-2015 11
• The bursts of disease activity in periodontal
diseases may be related to active phases of
bacterial invasion of the tissues. (Saglie FR,
1988)
• Bacteria in the tissue may enable persistence
of the species in the pocket by providing a
reservoir for colonization.
03-03-2015 12
5. Bacterial Evasion of Host
Defense Mechanisms
• Bacterial adherence avoids displacement by
host secretions.
• Cell invasion disrupts natural barriers formed
by the host tissues.
• Bacterial Properties in Evasion of Host
Defense Mechanism (SS Socransky, 1991):
03-03-2015 13
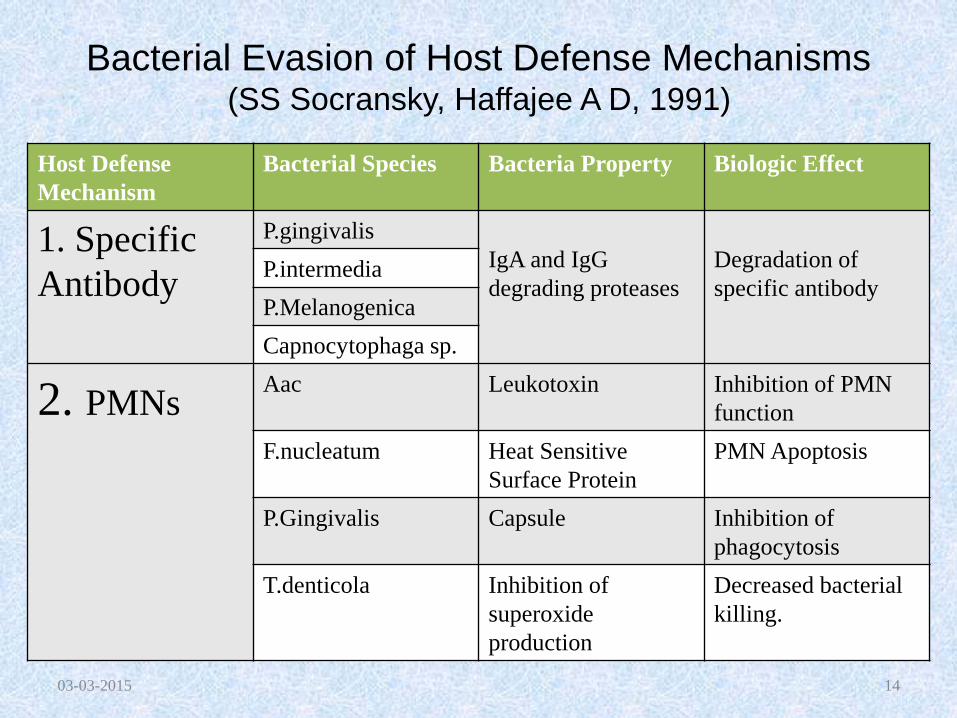
Bacterial Evasion of Host Defense Mechanisms (SS Socransky, Haffajee A D, 1991)
03-03-2015 14
Host Defense
Mechanism
Bacterial Species Bacteria Property Biologic Effect
1. Specific
Antibody
P.gingivalis
IgA and IgG
degrading proteases
Degradation of
specific antibodyP.intermedia
P.Melanogenica
Capnocytophaga sp.
2. PMNsAac Leukotoxin Inhibition of PMN
function
F.nucleatum Heat Sensitive
Surface Protein
PMN Apoptosis
P.Gingivalis Capsule Inhibition of
phagocytosis
T.denticola Inhibition of
superoxide
production
Decreased bacterial
killing.
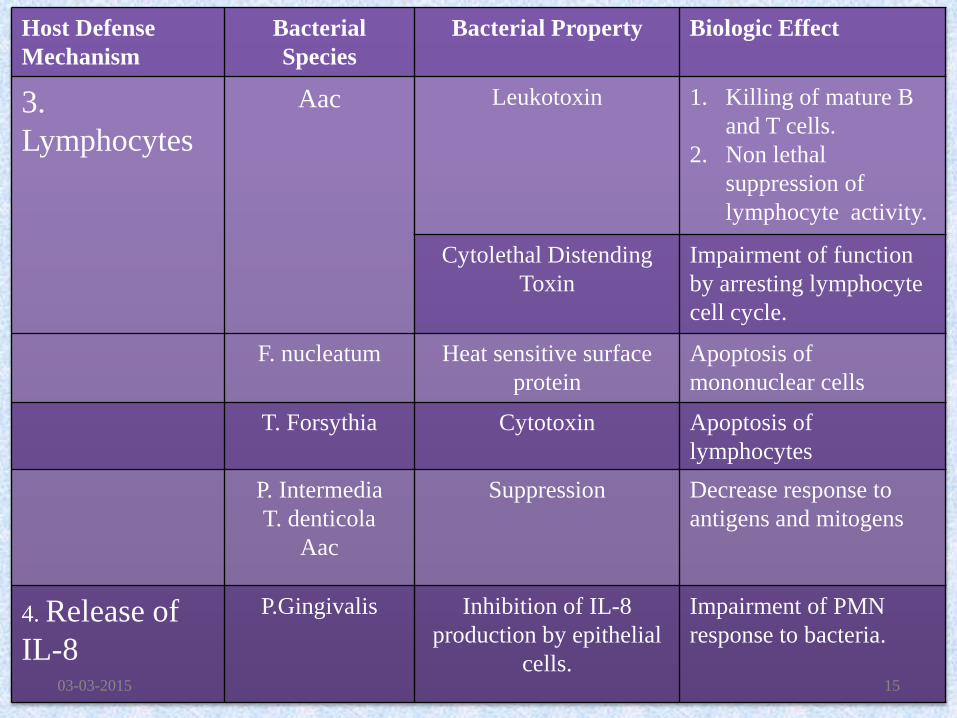
Host Defense
Mechanism
Bacterial
Species
Bacterial Property Biologic Effect
3.
Lymphocytes
Aac Leukotoxin 1. Killing of mature B
and T cells.
2. Non lethal
suppression of
lymphocyte activity.
Cytolethal Distending
Toxin
Impairment of function
by arresting lymphocyte
cell cycle.
F. nucleatum Heat sensitive surface
protein
Apoptosis of
mononuclear cells
T. Forsythia Cytotoxin Apoptosis of
lymphocytes
P. Intermedia
T. denticola
Aac
Suppression Decrease response to
antigens and mitogens
4. Release of
IL-8
P.Gingivalis Inhibition of IL-8
production by epithelial
cells.
Impairment of PMN
response to bacteria.
03-03-2015 15
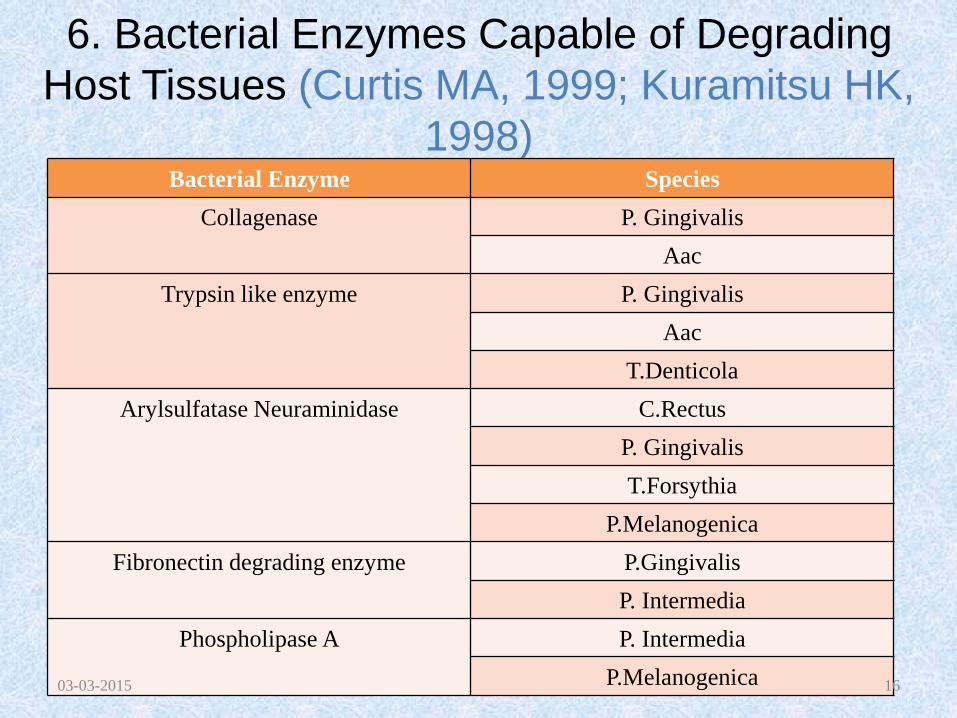
6. Bacterial Enzymes Capable of Degrading
Host Tissues (Curtis MA, 1999; Kuramitsu HK,
1998)Bacterial Enzyme Species
Collagenase P. Gingivalis
Aac
Trypsin like enzyme P. Gingivalis
Aac
T.Denticola
Arylsulfatase Neuraminidase C.Rectus
P. Gingivalis
T.Forsythia
P.Melanogenica
Fibronectin degrading enzyme P.Gingivalis
P. Intermedia
Phospholipase A P. Intermedia
P.Melanogenica03-03-2015 16
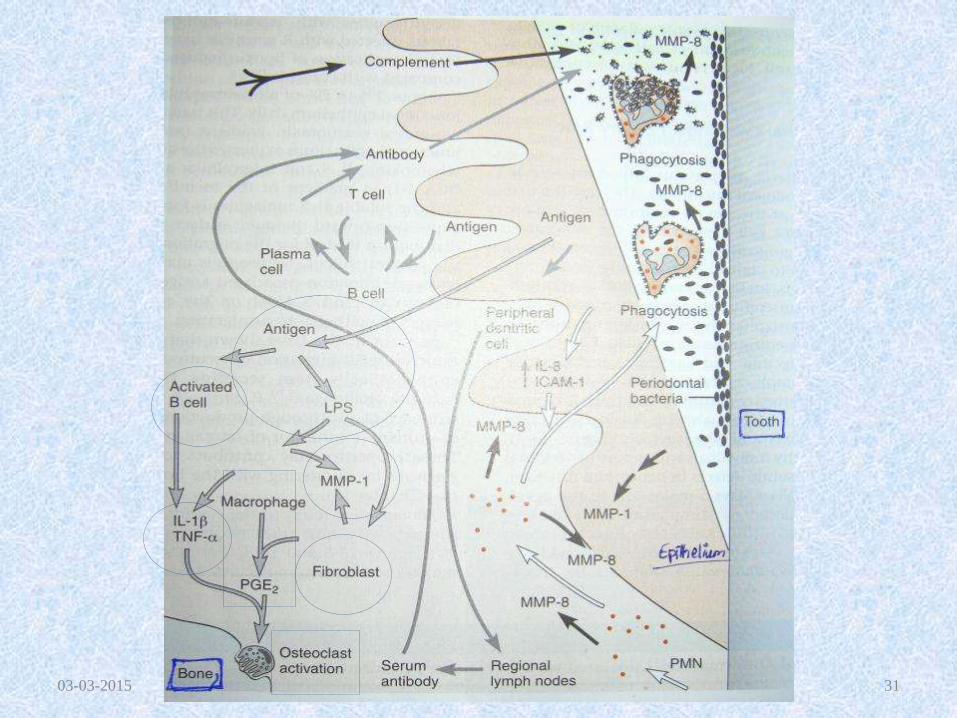
7. Immunological Aspects of
Microbial Host Interaction
• Well characterized interactions involve release of :
1. IL-1
2. TNF
3. Prostaglandins
These host derived mediators have the potential to stimulate bone resorption and activate or inhibit other host immune cells.
03-03-2015 17
From monocytes,
macrophages and PMNs
exposed to bacterial
endotoxin (LPS)
[Roberts FA, 1997.
Yoshimura A, 1997]
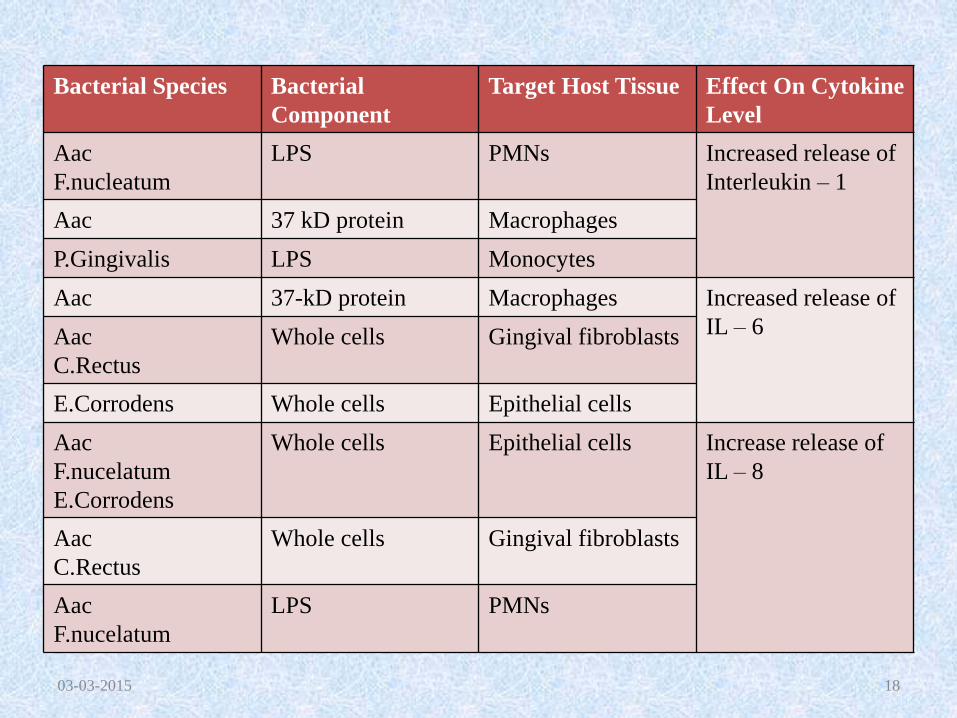
Bacterial Species Bacterial
Component
Target Host Tissue Effect On Cytokine
Level
Aac
F.nucleatum
LPS PMNs Increased release of
Interleukin – 1
Aac 37 kD protein Macrophages
P.Gingivalis LPS Monocytes
Aac 37-kD protein Macrophages Increased release of
IL – 6 Aac
C.Rectus
Whole cells Gingival fibroblasts
E.Corrodens Whole cells Epithelial cells
Aac
F.nucelatum
E.Corrodens
Whole cells Epithelial cells Increase release of
IL – 8
Aac
C.Rectus
Whole cells Gingival fibroblasts
Aac
F.nucelatum
LPS PMNs
03-03-2015 18
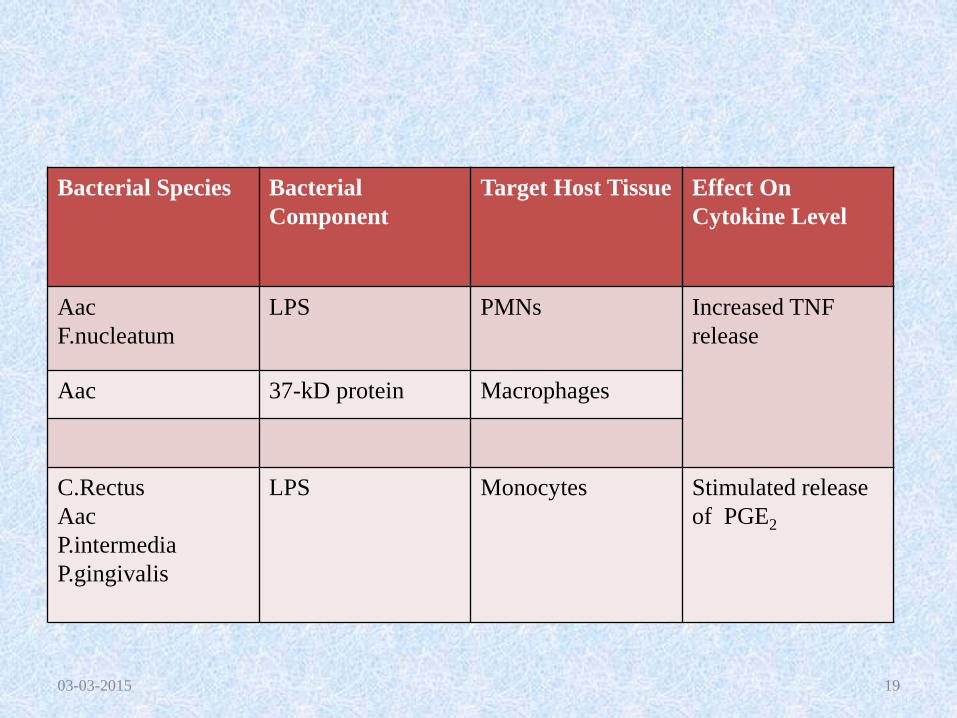
Bacterial Species Bacterial
Component
Target Host Tissue Effect On
Cytokine Level
Aac
F.nucleatum
LPS PMNs Increased TNF
release
Aac 37-kD protein Macrophages
C.Rectus
Aac
P.intermedia
P.gingivalis
LPS Monocytes Stimulated release
of PGE2
03-03-2015 19
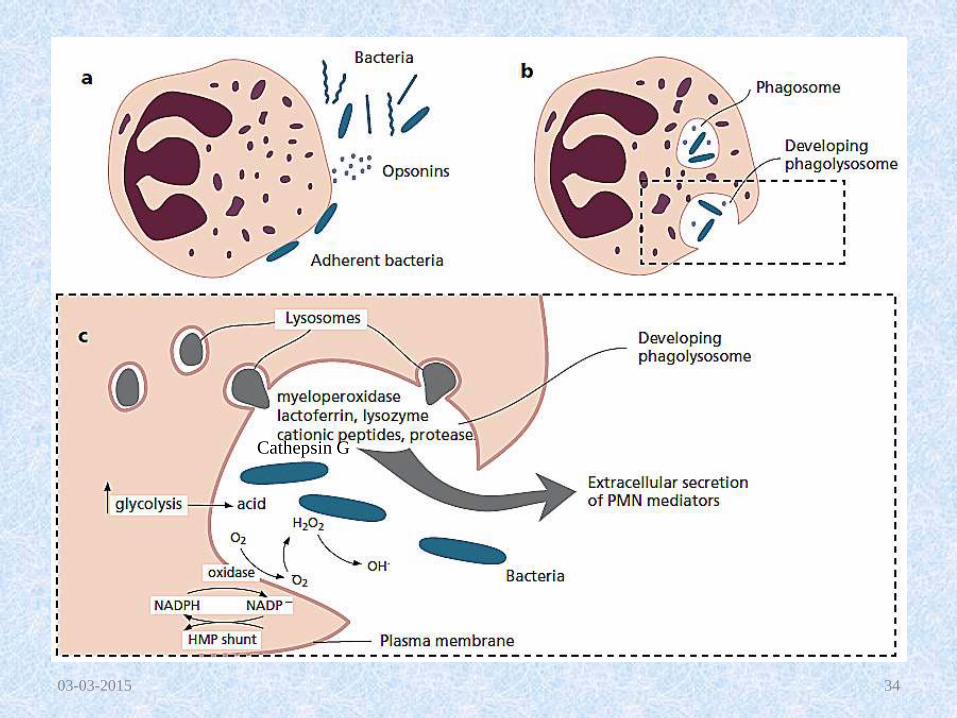
8.Host Defense Processes
• Innate Responses (Non-specific)
• Innate reactions include the inflammatory response and do not involve immunological mechanisms.
• Adaptive Responses (Specific)
• Adaptive reactions that include immunological responses tend to be very effective as the host response is specifically “tailored” to the offending pathogen(s).
03-03-2015 20
9. Host responses to Bacterial
Infection• Innate factors such as complement, resident leukocytes
especially mast cells play an important role in signaling endothelium and thus initiating inflammation.
• Acute inflammatory cells (Neutrophils) protect local tissues by controlling the periodontal microbiota within the gingival crevice and junctional epithelium.
• Chronic inflammatory cells ; macrophages and lymphocytes protect the entire host from within the subjacent connective tissues and do all that is necessary to prevent a local infection from becoming systemic and life threatening, including the sacrifice of local tissues.
03-03-2015 21
• Neutrophils function as antimicrobial cells.
• Chronic inflammatory cells organize adaptive responses.
• Neutrophils function to contain the microbial challenge through phagocytosis and killing and may contribute to local tissue changes by release of tissue degrading enzymes.
• The chronic inflammatory cells, the lymphocytes and monocytes, orchestrate connective tissue changes associated with both periodontal infection and repair and healing.
• They also function to assist the neutrophils in controlling bacterial infection by forming specific opsonic antibodies.
03-03-2015 22
10. Inflammatory Processes
• Redness
• Heat
• Swelling
• Pain
• Loss of function
03-03-2015 23
11. Molecules, Cells, and
Processes in Host Response
• PMNs
• Proteinases
• Proteinase inhibitors
• MMPs
• Cytokines
• Prostaglandins
• Bone Destruction
03-03-2015 25
Neutrophils / Polymorphonuclear
Leukocytes
• Elastase, a serine protease, is contained in the primary granules of the PMN; may cause tissue breakdown and is present with increased activity at sites of gingival inflammation.
• Lactoferrin is contained in the secondary granules of the PMN, and is released during PMN migration and is associated with PMN activation.
• A greater proportion of lactoferrin to elastase was found in advanced periodontitis lesions than in gingivitis sites.
03-03-2015 26
• TNF – A plays a major role in development of
inflammation by stimulating the release of
cytokines, including IL-1B from neutrophils.
(Price TH, 1994).
• Lipoxin A4 is a cytokine regulating lipid
mediator that can reduce the inflammation
induced by TNF – A.
• 1% - 2% Neutrophils migrate across the
junctional epithelium daily; which requires a
chemotaxin gradient.
03-03-2015 27
03-03-2015 28
03-03-2015 29
03-03-2015 30
03-03-2015 31
• P.gingivalis impedes transendothelial
migration of neutrophils (Madianos PN, 1997)
and prevents epithelial cells from secreting IL-
8 in response to bacterial challenge. (Huang
GT-J, 1998; Darveau RP, 1998)
03-03-2015 32
03-03-2015 34
Cathepsin G
12. Connective Tissue Alterations:
Tissue Destruction in Periodontitis
• Remodeling of connective tissues that leads to
a net loss of local soft tissues, bone and
periodontal attachment apparatus.
• The fundamental event in the transition from
gingivitis to periodontitis is the loss of soft
tissue attachment to the tooth and subsequent
loss of alveolar bone.
03-03-2015 35
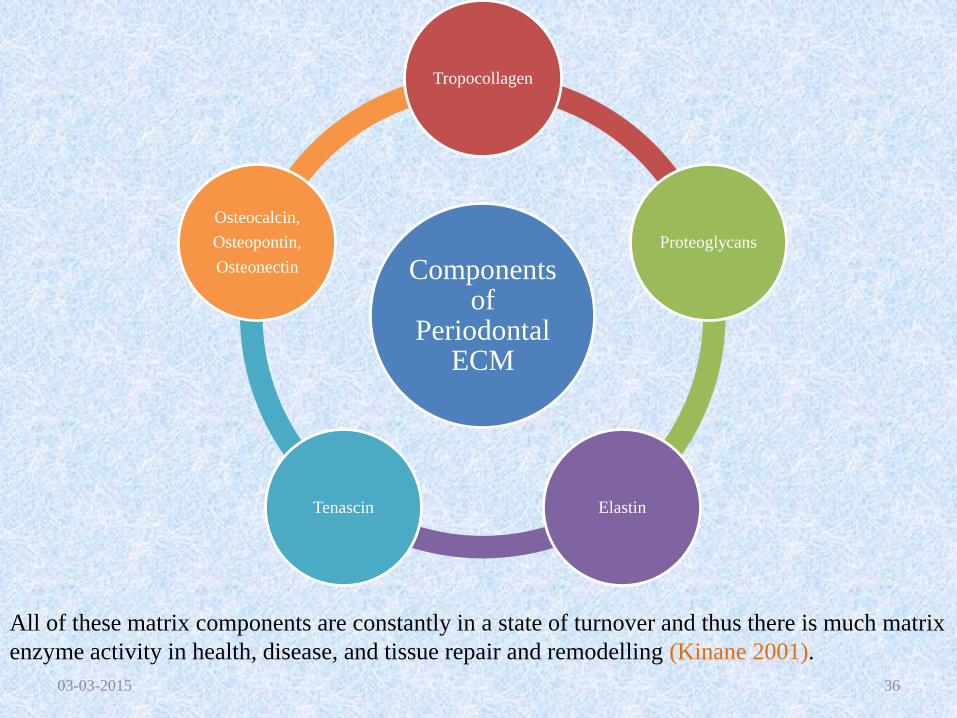
Components of
Periodontal ECM
Tropocollagen
Proteoglycans
ElastinTenascin
Osteocalcin,
Osteopontin,
Osteonectin
03-03-2015 36
All of these matrix components are constantly in a state of turnover and thus there is much matrix
enzyme activity in health, disease, and tissue repair and remodelling (Kinane 2001).
Proteinases/Proteases
• Proteinases (collagenase, elastase - like and trypsin-like, as well as serine and cysteine proteinases) cleave proteins by hydrolyzing peptide bonds.
• Depending on the location of activity of the enzyme on its substrate:
1. Endopeptidases
2. Exopeptidases,
• A reduction of protease levels following treatment was obtained in several studies.
03-03-2015 37
Proteinase Inhibitors
Alpha-2 macroglobulin (A2-M)
• Inhibits gingival collagenase
Alpha1 antitrypsin (A1-AT)
• Inhibits PMN collagenase
03-03-2015 38
• MMPs are a family of proteolytic enzymes found in neutrophils, macrophages, fibroblasts, epithelial cells, osteoblasts and osteoclasts. (Ryan ME, 2000) that degrade matrix molecules such collagen, elastin and gelatin.
• MMP1 and MMP8, both are collagenases.
• MMP 8 is released by infiltrating neutrophils whereas MMP1 is expressed by resident cells including fibroblasts, monocytes/macrophages and epithelial cells.
03-03-2015 39
Matrix Metalloproteinases
• MMPs are also produced by Aac and Pg which
is not considered a major factor in disease
progression. (AAP, 2002)
• MMPs are secreted in the inactive/latent form.
• Activation by proteolytic cleavage of a portion
of the latent enzyme.
• Proteases capable of MMP activation:
1. Chymotrypsin like protease by T .denticola
2. Host cell enzyme – Neutrophil Cathepsin G.
03-03-2015 40
• MMPs are inactivated by:
1. Alpha-macroglobulins found in serum and
GCF.
2. Tissue Inhibitors of MMPs (TIMP) produced
by cells of host tissue and fluid.
3. Tetracycline appears to inactivate neutrophil
MMP (Graves DT, 1999)
03-03-2015 41
Other Proteinases
1. Elastase : elastin, collagen, fibronectin.
2. Cathepsin – G: Bacterial proteinase and
MMP – 8 activation.
03-03-2015 42
• Neutrophil (PMN) Collagenase is found in higher
concentrations in inflamed gingival specimens
than in clinically healthy gingiva.
• The increased presence of these MMP enzymes in
diseased over healthy sites (Ohlsson et al. 1973),
their increase during experimental gingivitis
(Kowashi et al. 1979), and decrease after
periodontal treatment (Haerian et al. 1995, 1996)
suggest that MMPs from PMNs are involved in
periodontal tissue breakdown.
03-03-2015 43
Cytokines• Cytokines are soluble proteins, secreted by cells involved in both the
innate and adaptive host response, and act as messenger molecules that transmit signals to other cells.
• Actions:
1. Initiation and maintenance of immune and inflammatory responses.
2. Regulation of growth and differentiation of cells.
• Interleukins are important members of the cytokine group and are primarily involved in communication between leukocytes and other cells, such as epithelial cells, endothelial cells, and fibroblasts engaged in the inflammatory process.
• Interleukin (IL)-1a, IL-1b, and tumor necrosis factor (TNF)-alpha stimulate bone resorption and inhibit bone formation.
03-03-2015 44
• IL-1, IL-6and TNF have the central role in periodontal destruction. (Graves DT, 1999; Page RC, 1976)
• IL1a and IL1b are the 2 active forms.
• Main constituent of IL-1 : Osteoclast Activating Factor.
• IL-1 is produced by activated macrophages or lymphocytes but may also be produced by mast cells, fibroblasts, keratinocytes and endothelial cells.
• Bacterial LPS is a potent activator of macrophage IL-1 and TNFa secretion.
• TNFa and IL-1 can upregulate their own production.
• IL-6 also results in Bone remodeling. (Manolagas SC, 1999)
• TNF-a and TNF-b are active forms.
• TNFa shares similar biologic activity of IL-1a including stimulation of bone resorption. 03-03-2015 45
• Proinflammatory effects of IL-1 and TNF-a
(Page RC,1991):
1. Stimulation of endothelial cells to express
selectins that facilitate recruitment of
leukocytes.
2. Activation of macrophage IL-1production.
3. Induction of PGE2 by macrophages and
gingival fibroblasts.
03-03-2015 46
Prostaglandins
• Arachidonic acid derivative.
• Mediators of inflammation.
• IL-1b, TNFa and bacterial LPS upregulate COX-2.
• PGE2:
1. Potent vasodilator
2. Inducer of cytokine production by various cells.
3. PGE2 acts on fibroblasts and osteoclasts to induce production of MMPs.
03-03-2015 47
13. Bone Destruction
• Bone resorption is mediated by osteoclasts.
• Concomitant with the breakdown of the connective tissue attachment during disease progression.
• The mechanisms involved in bone resorption respond to signals from inflammatory cells in the lesion and initiate degradation of bone in order to maintain a “safety” distance to the periphery of the inflammatory cell infiltrate.
03-03-2015 48
Osteoclasts
• Osteoclasts are multinucleated cells that
develop from osteoclast progenitor
cells/macrophages.
• Mediators such as IL-1 beta, PGE2 and TNF
alpha, IL-6, IL-11 and IL-17 may act as
activators on osteoclasts.
03-03-2015 49
The Receptor Activator Of Nuclear
Factor-kappa Beta (RANK), the
RANK ligand (RANKL) and Osteoprotegrin (OPG)
• RANK is a receptor expressed by osteoclast progenitor cells.
• RANKL and OPG are cytokines that belong to the TNF family and are produced by osteoblasts and bone marrow stromal cells.
• While RANKL promotes activation of osteoclasts, OPG has the opposite effect.
• Thus, the binding of RANKL to the RANK will result in the differentiation of osteoclast progenitor cells into active osteoclasts, while OPG that binds to RANKL will inhibit the differentiation process.
03-03-2015 50
• Analyses of human biopsy specimens revealed that levels of RANKL were higher and levels of OPG were lower in sites with periodontitis than in sites representing healthy gingiva (Crotti et al. 2003; Liu et al. 2003).
• The RANK/RANKL/OPG system is also involved in bone degradation processes that are induced by pro-inflammatory cytokines such as PGE2, TNF alpha, IL-1 beta, IL-6, IL-11, and IL-17.
• The role of T cells, however, is unclear given that this cell not only produces RANKL but also inhibitors of RANKL, such as interferon (IFN)-gamma and IL-4 (Takayanagi 2005).
03-03-2015 51
14. Healing Process in Periodontitis
• Chronic immune system:
1. Regeneration: the replacement of tissues with new, identical tissues that function the same as the original tissues.
2. Repair: replacement of one tissue with another tissue.
• Under normal conditions, a platelet rich clot forms at the site of injury which facilitates in healing.
03-03-2015 52
• In periodontal infections, the platelet rich clot does not form.
• The periodontal healing cycle during the pathogenesis of periodontal diseases is primarily post inflammatory and cellular elements other than platelets provide important signals in this process.
• Periodontal repair occurs in overlapping phases of
1. Inflammation shutdown,
2. Angiogenesis
3. Fibrogenesis.
03-03-2015 53
Inflammation Shutdown• Orchestrated by leukocytes.
• Anti-inflammatory signals generated (Genco RJ,1991):
1. IL-1 receptor antagonist (IL-1ra)
2. Transforming Growth Factor Beta (TGF-b)
3. IL-4
4. IL-10 Manolagas SC, 2000.
5. IL-11
• In the inflamed periodontal tissues:
1. Macrophages produce IL-1ra. (Kabashima, 1996)
2. Mast cells and lymphocytes produce TGF-b. (Steinsvoll 1999)
03-03-2015 54
Angiogenesis and Fibrogenesis
• IL1b and TNF-b participate in both
inflammation and healing.
• IL1a and IL1b are involved indirectly in in
inducing fibroblast proliferation and collagen
synthesis by stimulating the production of
PGE2 or the release of PDGF and TGF-b.
03-03-2015 55
Angiogenesis and Fibrogenesis
• PDGF – AA, PDGF-AB, PDGF – BB, PDGF-CC, PDGF-DD.
• PDGF activates fibroblasts and osteoblasts and results in induction of protein synthesis. (GiannobileWV, 1996).
• TGF-b is a multifunctional peptide that stimulates osteoblasts and fibroblasts and inhibits osteoclasts, epithelial and immune cells.
• TGF-b activates in low pH/acidic conditions.
• It promotes the elaboration of fibroblast extracellular matrix adhesion.
03-03-2015 56
Angiogenesis and Fibrogenesis
• Basic fibroblast growth factor (bFGF)
produced primarily by PDL cells and
endothelium. (Gao J,1996)
• TGF – a (monocyte)
• TNF – a (monocyte)
03-03-2015 57
Healing of Alveolar Bone
• Activation of osteoblasts
• Inactivation of osteoclasts
• TGF-b is a potent inhibitor of osteoclast formation.
• Osteoclast differentiation and activation are inhibited by:
1. Interferon – g secreted by NK cell, Th1Tcells and macrophages. It inhibits IL-1 and TNF-a induced osteoclast activation.
2. IL-1ra is also effective in blocking IL-1 and TNF-a induced osteoclast activation.
03-03-2015 58
Conclusion
03-03-2015 59

Thank You!!!03-03-2015 60





























