Embed Size (px)
DESCRIPTION
Citation preview

Hepatitis C Primer for HIV Care Providers
Adeel A. Butt, MDAssistant Professor of MedicineDivision of Infectious DiseasesUniversity of PittsburghDirector, Pittsburgh VAMC ID-HIV ClinicsCenter for Health Equity Research and Promotion

Adeel A. Butt, MD
Overview
Prevalence of HCV A word of virology Risk Factors Natural History of HCV Treatment of HCV
Treatment Indications and Goals HCV-HIV Co-infection
Treatment of HCV-HIV co-infection

Adeel A. Butt, MD
HCV - Epidemiology
Epidemiology: 1.8% of the U.S. population ~ 4 million infected persons in the
U.S. 8,000 – 10,000 deaths per year
Global prevalence – 170 million 5 X more prevalent than HIV
Lauer, NEJM 2001;345:41-52

Adeel A. Butt, MD
HCV – Global Prevalence
57169.73.15 811Total
1162.23.91 600Western Pacific
332.32.151 500South-East Asia
198.91.03858Europe
721.34.6 466Eastern Mediterranean
713.11.7785Americas
1231.95.3602Africa
Number-of countries by
WHO Region where data are not available
Infected Population(Millions)
Hepatitis C prevalence
Rate %
Total Population(Millions)
WHO Region

Adeel A. Butt, MD
HCV - Virology
The Virus Single stranded, positive sense,
RNA Falviviridae family Spherical, enveloped ~ 50 nm Discovered in 1989
Choo, Science 1989;244:359-62

Adeel A. Butt, MD
HCV - Genetics
Six genotypes, 1 through 6 Multiple subtypes, a, b, c, etc.
Further divided into quasispecies, varying in RNA sequence by 1-9%
RNA sequence may vary by 35% between genotype
Great genetic diversity
Farci, Semin Liver Dis 2000;20:103-26

Adeel A. Butt, MD
HCV Genotype Distribution
Asia6
South Africa5
Africa Egypt
4 4a
Younger population in Western countries, especially IDUs
Predominant genotype in Pakistan Japan, Nepal, Thailand, Indonesia Nepal
3 3a 3b 3c
Worldwide distribution Northern Italy
2 2c
America, Europe, Japan North America, Western Europe Japan Indonesia (20% of total)
1 1a 1b 1c
Geographic DistributionGenotype/Subtype

Adeel A. Butt, MD
HCV – Risk factors
Transfusion Dependent on prevalence in general population Screening methods and diligence in screening
In the US, it dropped from 25% to 0.1% after initiation of screening
1996 risk in the US was 1 in 103,000 units (for HIV this risk was 1 in 493,000 units)
Current risks: HCV – 1 in 1,600,000 units HIV – 1 in 1,800,000 units HBV – 1 in 220,000 units

Adeel A. Butt, MD
Decline in transfusion transmitted viral infections

Adeel A. Butt, MD
Blood Supply Screening Antibody based Antigen based Nucleic acid technology (NAT)
Introduced in 1998 Reduces window period
For HCV: from 70 days to 10 days For HIV: from 22 days (antibody) to 11 days
Potential reasons for transmission Window period Immunovariant strains Persistently antibody negative carriers Testing errors

Adeel A. Butt, MD
HCV – Risk Factors (contd.)
Sexual Transmission Inefficient route of transmission ?risk 1-3%
1 of 85 long term sexual partners1 2 of 42 index cases (one had
independent risk factors)2 Probably enhanced by HIV co-
infection3
1 Conry-Cantilena NEJM 1996;334:1691-6
2 Feldman, STD 2001;27:338-42
3 Bonacini, Arch Int Med 2000,160:3365-73

Adeel A. Butt, MD
HCV – Risk factors (contd.)
Other risk factors and routes of transmission: Tattoos Person-to-person in hemodialysis
units Person-to-person by HCW Nosocomial outbreaks reported Organ and tissue transplant

Adeel A. Butt, MD
HCV – Transmission
Pregnancy and Vertical Transmission Prevalence in pregnant women 0.3-4.4% Over 40% in IDU from NY
Overall vertical transmission rate ~ 6% HIV co-infection increases transmission rates Role of HCV VL and mode of delivery unclear
No known transmission from breast milk

Adeel A. Butt, MD
HCV and Health Care Workers
600,000-800,000 needlestick injuries occur each year
Prevalence in Public Safety workers 1.3-3.2% Prevalence in Scottish HCW 0.28%
Risk of HCV from a needlestick estimated to be 2.7-6%
Multiple reported cases of transmission from HCW to patients
Risk of HCV+ surgeon transmitting it a patient estimated at 1 in 1,750-16,000 procedures

Adeel A. Butt, MD
HCV – Natural History
Acute HCV-100 patients
Resolved - 25 Chronic - 75
Stable – 45-55 Cirrhosis – 20-30
Stable – 15-25Decompensation – 5-8HCC – 1-3 per year
20 – 30 yearsAccelerated by:
alcohol
HIV

Adeel A. Butt, MD
Goals of Treatment
Eradicate HCV replicationDelay fibrosisPrevent liver failurePrevent hepatocellular carcinomaPrevent deathEnhance quality of life
Butt, Singh. Hepatitis C: Prevention, Therapy and Role of Transplantation. In Wenzel (ed) Prevention
and Control of Nosocomial Infections. Fourth Edition. Lippincott, Williams and Wilkins.

Adeel A. Butt, MD
HCV - Treatment
Indications for treatment
Recommended Not recommended Unclear
Detectable HCV RNAPersistently elevated ALTAbnormal liver biopsy showing portal or bridging fibrosis, or at least moderate inflammation
Persistently normal ALTAdvanced or decompensated cirrhosisExcessive alcohol useActive drug useContraindications to treatment
Compensated cirrhosisElevated ALT but normal liver histology

Adeel A. Butt, MD
HCV – Pretreatment Workup
History and Physical Exam Psychiatric history/evaluation Blood counts Chemistry panel Liver panel, including PT TFTs HCV genotype HCV RNA AFP; ?liver imaging Liver biopsy

Adeel A. Butt, MD
HCV - Treatment
Therapy Trade name (manufacturer)
Interferon alfa-2b Intron A (Schering-Plough)
Interferon alfa-2a Roferon (Roche)
Interferon alfacon-1 Infergen (?Amgen)
Interferon alfa-2b plus Ribavirin Rebetron (Schering-Plough)
Pegylated Interferon alfa-2a Pegasys (Roche)
Pegylated Interferon alfa-2b PEG-Intron (Schering-Plough)
Drugs approved for the treatment of HCV infection

Adeel A. Butt, MD
HCV – Treatment (non-HIV Patients)
Sustained Virologic Response Rates
Source: Multiple randomized controlled trails
6
1624
41 39
54
0
10
20
30
40
50
60
IFN 24wks
IFN 48wks
IFN/RBV24 wks
IFN/RBV48 wks
PEG-IFN PEG/RBV

Adeel A. Butt, MD
Treatment Patterns in HCV Infected Patients
155 (65)Number of patients who did not receive treatment for HCV (%)
231 to 36
Estimated duration of HCV infection (years) Mean Range
72.526.6< 1
Race (%) Caucasian African-American Other
982
Gender (%) Male Female
48 yearsAge (mean)
Demographics of patients with HCV (N=237)

Adeel A. Butt, MD
Reasons for non-treatment in HCV only infected patients
Ten most common reasons for non-treatment of HCV in 155 patients. (excludes the unknown category)
3 (2)Deferred while waiting for approval for pegylated interferon
5 (3)End stage liver disease
7 (4)Referred for transplant evaluation
9 (6)Patient refused treatment
11 (7)Concurrent medical problems
12 (8)Psychiatric problems
12 (8)Undetectable HCV RNA
15 (10)Normal liver enzymes
15 (10)Current drug or alcohol use
37 (24)Non compliance with follow up visits
n (%)

Adeel A. Butt, MD
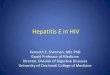
Treatment Patterns in HCV-HIV Co-infected Patients (VACS-3 Cohort)
881 Patients
181 (20.5%, 20.5%) Not Tested
700 (79.5%, 79.5%) Tested
400 (57.1%, 45.4%) Hepatitis C Negative
300 (42.9%, 34.1%) Hepatitis C Postive
210 (70.0%, 23.8%) without GI Referral
67 (31.9%, 7.6%) with No Indication
143 (68.1%, 16.2%) with Indications
38 (26.6%, 4.3%) Eligible for Treatment
90 (30.0%, 10.2%) with GI Referral
26 (28.9%, 3.0%) with No Indication
64 (71.1%, 7.3%) with Indications
27 (42.2%, 3.1%) Eligible for Treatment
12 (44.4%, 1.4%) Underwent Liver Biopsy
2 (16.7%, 0.2%) Received Interferon

Adeel A. Butt, MD
HCV - Treatment
Predictors of a Favorable Response
Genotype 2 or 3 Low HCV Viral Load (<2 million) No or only portal fibrosis Female gender Age < 40 years
Role of gender not an independent factor if controlled for body weightPoynard, Hepatlogy 2000;31:211-8
Manns, Lancet 2001;358:958-65

Adeel A. Butt, MD
Functional Characteristics of PEGylated Proteins
Protected from proteolytic degradation Restricted distribution Reduced renal clearance Enhanced solubility PEG-moiety is biocompatible and
nontoxic
Harris JM, Poly (Ethylene Glycol) Chemistry. 1992.
Katre NV. Adv Drug Delivery Rev. 1993.

Adeel A. Butt, MDRoche, data on file, Phase
II trial.
0
5
10
15
20
25
30
0 24 48 72 96 120 144 168 192
Time (hours)
Con
cen
trati
on
(n
g/m
L) Tue Wed Thu Fri Sat SunMon
PEGASYS (PEG-IFN) 180 mcg SC qw in patients with CHC* (Week 48)
The Inherent Qualities of PEG-alfa 2a
*CHC=chronic hepatitis C