Embed Size (px)
Citation preview
Hepatitis and its prophylaxis
1
CONTENTS
Introduction
Functions of liver
Hepatitis A,B,C,D,E
Chronic hepatitis
Drug induced liver disease
Cirrhosis
Alcoholic liver disease
19-01-20152
INTRODUCTION
Hepatitis is inflammation of the liver that may result from infectious or other causes.
Hepatitis is a worldwide heath problem with more than 5 million new cases occuring annually and more than 300 million persons across the globe carrying the viruses.
19-01-20153
19-01-20154
19-01-20155
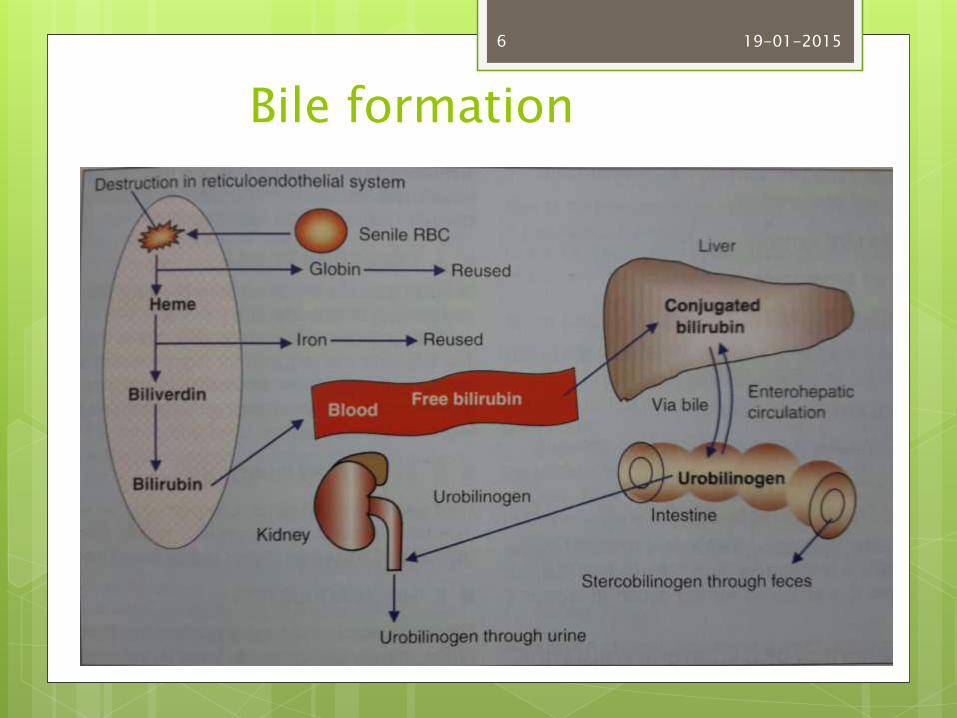
Bile formation
19-01-20156
Functions of liver
Metabolic
Storage- glycogen, amino acids, iron, folic acid, vit A, B12, D
Synthetic- produces glucose, synthesis of plasma proteins, clotting factors, hormone binding proteins
Secretion of bile
19-01-20157
Excretory – excretion of cholesterol, bile pigments, heavy metals, toxins, bacteria, virus
Hemopoietic- stores vit B12 necessary for erythropoiesis and iron , thrombopoietin
Hemolytic –destruction of senile RBCs
Inactivation of hormones and drugs-catabolizes hormones
Defense and detoxification
19-01-20158
19-01-20159
19-01-201510
Causes of liver disease Congenital hyperbilirubinaemia-
Rhesus incompatibilityprematuritybiliary atresiaGilbert’s syndromeCrigler-Najjar syndrome
Dental aspects- disorders associated with an early rise in serum levels of conjugated bilirubincan cause dental hypoplasia and a greenish discoloration of the teeth
19-01-201511
Parenchymal liver disease (hepatocellular)
Viral hepatitis
Chronic hepatitis
Cirrhosis
Primary biliary cirrhosis
Drug induced hepatitis
19-01-201512
Extrahepatic biliary obstruction-
Gallstones
Ca of pancreas
19-01-201513
Parenchymal liver disease
Acute viral hepatitis-
5 distinct types-A,B,C,D,E
Other viruses- EBV,CMV, herpes simplex
19-01-201514
Hepatitis A
Infectious hepatitis
Endemic throughout the world but seen particularly where socioeconomic level is poor
Transmission- feco-oral
Can also be transmitted sexually and in body fluids including saliva
19-01-201515
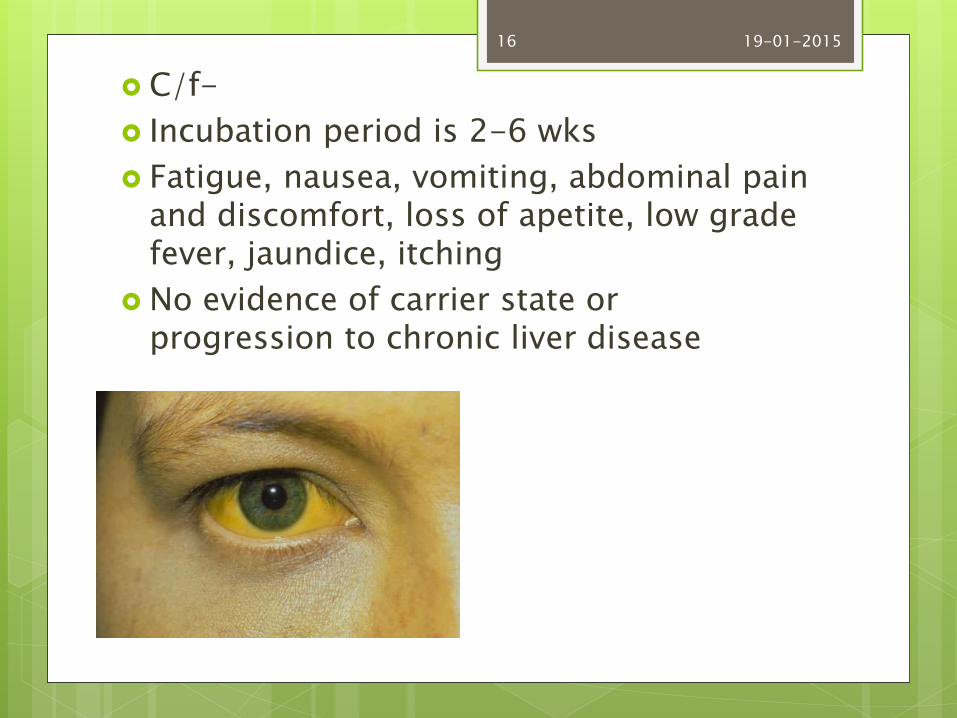
C/f-
Incubation period is 2-6 wks
Fatigue, nausea, vomiting, abdominal pain and discomfort, loss of apetite, low grade fever, jaundice, itching
No evidence of carrier state or progression to chronic liver disease
19-01-201516
General management
Diagnosis is confirmed by serum antibodies to the virus- antiHAV
Can be prevented by administration of HAV immune globulin 0.02 mg/kg prophylactically or within 2 wks of exposure
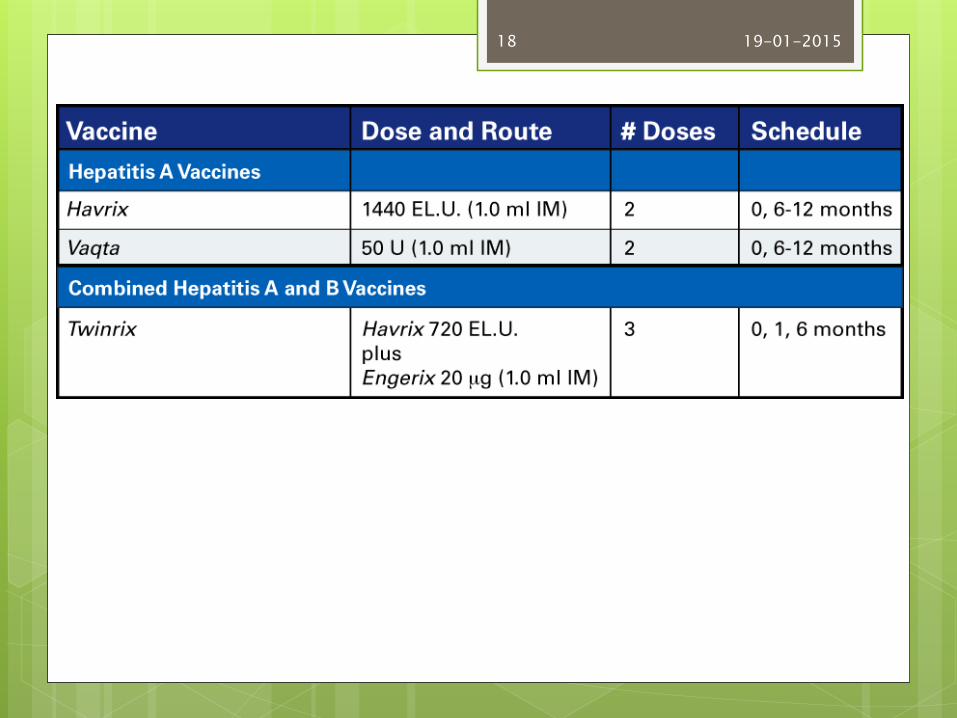
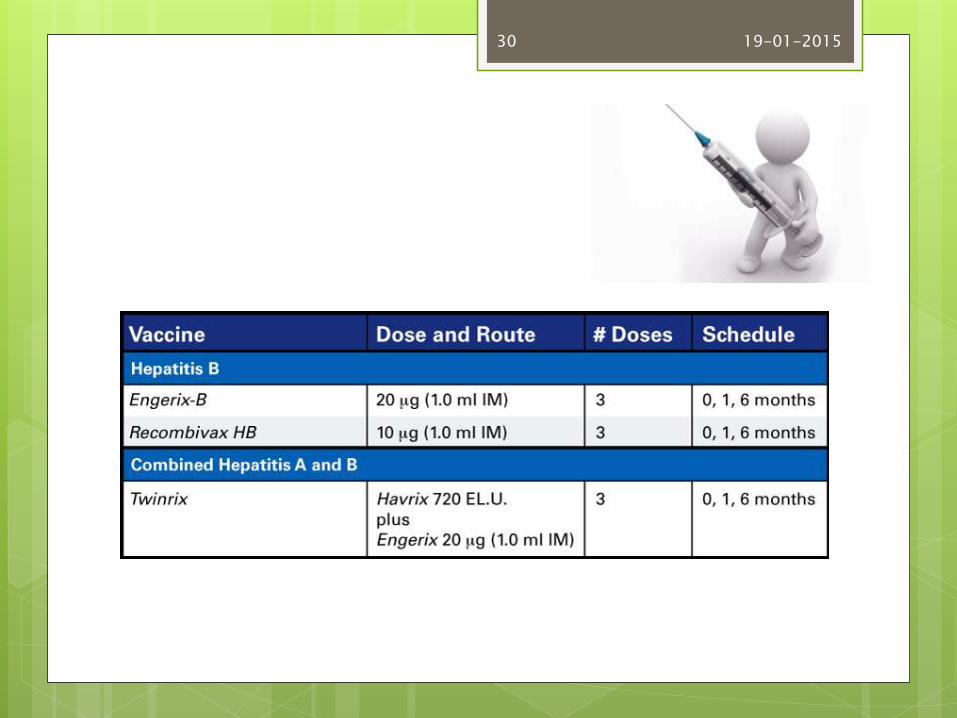
Vaccine is available for prophylaxis in travellers to high risk endemic areas-Havrix, vaqta and twinrix
19-01-201517
19-01-201518
Hepatitis B
HBV
Can cause lifelong infection, cirrhosis of liver, liver cancer, liver failure and death
Transmission- parenteral- via unscreened blood or blood products, IV drug abuse, sharing of needles, sexually, tattoing/body piercing, vertical transmission
19-01-201519
19-01-201520
High risk groups Pts who have received unscreened blood products
or multiple plasma or blood transfusion Haemodialysis for end stage renal disease Immunosuppressed (eg. HIV) Residents and staff of long stay institutions,
particularly prisons Occupations that expose to human blood
especially surgeons IV drug abusers Travellers to endemic areas Chronic liver disease Newborns whose mothers are infected with HBV
19-01-201521
Clinical features
Incubation period is 2-6 months
Effects range from subclinical infections without jaundice, to fulminating hepatitis, acute hepatic failure and death
Prodromal symptoms(1-2 wks)- anorexia, malaise and nausea
Jaundice- pale stools and dark urine
Enlarged and tender liver
Muscle pain, arthralgia and rashes
19-01-201522
Complications
Carrier state- HBV persists within the body for more than 6 months(develops in 5-10%)
More frequent in anicteric infections
Carriage may persist for up to 20 yrs and may be asymptomatic.
Pts who have received blood products, those infected with HDV and those with immune defects are predisposed to carrier state.
19-01-201523
Serum enzyme estimations – AST, ALT are raised in proportion to the severity of illness
Alkaline phosphatase and serum bilirubin are also raised
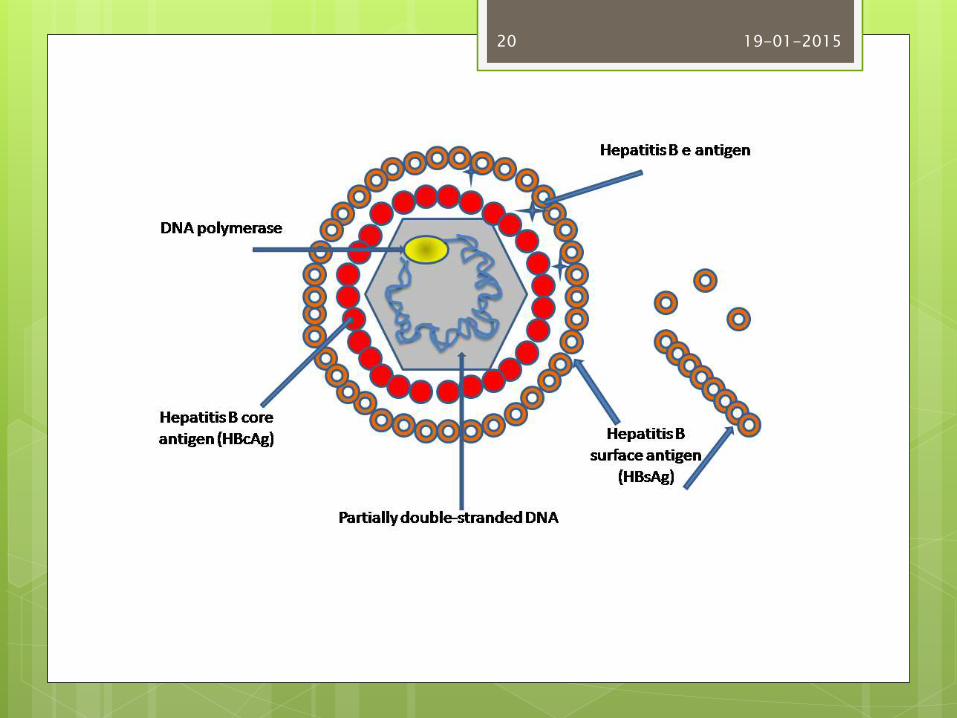
Serologic markers- EM shows 3 types of particles in serum Dane particle-intact hepatitis virus (inner core of
DNA and core antigen HBcAg and outer envelope of HBsAg.
Persitance of HBsAg beyond 13 wks of clinical illness indicates carrier state is developing
HBeAg
19-01-201524
Anti-HBs develops after infection or vaccination and in the absence of HBsAgimplies immunity
HBeAg- active disease and high infectivityfound only in serum that is HBsAg positive.persistance beyond 4 wks of the onset of
symptoms indicates tht the patient will probably remain infectious and develop chronic liver diseaseAnti Hbe indicates complete recovery and loss of infectivity provided HBeAg is lost
19-01-201525
HBcAg- found in liver biopsy in acute hepatitis
Sensitive marker of viral replication and indicates current or recent infection
antiHBc associated with antiHBs indicates recovery and immunity
If antiHBs is absent it indicates carrier state or chronic hepatitis
DNA polymerase appears transiently in the serum early in the course infection. If it is demonstrable in HBsAg carriers , it indicates high infectivity
19-01-201526
General management Bed rest Avoid hepatotoxins like alcohol Chronic HBV infection can be treated with
lamivudine or interferon or adefovir dipivoxil Prevention- avoiding contact with HBV and having
hepatitis B vaccination Giving HBIG and vaccine within 12 hrs after birth
to infants born to HBV infected mothers Drug users should not share needles, syringes Not sharing personal care items like razors,
toothbrushes Avoiding tattoing or body piercing
19-01-201527
Healthcare workers should always follow universal precautions, safely handling needles and other sharps and being vaccinated
19-01-201528
Dental aspects Drugs should be used with caution There may be bleeding tendency if the platelet
count is low or if PT is prolonged Saliva may contain HBV Human bite can also transmit HBV Needlestick injury- 25% of these may transmit
HBV infection. HBIG should be given within 24 hours and 1st shot of hepatitis B vaccine
If adequate precautions are taken dental surgery is no longer a significant source of infection
Practitioners ill with hepatitis should stop dental practice until fully recovered.
19-01-201529
19-01-201530
Hepatitis C
Previously known as non A non B hepatitis
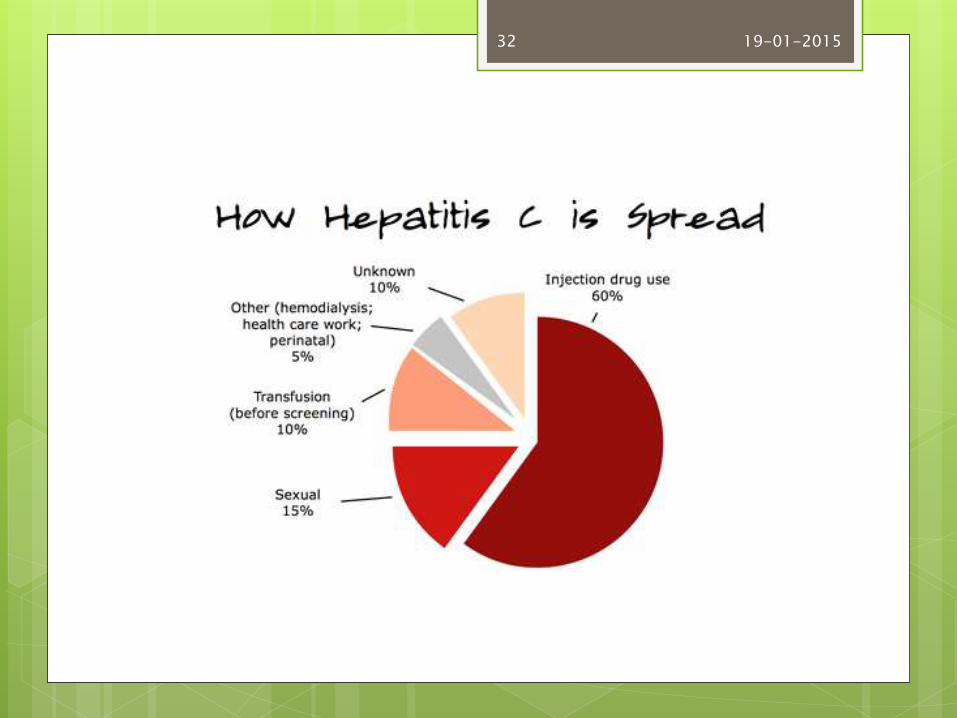
Transmission- blood and blood products
Persons at risk- those who have received blood from a donor who later tested positive for HCV, illegal IV drug user, long term renal dialysis, health care workers exposed to blood
19-01-201531
19-01-201532
C/f: 80-90% of infected persons have no signs or symptoms
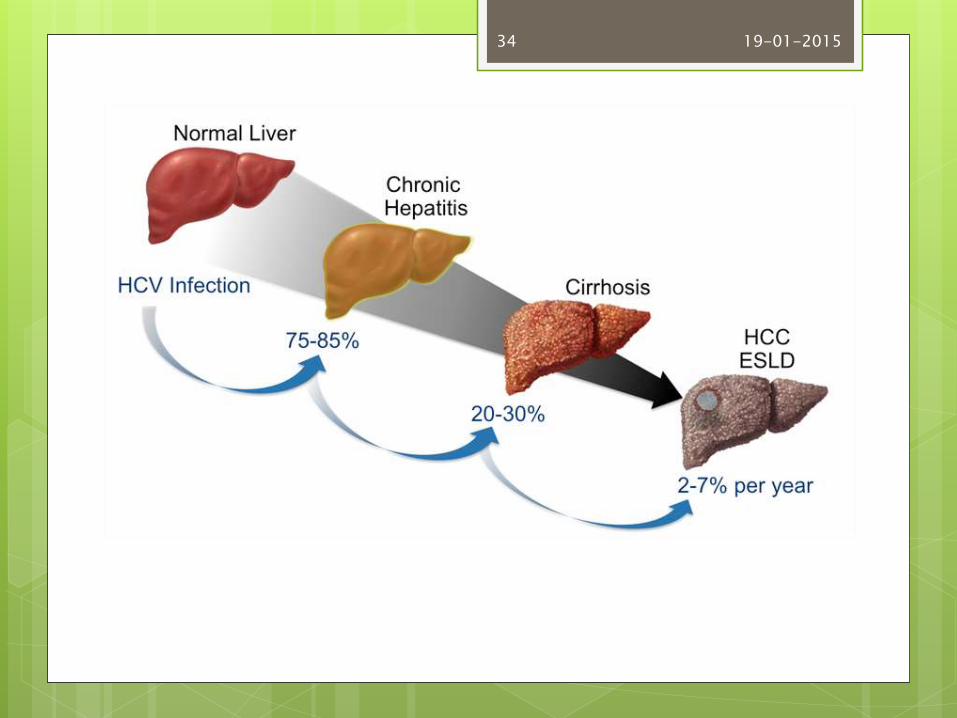
25-80% of pts with HCV have abnormal liver function tests after one year and may go on to chronic liver disease(up to 85%) or liver cancer or die(<3%)
Coinfection with HGV- 15%
19-01-201533
19-01-201534
General management
Serologic test (ELISA) are available to detect HCV
No vaccine available
Drug treatment with alpha interferon
Chronic HCV- combination of ribavirin plus interferon alpha
Prevention: routine barrier precautions and safely handling needles
19-01-201535
Dental aspects
HCV has been found in saliva
Transmitted in 10 % of needlestick injuries
Infected staff should not perform exposure prone procedures
The main salivary gland disorders associated with HCV infection are xerostomia, Sjögren’ssyndrome, lichen planus and
sialadenitis.
19-01-201536
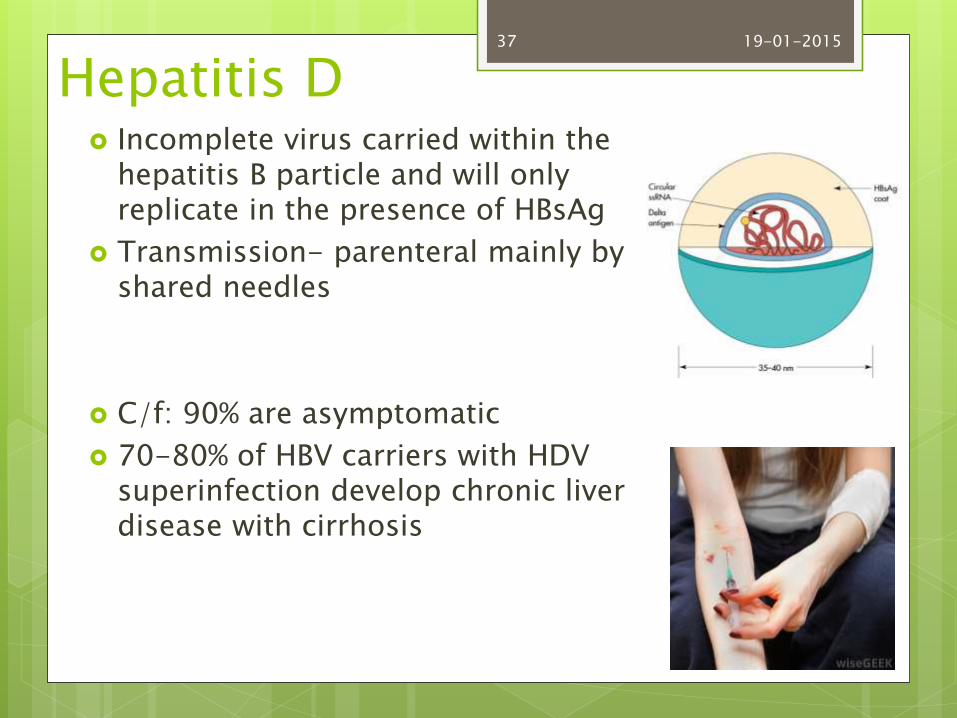
Hepatitis D Incomplete virus carried within the
hepatitis B particle and will only replicate in the presence of HBsAg
Transmission- parenteral mainly by shared needles
C/f: 90% are asymptomatic
70-80% of HBV carriers with HDV superinfection develop chronic liver disease with cirrhosis
19-01-201537
HDV antigen indicates recent infection and delta antibody indicates chronic hepatitis or recovery
Vaccination against HBV protects indirectly against HDV
Drug treatment with alpha interferon
19-01-201538

Hepatitis E
Spreads via feco-oral route
In developing countries with poor sanitation
Causes a disease similar to hepatitis A
High mortality in pregnant women (more than 40%)
Not known to be transmitted in dentistry
19-01-201539
Hepatitis Non A -E
Cases of acute hepatitis than appear to have viral origin but that cannot attributed to any known virus
This includes unknown viruses such as hepatitis F virus, hepatitis G virus and TTV
19-01-201540
Chronic hepatitis Persists longer than 6 months Causes: hepatitis B or C
autoimmuneAlcoholismwilsons diseasealpha 1 antitrypsin deficiency
Drugs: aspirincytotoxic agentshalothaneisoniazidmethyldopaacetaminophen
19-01-201541
Clinical features Many patients are asymptomatic Malaise Anorexia Fatigue Low grade fever Upper abdominal discomfortSigns: splenomegalySpider naeviAscitesFluid retentionJaundice
19-01-201542
19-01-201543
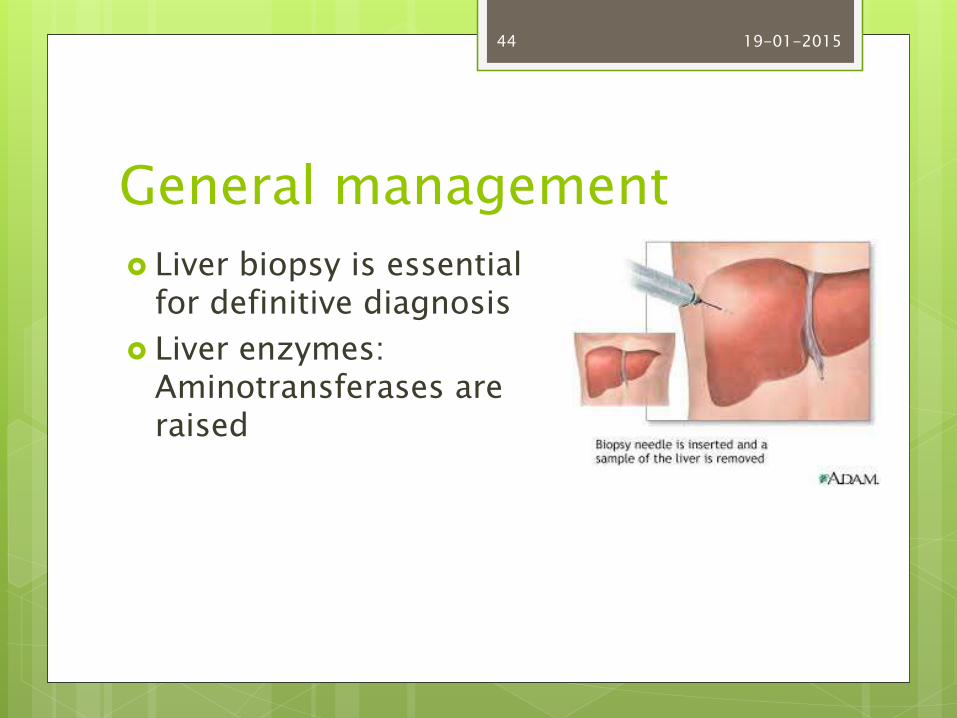
General management
Liver biopsy is essential for definitive diagnosis
Liver enzymes: Aminotransferases are raised
19-01-201544
Treatment includes withdrawl of causative drugs and management of complications
Chronic HBV /HCV: interferon alpha, lamivudine
Chronic HCV: ribavirine plus interferon alpha
Liver transplantation for advanced hepatitis C
19-01-201545
Hepatotoxic agents aspirin and paracetamol should be avoided
No common oral problems in chronic hepatits but sjogrens syndrome is relatively common and oral lichenoidlesions may develop
19-01-201546
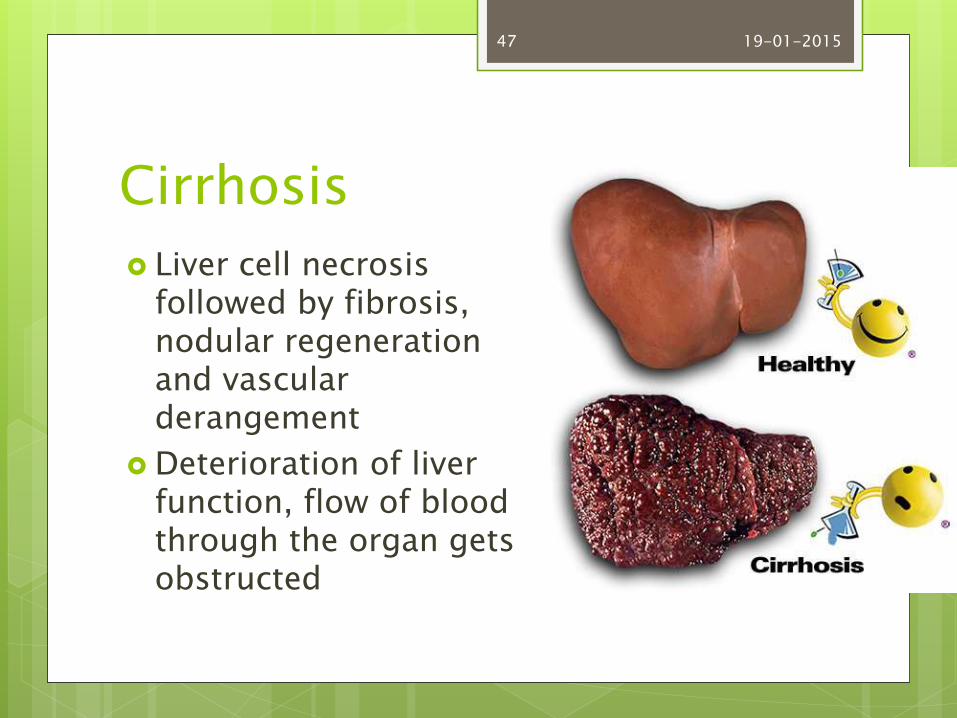
Cirrhosis
Liver cell necrosis followed by fibrosis, nodular regeneration and vascular derangement
Deterioration of liver function, flow of blood through the organ gets obstructed
19-01-201547
Causes of cirrhosis idiopathic alcoholism Hepatitis C,B,D Chronic hepatitis Primary biliary cirrhosis wilson’s disease alpha 1 antitrypsin deficiency congestive cardiac failure drugs
19-01-201548

C/F anorexia ,malaise, weight loss Jaundice Splenomegaly Ascites GI haemorrhage Palmer erythema Spider naevi Finger clubbing Opaque nails Pigmentation Fluid retention Bruising Gynaecomastia, testicular atrophy
19-01-201549
Alcoholic cirrhosis – parotid swelling
Dupuytren’s contracture
Gastric ulceration, or pancreatitis
Complications from hepatocellular damage and portal hypertension:
vomiting of blood
thrombocytopenia
bleeding tendency
anaemia
19-01-201550
General management
Serum bilirubin levels, immunoglobulins, transaminases and alkaline phosphatasemay be raised
Serum albumin is low
Prolonged PT
Thrombocytopenia, anaemia
Liver damage from cirrhosis cannot be reversed but treatment can stop or delay further progression
19-01-201551
Treatment of the cause
Treatment is directed towards prevention and treatment of complications
Liver transplantation when complications cannot be controlled
19-01-201552
Dental aspects
SBP is a potential problem in cirrhosis with ascites
Invasive dental or oral surgical procedures may increase the risk of SBP
Antibiotic prophylaxis should be considered
Amoxicillin orally 2-3g with metronidazole 1 h preop or intravenous imipenem are recommended
Some pts have sialosis, or tooth erosion from gastric regurgitation
19-01-201553
Drug induced liver disease
Dose related liver damage-alcohol, acetaminophen, tetracyclines, ketoconazole, isoniazid, methyldopa
Non dose related – erythromycin, halothane and sulfonamides , antithyroid drugs, phenytoin,nitrofurantoin
19-01-201554
Tetracyclines in massive doses can cause liver damage
Erythromycin estolate is potentially hepatotoxic but the effect is reversible when the drug is stopped
Halothane can cause hepatitis Halothane hepatitis causes pyrexia 1 week post op
and malaise , anorexia and jaundice may then appear
Halothane should never be given repeatedly or within a period of 3 months
Enflurane, isoflurane, desflurane and sevoflurane do not induce hepatitis in those who have had halothane hepatitis
19-01-201555
Aspirin: reye’s syndrome in children-liver damage with encephalopathy and abnormal accumulation of fat in the liver and other organs alone with a severe rise in intracranial pressure
Therefore it is contraindicated in children below 16 yrs
19-01-201556
Liver cancer
Fifth most common cancer worldwide
Cancer of the hepatocytes- hepatocellularcarcinoma or malignant hepatoma
It has been estimated that HBV and HCV are responsible for over 80% of all hepatocarcinomas.
Risk factors: old age, a positive family history, chronic HCV or HBV, cirrhosis , aflatoxin, long term oral contraceptive use
19-01-201557
Clinical features
Early stages- no symptoms
Later- wasting,
jaundice,
pain in the right upper abdomen,
swollen abdomen,
loss of appetite,
weakness,
nausea and vomiting ,
fever
19-01-201558
General management
Ultrasound, MRI scan , biopsy
High alpha fetoprotein levels
Treatment- surgical resection (partial hepatectomy)
Liver transplantation
19-01-201559
Extrahepatic biliaryobstruction
Causes- gall stones and Ca of pancrease
C/f-
Gall stones are often asymptomatic
Passage of the stones into the bile ducts can cause severe pain because of biliary colic, acute cholecystitis or acute pancreatitis
Jaundice, pruritus, dark urine and pale stools
Impaired absorption of fats and vitamin K
19-01-201560
General management
Diagnosis- ultrasound and endoscopic
Rise in serum bilirubin esters, alkaline phosphatase, 5’ nucleosidase, gamma glutamyl transpeptidase and transaminase
Treatment- lithotripsy,
Cholecystectomy
19-01-201561
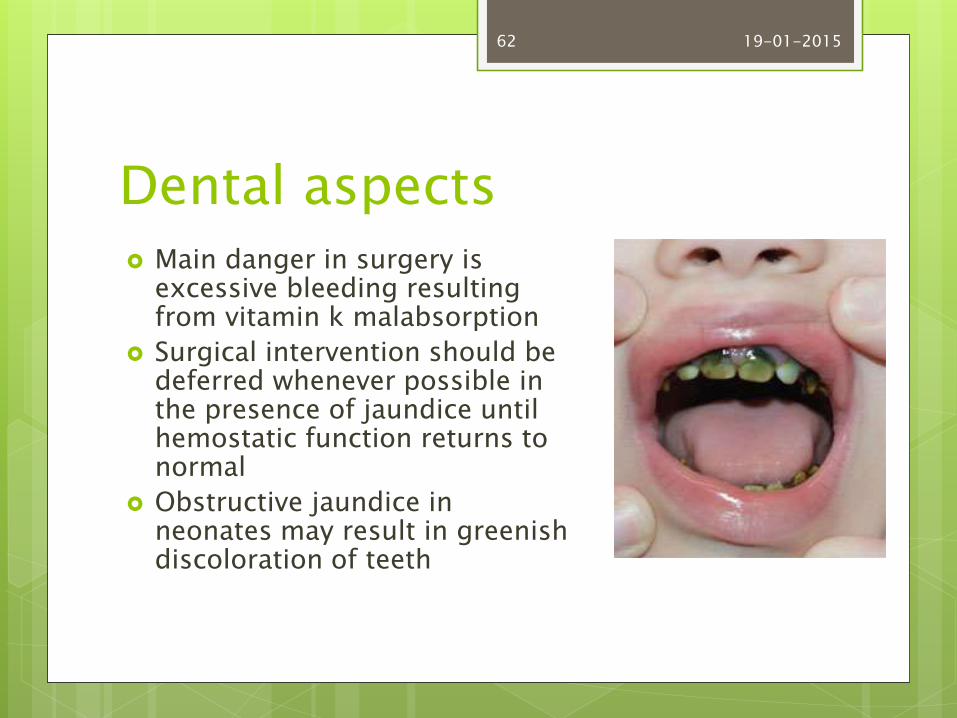
Dental aspects Main danger in surgery is
excessive bleeding resulting from vitamin k malabsorption
Surgical intervention should be deferred whenever possible in the presence of jaundice until hemostatic function returns to normal
Obstructive jaundice in neonates may result in greenish discoloration of teeth
19-01-201562
Alcoholic liver disease
Earliest change- fatty infiltrate, enlargement of liver (reversible)
Alcoholic hepatitis- diffuse inflammatory condition of liver with destructive cellular changes(irreversible)
Irriversible changes can lead to necrosis
Cirrhosis- progressive fibrosis and abnormal regeneration of liver architecture
Cirrhosis leads to liver failure
19-01-201563
Patients with alcoholic hepatitis can present glossitis, angular cheilitis and gingivitis, particularly in combination with nutritional deficiencies
Sialadenosis
19-01-201564
A patient with untreated alcoholic liver disease is not a candidate for outpatient dental care and should be referred to a physician.
Screening lab tests, including CBC, AST,ALT,PT should be ordered before the invasive procedures are performed
Use drugs with caution as metabolism may be impaired. Eg. Half the dose if cirrhosis or alcoholic hepatitis is present
There is risk of infection or spread of infection. Antibiotics should be prescribed when infection develops.
19-01-201565
Dental considerations of hepatitis
Dentists who are hepatits virus carriers:
The CDC suggests that health care professionals who perform invasive procedures should know their infectivity status
And if found positive for a blood transmissible virus, should not perform exposure prone procedures
19-01-201566
All patients with a history of viral hepatitis must be managed as though they are potentially infectious
All dental healthcare workers who provide patient care should receive vaccination against hepatitis B and should implement universal precautions
19-01-201567
Patients with active hepatitis: no dental treatment other than urgent care
Strict adherence to standard precautions
Aerosols should be minimized and drugs metabolized in the liver should be avoided.
If surgery is necessary, preop PT and BT should be obtained.
19-01-201568
Patients with history of hepatitis:
Most carriers of HBV,HCV and HDV are unaware that they have had hepatitis
Thus these pts are not identified with medical history and lab screening of all the pts is impractical
The only practical method of protection from these pts is to adopt a strict program of clinical asepsis for all patients
19-01-201569
Patients at high risk for HBV or HCV infection:
Screening for HBsAg and antiHAV
If a patient is found to be carrier, the patient may have undetected chronic active hepatitis, which could lead to bleeding complications and drug metabolism problems.
19-01-201570
:
19-01-201571
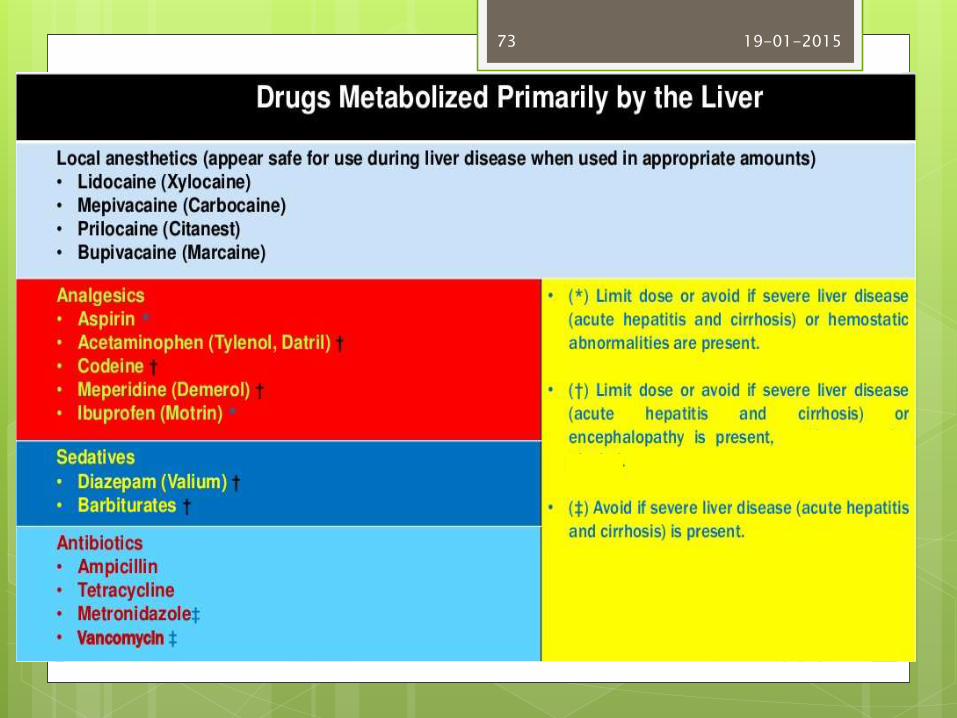
Drug administration
Drugs metabolized in the liver should be considered for diminished dosage when one or more of the following are present:
Aminotransferase levels elevated to greater than 4 times normal value
Serum bilirubin elevated to above 2mg/dL
Serum albumin levels lower than 35mg/L
Signs of ascites and encephalopathy and prolonged BT
19-01-201572
19-01-201573
Oral manifestations
The oral cavity can reflect liver dysfunction in the form of mucosal membrane jaundice, bleeding disorders, petechiae,
increased vulnerability to bruising, gingivitis, gingival bleeding (even in response to minimum trauma) foetorhepaticus (a characteristic odor of advanced liver disease), cheilitis, smooth and atrophic tongue, xerostomia, bruxism and crusted perioral rash
19-01-201574
Before any surgery is performed, the PT should be obtained
INR should be lower than 3.5
If it is more than 3.5, extensive surgical procedure should be postponed
19-01-201575
The most frequent problems associated with liver disease in clinical practice refer to the risk of viral contagion on the part of the dental professionals and rest of patients (cross-infection),
the risk of bleeding in patients with serious liver disease,
alterations in the metabolism of certain drugs which increases the risk of toxicity.
HCV has been detected on different surfaces within the dental clinic after treating patients with hepatitis C, and the virus is able to remain stable at room temperature for over 5 days
Strict sterilization measures are therefore required The universal protective measures are applicable
in order to prevent cross-infection, i.e., the use of barrier methods, with correct sterilization and disinfection measures
19-01-201576
The measures in the case of accidental perforation of the skin with instruments or needles comprise careful washing of the wound (without rubbing, as this may inoculate the virus into deeper tissues) for several minutes with iodine solution.
pressure should be applied beneath the level of the wound in order to induce bleeding and thus help evacuate any possible infectious material. If exposure through some mucosal membrane has occurred, abundant irrigation with sterile saline solution or sterile water is advised, for several minutes. The rationale behind these measures is to reduce the number of viral units to below the threshold count needed to cause infection (i.e., the infectious dose).
19-01-201577
In many cases, discrimination and stigma, or fear and past experience can prevent people with hepatitis B or C from accessing dental and other healthcare services.
Therefore, we should have a welcoming and nonjudgmental approach to treating all patients to ensure the provision of effective healthcare and follow-up.
Prevention is an important aspect in controlling the spread of this viral infection as an epidemic. Knowing facts, having proper awareness, and proper behavior and attitude toward clinical aspects of the infection and toward the patients are critical to prevent the spread of these infections.
19-01-201578
Setia, et al. : Hepatitis B and C infection in dentistry and its management, Eur J Gen Dent 2013;2:13-9
Medical problems in dentistry, 5th edition, Crispian Scully, Roderick Cawson
Robbins basic pathology, 9th edition
Little,J.W, dental management of medically compromised patients
19-01-201579

Thank you !
19-01-201580