Embed Size (px)
Citation preview
Heart AttacksThe Cause
AbstractObjective The aim of this study was to determine the extent of drug interactions affecting levothyroxine, using study drugs often co-administered to patients on long-term levothyroxine therapy.Design A retrospective population analysis linking biochemistry and prescription data between 1 January 1993 and 31 December 2012 was used.Patients The study population was Tayside residents prescribed levothyroxine on at least three occasions, within a six-month period, prior to the start of a study drug. Individuals acted as their own controls pre- and postinitiation of study drug. Overall, 10 999 patients (mean age 58 years, 82% female) being treated with thyroxine were included in the study.Measurements Changes in TSH following initiation of study drug.Results Iron, calcium, proton pump inhibitors and oestrogen all increased serum TSH concentration: an increase of 0·22 mU/l (P < 0.001), 0·27 mU/l (P < 0·001), 0·12 mU/l (P < 0·01), and 0·08 mU/l (P < 0·007), respectively. For these four study drugs, there was a clinically significant increase of over 5 mU/l in serum TSH, in 7·5%, 4·4%, 5·6% and 4·3% patients, respectively. There was a decrease of 0·17 mU/l (P-value 0.01) in the TSH concentration for those patients on statins. The TSH decreased by 5 mU/l in 3·7% of patients. There was no effect with H2 receptor antagonists or glucocorticoids.Conclusion This large population-based study demonstrates significant interaction between levothyroxine and iron, calcium, proton pump inhibitors, statins and oestrogens. These drugs may reduce the effectiveness of levothyroxine, and patients' TSH concentrations should be carefully monitored.
Theory: Most heart attacks are caused by the blockage caused by plaque buildup in the four major coronary arteries supplying the heart
These plaques are composed of cholesterol that built up in the arterial lumen (inside of the artery)
which eventually cut off blood supply to a certain area of the heart, resulting in oxygen deficiency in that area,
causing first pain (angina), then progressing to ischemia (heart attack).
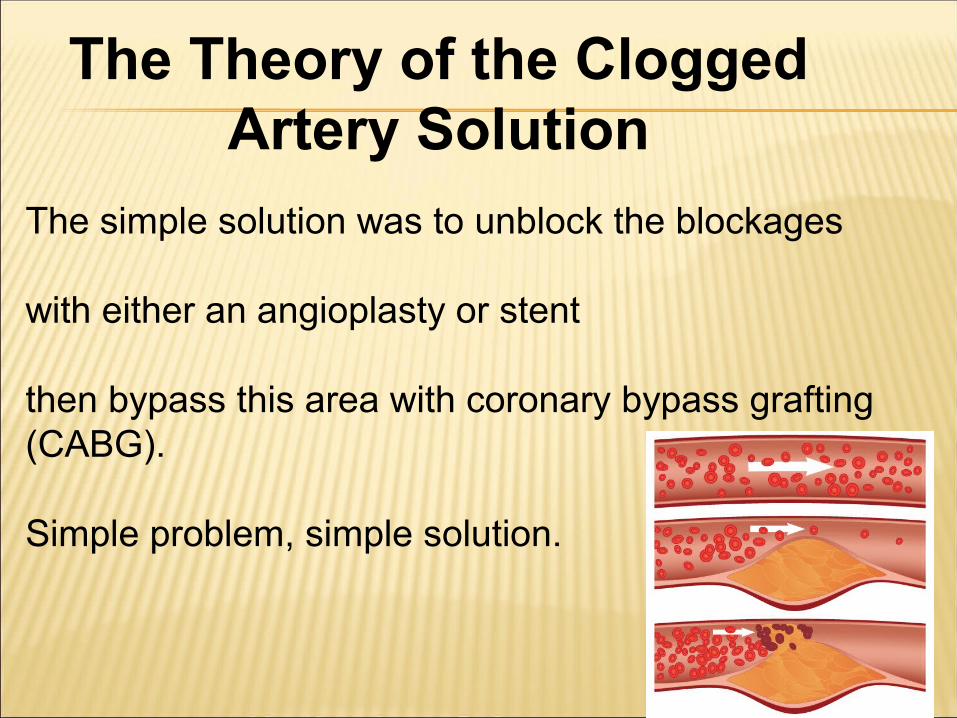
The simple solution was to unblock the blockages
with either an angioplasty or stent
then bypass this area with coronary bypass grafting (CABG).
Simple problem, simple solution.
The Theory of the Clogged Artery Solution
The first major autopsy study of patients dying of MI was carried out in Heidelberg in the 1970s. The study found that sufficient thrombosis to cause the MI was found in only 20 percent of cases Doerr W, et al.: Springer, Berlin-Heidelberg- New York, 1974.
The largest such study found sufficient thrombosis in only 41 percent of cases. The Etiopathogenesis of Coronary Heart Disease: A Heretical Theory Based on Morphology, Eurekah. com, Landes, Bioscience, 2004.
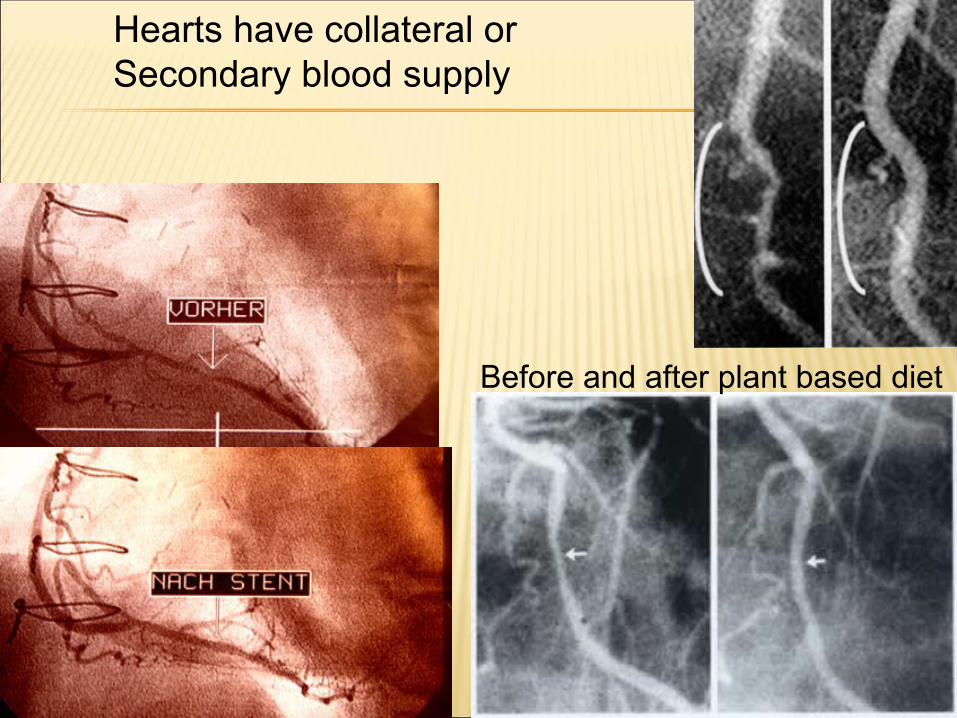
Before and after plant based diet
Hearts have collateral or Secondary blood supply
Acute unstable angina: 90s’, heart attacks were redefined
Pre 90’s three criteria for diagnosing a heart attack: •typical heart complaints•typical alterations in the ECG•certain blood values
New definition the alterations in the ECG were omitted and the indicators in the blood were reduced to a single item “troponin”
NSTEMI: N = non, STE = ST elevation (a typical sign of heart attack in the ECG), and MI = myocardial infarction (heart attack) This is a heart attack that is not seen on the ECG. It is an acute heart attack in its developing phase, before the ECG shows the destruction of the tissue that takes place in the following minutes or hours.
troponin
“NSTEMI” is based on the slight rise in “troponin”
•released into the bloodstream during a heart attack•also after an attack of acute angina pectoris•excitement ,adrenaline, with alcohol, can increase troponin•not unusual in daily life
A heart seizure, leads to a slight rise in troponin levels about 4 hours later.
If the patient is taken to a clinic, the emergency doctor will diagnose a “NSTEMI heart attack. And calls for the immediate use of the heart catheter.
nearly always find alterations to the coronary vessels during catheterization, which retrospectively validify the intervention.
the vessel is then widened with a balloon and a stent is inserted.
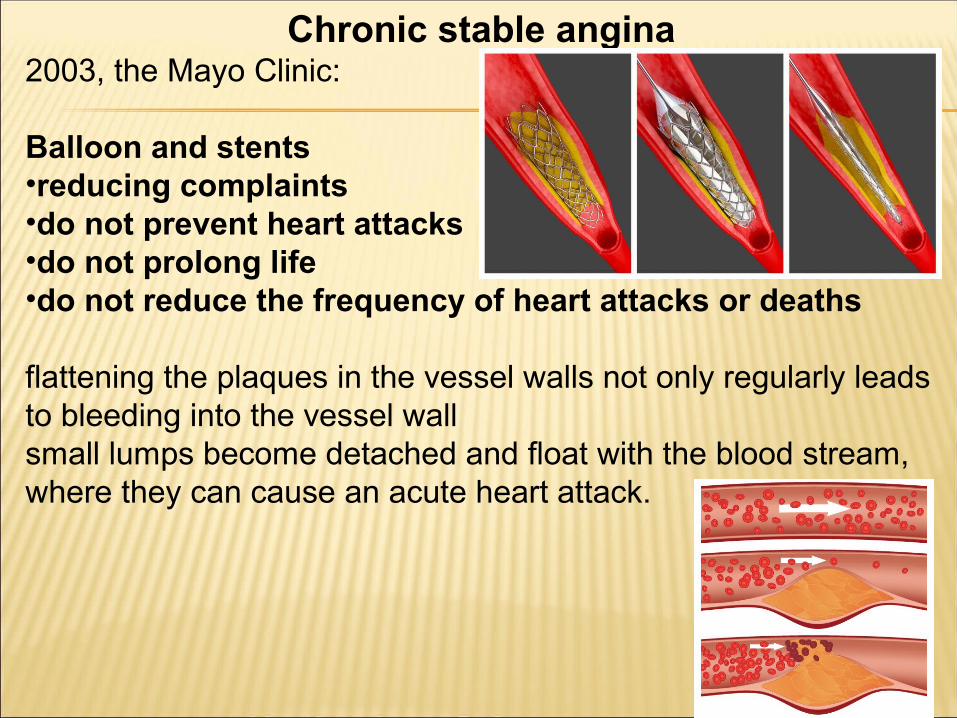
Chronic stable angina 2003, the Mayo Clinic:
Balloon and stents•reducing complaints•do not prevent heart attacks•do not prolong life•do not reduce the frequency of heart attacks or deaths
flattening the plaques in the vessel walls not only regularly leads to bleeding into the vessel wallsmall lumps become detached and float with the blood stream, where they can cause an acute heart attack.
New England Journal of Medicine. Cindy L. Grines, M.D., Beaumont cardiologist,
•worldwide study that involved 900 patients at 62 centers. •All patients in the study were treated within 12 hours of their heart attack.
•a higher death rate (4.2% Stent & angioplasty vs. 2.7% angioplasty)•They also unexpectedly experienced decreased blood flow following stent placement.
•Dr. Grines says "The higher mortal ity rate and decrease in blood f low makes it necessary for addit ional research to be conducted before routine stenting can be recommended as a standard of care."
•Dr. Grines says that the study also offers no evidence that routine stent placement after a heart attack wil l reduce future complications such as stroke or another heart attack.
•evaluation the use of catheterization in chronic stages of heart disease. •RITA 2” precisely shows the uselessness and potential damage that can be caused by this intervention in chronic heart disease.
•Although catheterization and stents had been claimed to be life-saving measures, they do not prevent heart attacks or save lives. this intervention is accompanied by a great placebo effect.
J Am Coll Cardiol. 2003 Oct 1;42(7):1161-70.Seven-year outcome in the RITA-2 trial: coronary
angioplasty versus medical therapy.
5-Year Clinical Outcomes in the ICTUS (Invasive versus Conservative Treatment in Unstable coronary Syndromes)
TrialA Randomized Comparison of an Early Invasive Versus Selective Invasive Management in Patients With Non–ST-
Segment Elevation Acute Coronary Syndrome J Am Coll Cardiol. 2010;55(9):858-864.
doi:10.1016/j.jacc.2009.11.026
Objectives We present the 5-year clinical outcomes according to treatment strategy with additional risk stratification of the ICTUS (Invasive versus Conservative Treatment in Unstable coronary Syndromes) trial.
Conclusions ….we could not demonstrate a long-term benefit of an early invasive strategy in reducing death or MI. (Invasive versus Conservative Treatment in Unstable coronary Syndromes [ICTUS
The average death rate for bypass surgery is greater than the average death rate of heart patients treated without surgery.
Heart disease progresses faster in those who have had invasive surgery than in those treated non-surgically.
Heart Surgery kills thousands of patients per year and debilitates thousands more.
The first major autopsy study of patients dying of MI was carried out in Heidelberg in the 1970s. The study found that sufficient thrombosis to cause the MI was found in only 20 percent of cases Doerr W, et al.: Springer, Berlin-Heidelberg- New York, 1974.
The largest such study found sufficient thrombosis in only 41 percent of cases. The Etiopathogenesis of Coronary Heart Disease: A Heretical Theory Based on Morphology, Eurekah. com, Landes, Bioscience, 2004.
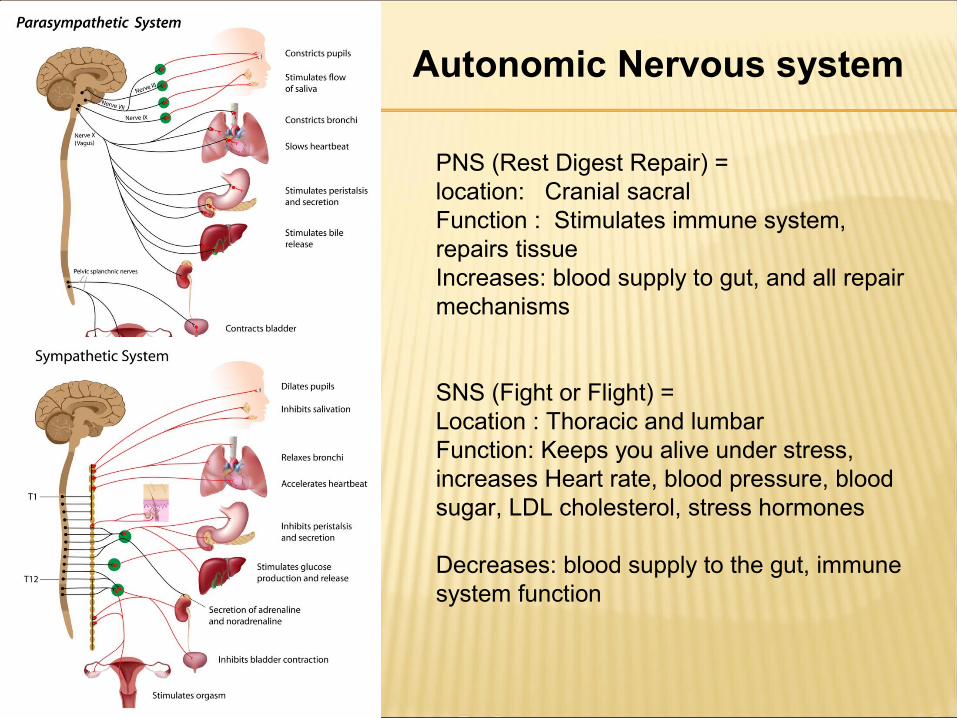
Autonomic Nervous system
PNS (Rest Digest Repair) = location: Cranial sacralFunction : Stimulates immune system, repairs tissueIncreases: blood supply to gut, and all repair mechanisms
SNS (Fight or Flight) = Location : Thoracic and lumbar Function: Keeps you alive under stress, increases Heart rate, blood pressure, blood sugar, LDL cholesterol, stress hormones
Decreases: blood supply to the gut, immune system function
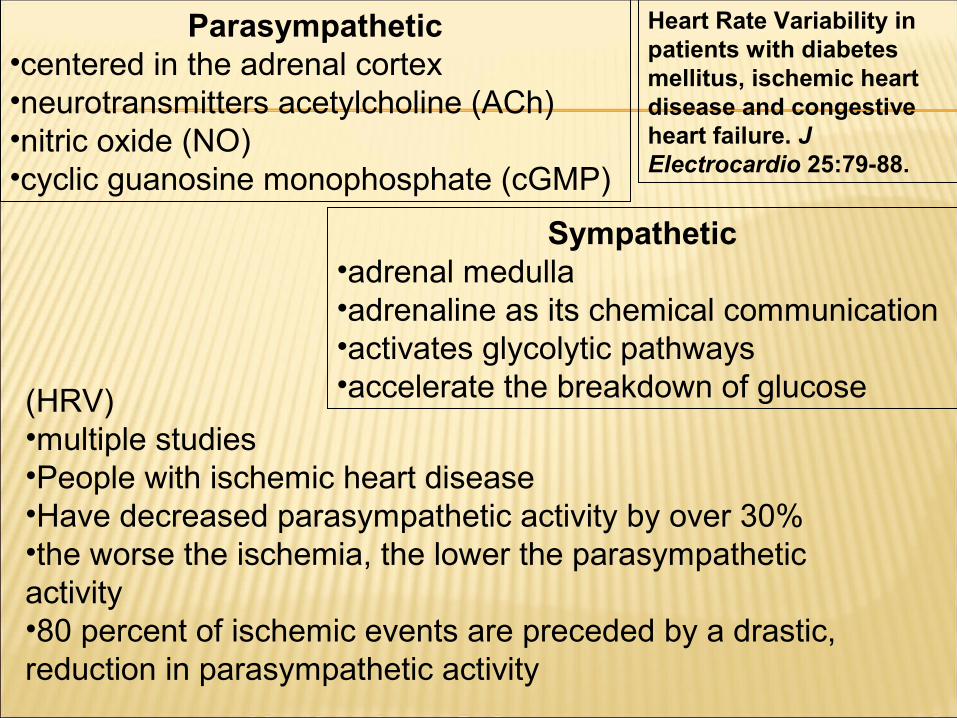
Parasympathetic•centered in the adrenal cortex•neurotransmitters acetylcholine (ACh)•nitric oxide (NO)•cyclic guanosine monophosphate (cGMP)
Sympathetic•adrenal medulla•adrenaline as its chemical communication •activates glycolytic pathways•accelerate the breakdown of glucose(HRV)
•multiple studies•People with ischemic heart disease•Have decreased parasympathetic activity by over 30%•the worse the ischemia, the lower the parasympathetic activity•80 percent of ischemic events are preceded by a drastic, reduction in parasympathetic activity
Heart Rate Variability in patients with diabetes mellitus, ischemic heart disease and congestive heart failure. J Electrocardio 25:79-88.
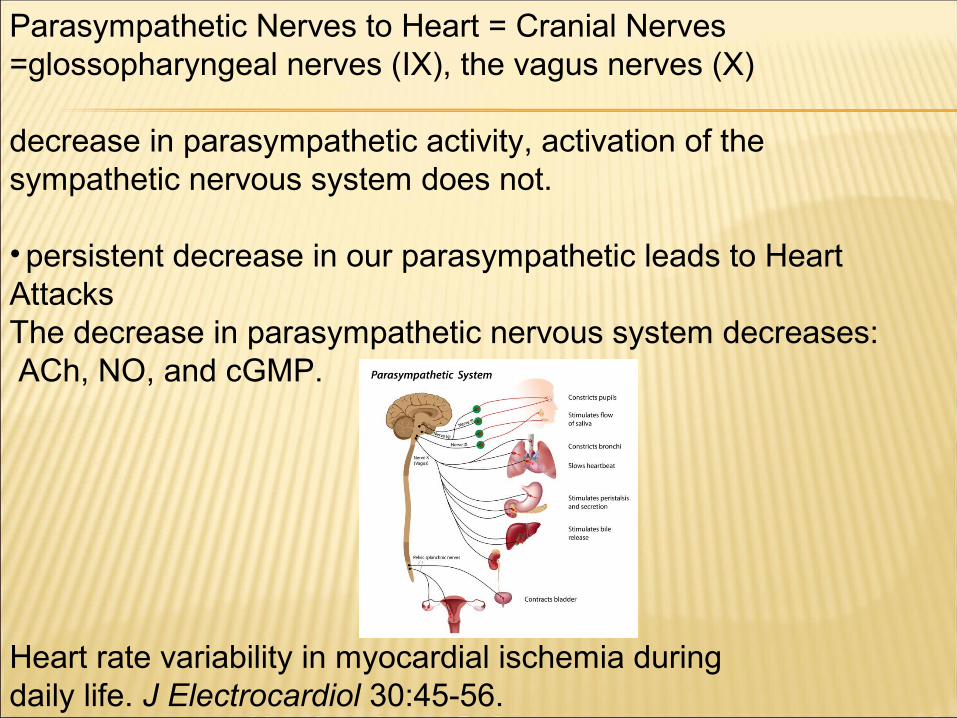
Parasympathetic Nerves to Heart = Cranial Nerves =glossopharyngeal nerves (IX), the vagus nerves (X)
decrease in parasympathetic activity, activation of the sympathetic nervous system does not.
• persistent decrease in our parasympathetic leads to Heart AttacksThe decrease in parasympathetic nervous system decreases: ACh, NO, and cGMP.
Heart rate variability in myocardial ischemia during daily life. J Electrocardiol 30:45-56.
women have stronger vagal (X) activity than menWomen have lower heart attack rates
Average age of death due to heart disease: 74.4 years for men81.9 years for women42.0 percent of male heart disease deaths under 75yo21.1 percent of female heart disease deaths under 75yo
Causes decrease in Parasympathetic or Vagal activities:•Hypertension •Smoking•Diabetes•physical and emotional stress
• signals the vasomotor center in the brain to change the blood pressure by dilating or constricting the blood vessels
• decreasing or increasing, heart rate • abnormal heart rhythms
Medications used in cardiology upregulate the parasympathetic nervous system
•Nitrates stimulate NO production•aspirin and statin drugs also stimulate the production of Ach, NO
These Medications cause a rebound decrease in these substances making
the parasympathetic activity even worse
•Beta-blockers block the sympathetic nervous system, the increasing Heart attack risk
National Institute for Health Research Health Technology Assessment (NIHR HTA)
benefits of taking aspirin each day• 10% to 15% drop in coronary heart disease.• 33-46 fewer deaths per 100,000
adverse effects of aspirin
•37% increase in gastrointestinal bleeding (68-117 per 100,000) •32%-38% increase ..hemorrhagic stroke (8-10 per 100,000)
Aileen Clarke, Professor of Public Health Research and Director of Warwick Evidence at
Warwick Medical School, said, “…clear that there is an incredibly fine balance between the possible benefits and risks of the intervention. We need to be extremely careful about over-promoting aspirin intervention without having first fully understood these negative side effects.”
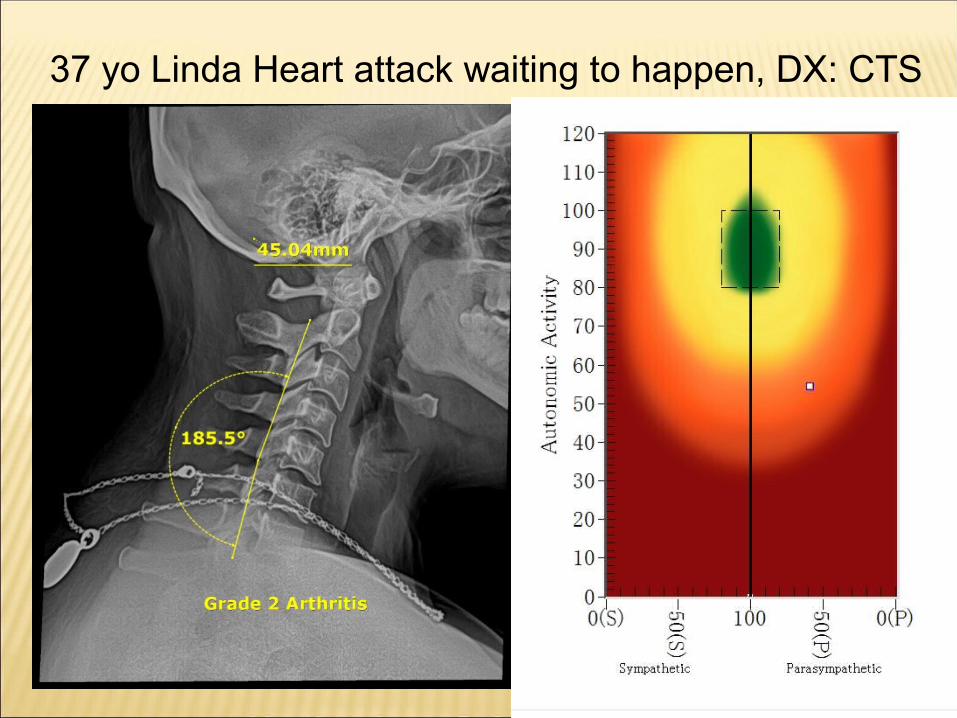
37 yo Linda Heart attack waiting to happen, DX: CTS
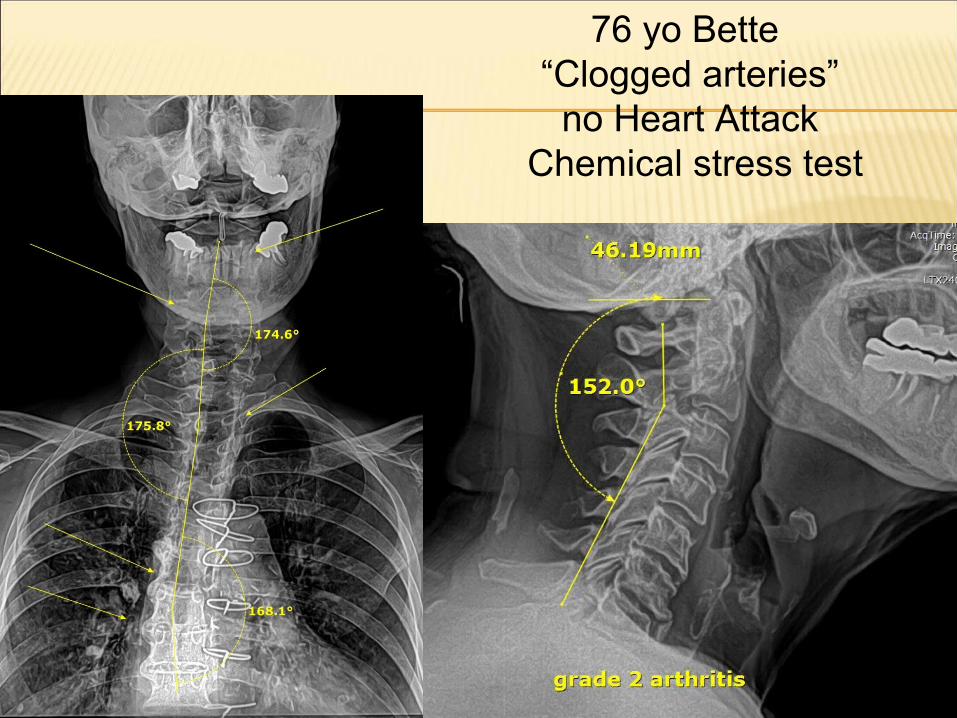
76 yo Bette “Clogged arteries” no Heart Attack
Chemical stress test
They advise to use: Liquid vegetable oils such as canola, safflower, sunflower, soybean, and olive.
They advise to use egg whites or egg white substitutes.
AMERICAN HEART ASSOCIATION SAYS SO...
Deadly Advice
Healthy Diet / food 1:1 to 3:1 Disease start at 8:1 American Diet 20:1 Corn oil 60:1 safflower oil 77:1
soybean, sunflower, Corn, Peanut, Cottonseed, Grape seed, Canola.
omega-6 and low omega-3 fats profile in these oils (as much as 200:1!)
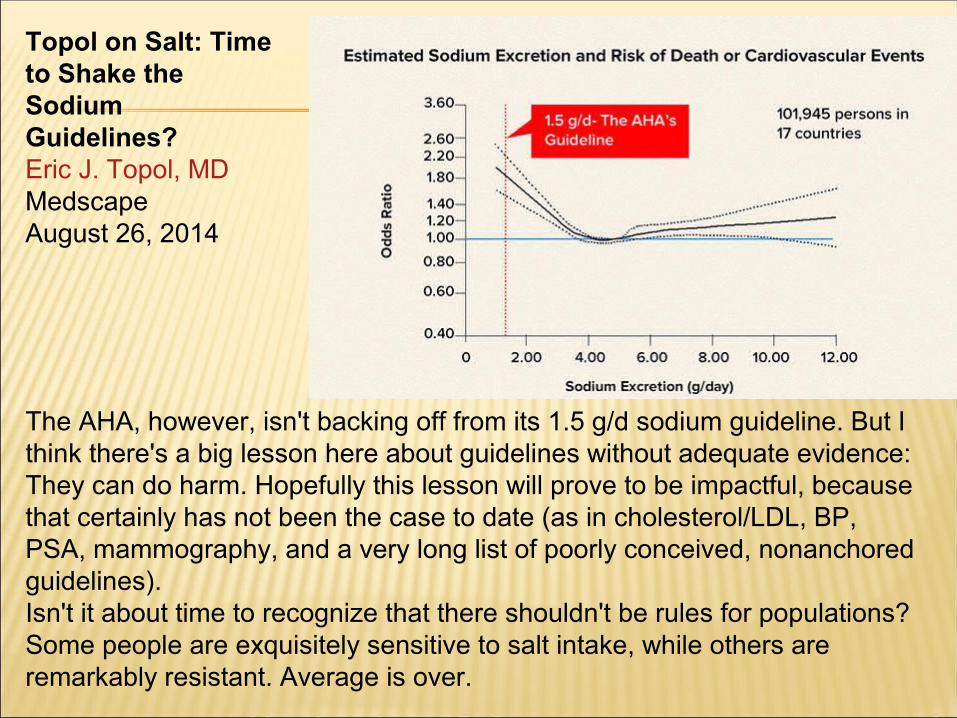
The AHA, however, isn't backing off from its 1.5 g/d sodium guideline. But I think there's a big lesson here about guidelines without adequate evidence: They can do harm. Hopefully this lesson will prove to be impactful, because that certainly has not been the case to date (as in cholesterol/LDL, BP, PSA, mammography, and a very long list of poorly conceived, nonanchored guidelines).Isn't it about time to recognize that there shouldn't be rules for populations? Some people are exquisitely sensitive to salt intake, while others are remarkably resistant. Average is over.
Topol on Salt: Time to Shake the Sodium Guidelines?Eric J. Topol, MDMedscapeAugust 26, 2014
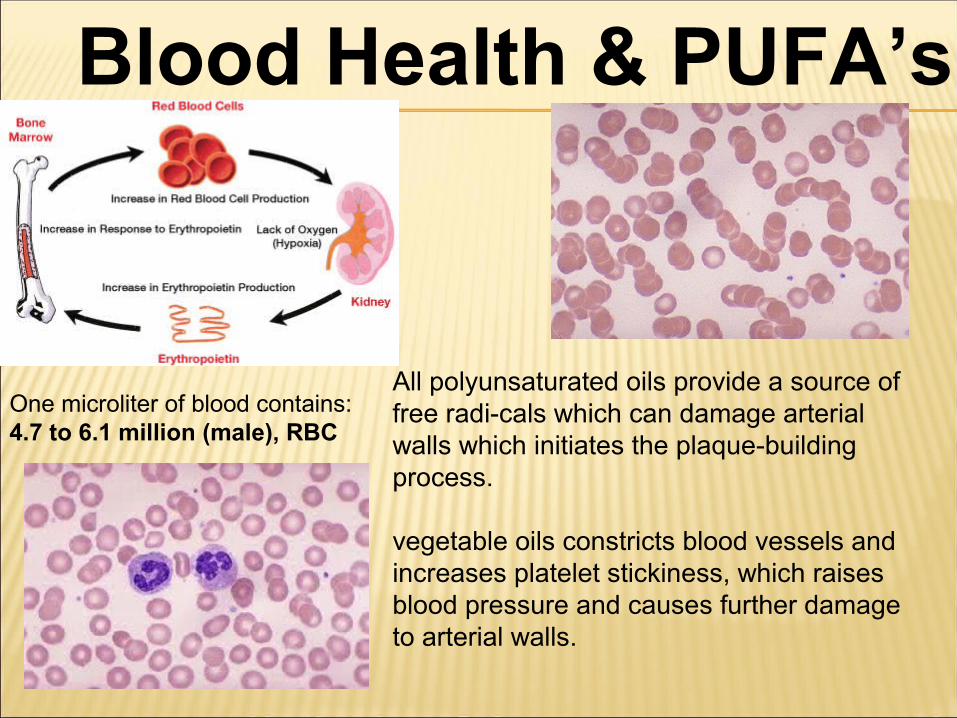
Blood Health & PUFA’s
One microliter of blood contains:4.7 to 6.1 million (male), RBC
All polyunsaturated oils provide a source of free radi-cals which can damage arterial walls which initiates the plaque-building process.
vegetable oils constricts blood vessels and increases platelet stickiness, which raises blood pressure and causes further damage to arterial walls.
(NSAIDs) caused a greater than 10-fold increase in the risk of Congestive Hear t Failure (CHF)
Archives of Internal Medicine June 2000; 160: 777-784.
The study followed more than 80,000 women between the ages of 31 and 50 years who were initially hypertension-free.
two years later women who used NSAIDs 22 days or more per month, the risk of high-
blood pressure increased some 86 percent.
Nonetheless, it was concluded that a large portion of U.S. hypertension cases may be the result of over-using these pain medications
Archives of Internal Medicine. October 28, 2002;162:2204-
2208
Sudden death after radiofrequency ablation of the atrioventricular node in patients with atrial
fibrillation J Am Coll Cardiol. 2002;40(1):105-110. doi:10.1016/S0735-1097(02)01927-7
Results Of 334 consecutive patients with AF who underwent AV node ablation, nine had sudden death after the ablation…. Conclusions Sudden death likely or possibly related to catheter ablation occurred in 7 of 334 patients (2.1%). Risk of sudden death is highest within two days after the procedure.
Proper nerve supply – FREE of subluxation
Regular Exercise
Proper Nutrition
Sufficient Rest
Prayer and Meditation
Keep Informed, Stay Healthy:

www.owners-guide.com
Free 7 day TrialFree access if You Are a
Bergman Family Chiropractic Patient
VIDEOS
Handouts
Private
Power
Points
Take Action TodayDisease Risk Assessment is $275.00
5 Step Disease Risk Assessment!!
•Disease Proof your Body•Get Your Vitality Back•Feel Young Again•Reduce or Eliminate Your Dependency on Rx
Only $99
The The ChiropractiChiropracti
c c AdjustmentAdjustment
HEART RATE VARIABILITYThe real revolution in the prevention and treatment of heart disease will come with increased understanding of the role played by the autonomic nervous system in the genesis of ischemia and its measurement through the tool of heart rate variability (HRV).We have two distinct nervous systems: the first, the central nervous system (CNS), controls conscious functions such as muscle and nerve function; the second nervous system, the autonomic (or unconscious) nervous system (ANS), controls the function of our internal organs. The autonomic nervous system is divided into two branches, which in a healthy person are always in a balanced yet ready state. The sympathetic or “fight-or-flight” system is centered in our adrenal medulla; it uses the chemical adrenaline as its chemical transmission device and tells our bodies there is danger afoot—time to activate and run. It does so by activating a series of biochemical responses, the centerpiece of which is the glycolytic pathways, which accelerate the breakdown of glucose to be used as quick energy as we make our escape from the bear chasing us.In contrast, the parasympathetic branch, centered in the adrenal cortex, uses the neurotransmitters acetylcholine (ACh), nitric oxide (NO), and cyclic guanosine monophosphate (cGMP) as its chemical mediators; this is the “rest-and-digest” arm of the autonomic nervous system.The particular nerve of the parasympathetic chain that supplies the heart with nervous activity is called the vagus nerve; it slows and relaxes the heart, whereas the sympathetic branches accelerate and constrict the heart. I believe it can be shown that an imbalance in these two branches is responsible for the vast majority of heart disease.Using the techniques of heart rate variability (HRV) monitoring, which gives a real-time accurate depiction of autonomic nervous system status, researchers have shown in multiple studies5 that patients with ischemic heart disease have on average a reduction of parasympathetic activity of over one-third. Typically, the worse the ischemia, the lower the parasympathetic activity.6 Furthermore about 80 percent of ischemic events are preceded by a significant, often drastic, reduction in parasympathetic activity.7