Embed Size (px)
DESCRIPTION
Citation preview
Trauma Rounds Case Reports from the Mass General Hospital and Brigham & Women’s Hospital A Quarterly Case Study Volume 4, Fall 2012
Chris Evans, PhD
Vaida Glatt, PhD
Large segmental defects heal poorly and often present clinical challenges. Approaches used to improve healing include auto-graft and allograft bone, distraction osteogenesis, vascularized bone grafts and the application of BMP-2 and BMP-7. We wanted to determine whether modulation of the mechanical environment could improve bone healing in a rat femoral seg-mental defect model.
The responsiveness of bone to mechanical stimulation has been known for well over a century, and there is a considerable body of literature describing its influence on fracture healing. Sur-prisingly, we could find no prior literature concerning the re-sponses of large segmental defects to their mechanical envi-ronment. To remedy this, we developed customized external fixators of different stiffness for use in conjunction with a 5 mil-limeter (mm) femoral defect in the rat. The external fixator de-sign allows the stiffness to be changed on living animals as they heal.
The concept of modulating the rigidity of fixation to promote bone healing goes back to the late 1970’s when Dr. Giovanni de Bastiani of the University of Verona, Italy, proposed the applica-tion of “dynamization” for external fracture fixation treatment. According to Dr. de Bastiani’s concept, the fracture site is ini-tially fixed very rigidly to provide stability and to allow healing to commence. Once woven bone is laid down, the fixator is loosened to allow the bone to bear greater load and thus re-model more rapidly. Based upon certain information from the literature, we won-dered whether the healing of large segmental defects would benefit from the opposite strategy – loose fixation first, followed
by rigid fixation. This is called reverse dynamization. We tested the reverse dynamization process in the study described here.MethodsFive mm, critical-sized, mid-femoral defects were created in rats. These do not spontaneously heal, but do heal in response to 11 !g recombinant, human BMP-2.We maintained groups of rats for 8 weeks with fixators of low (114 N/mm), medium (185 N/mm) and high (254 N/mm) stiff-ness. An additional group underwent reverse dynamization, where low stiffness fixation was applied for the first 2 weeks, after which time we imposed high stiffness fixation. All defects also received BMP-2.Animals were euthanized at 8 weeks. Healing was assessed by radiologic evaluation, mechanical testing, histology, dual-energy ray absorptiometry (DXA) and !CT. Results
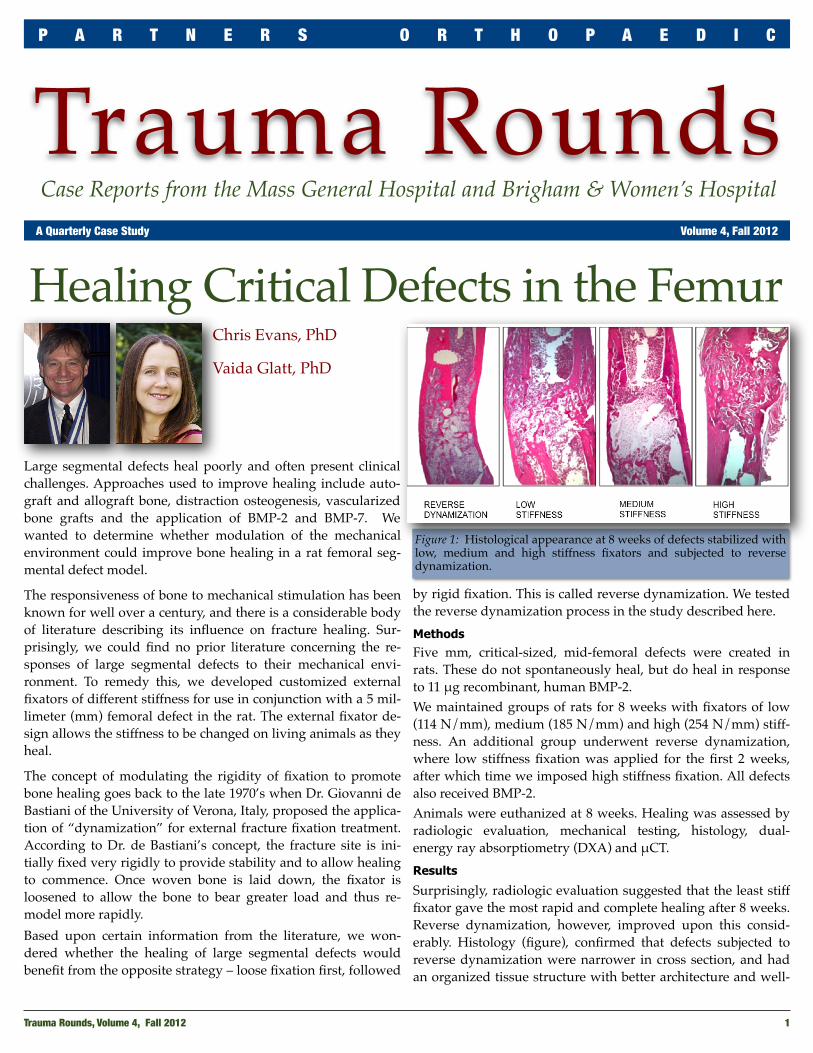
Surprisingly, radiologic evaluation suggested that the least stiff fixator gave the most rapid and complete healing after 8 weeks. Reverse dynamization, however, improved upon this consid-erably. Histology (figure), confirmed that defects subjected to reverse dynamization were narrower in cross section, and had an organized tissue structure with better architecture and well-
Trauma Rounds, Volume 4, Fall 2012 1
P A R T N E R S O R T H O P A E D I C
Healing Critical Defects in the Femur
Figure 1: Histological appearance at 8 weeks of defects stabilized with low, medium and high stiffness fixators and subjected to reverse dynamization.

formed evenly distributed neocortices, and only a small amount of trabecular bone. All other defects had persistent callus, and contained disorganized woven bone with poor cortication. De-fects stabilized for 8 weeks with medium stiffness fixators con-tained a central gap in the defect surrounded by unmineralized soft tissue. Defects stabilized for 8 weeks with the highest stiff-ness fixator contained a prominent band of cartilage, raising the possibility of developing into a non-union. Cartilage was not seen in any of the other groups at 8 weeks.The !CT, DXA and mechanical testing data were in broad agreement with the radiological and histological data.Discussion
These data support the concept of reverse dynamization to im-prove the healing of large segmental defects. Only one regimen of reverse dynamization was evaluated in this study. It is pos-sible that a different stiffnesses or timing of reverse dynamiza-tion would provide even better results. Optimization of the strategy remains a future goal.Although these experiments used a rat model, the results are relevant to clinical orthopaedics. They show that the healing of critical-sized segmental defects is highly responsive to the am-bient mechanical environment. The use of reverse dynamization runs counter to present clinical practice, where large segmental defects are subject to immediate rigid fixation. Further study of reverse dynamization could lead to improved clinical manage-ment of patients with these difficult injuries. Future ResearchUsing funding from the Department of Defense we are deter-mining whether reverse dynamization reduces the need for BMP-2 to achieve healing, and whether it accelerates the acqui-sition of mechanical strength. The former would reduce health care costs and the latter would allow earlier load bearing. We have also applied for additional funding to undertake a study of reverse dynamization in sheep.
FundingSupported by the AO Foundation (Grant S-08-42G) and the De-partment of Defense (Grant W81XWH-10-1-0888).
Christopher Evans, PhD, is the Maurice Mueller Professor of Orthopaedic Surgery and Director of the Center for Advanced Orthopaedic Studies in the Department of Orthopaedic Surgery at Beth Israel Deaconess Medical Center.
Vaida Glatt, PhD, is a Senior Research Fellow with the Trauma Research Group of the Institute of Health and Biomedical Innovation at Queensland University of Technology Brisbane, Queensland.
References1. This short brief was excerpted from this detailed manuscript: Glatt V, Miller
M, Ivkovic A, Liu F, Parry N, Griffin D, Vrahas M, Evans C. Improved heal-ing of large segmental defects in the rat femur by reverse dynamization in the presence of bone morphogenetic protein-2. J Bone Joint Surg Am. 2012 Nov 21;94 (22):2063-2073.
2. This study was performed in partial fulfillment of a PhD degree from the University of Warwick, UK, granted to Vaida Glatt.
P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S
2 Trauma Rounds, Volume 4, Fall 2012
Trauma FacultyMark Vrahas, MD — 617-726-2943Partners Chief of Orthopaedic [email protected]
Mitchel B Harris, MD — 617-732-5385Chief, BWH Orthopedic [email protected] Malcolm Smith, MD, FRCS — 617-726-2794Chief, MGH Orthopaedic [email protected] Lhowe, MD — 617-724-2800MGH Orthopaedic [email protected]
Michael Weaver, MD — 617-525-8088BWH Orthopedic [email protected]
Jesse Jupiter, MD — 617-726-5100MGH Hand & Upper Extremity [email protected]
David Ring, MD — 617-724-3953MGH Hand & Upper Extremity [email protected]
Brandon E Earp, MD — 617-732-8064BWH Hand & Upper Extremity [email protected]
George Dyer, MD — 617-732-6607BWH Hand & Upper Extremity [email protected]
John Kwon, MD — 617-643-5701MGH Foot & Ankle [email protected]
Please share your comments online, or by email:Mark Vrahas, MD / [email protected] Center for Outpatient Care, Suite 3C55 Fruit Street, Boston, MA 02114
Editor in Chief Mark Vrahas, MD
Program DirectorSuzanne Morrison, MPH(617) [email protected]
Editor, PublisherArun Shanbhag, PhD, MBAwww.MassGeneral.org/orthowww.BrighamAndWomens.org/orthopedics
AchesAndJoints.org/TraumaRead archives of all previous issues
New England Regional Fracture Summit, Stowe, VTThe annual AO Fracture Summit will be held January 18 – 21, 2013 in Stowe, VT. The course is chaired by Drs Mark Vrahas, Jesse Jupiter and Raymond White, and features several Harvard Orthopaedic Faculty. This year’s special guest will be the renowned foot and ankle surgeon, Sigvard Hansen, MD, of Harborview Medical Center, Seattle, WA. The course uses an informal, discussion-based, highly interactive format. The chief aim is to educate community orthopaedic surgeons who are actively involved in the treatment of patients with fractures. Partici-pants are invited to bring their own cases for discussion.
Registration is still open!For more information: www.aona.org
Happy HolidaysOn behalf of our entire faculty and staff, I wish you and your family a very happy holiday season.
We wish you all the best in 2013.
~ Mark Vrahas, MD