Embed Size (px)
Citation preview
DR CHANDER PAL
DITO,DELHI
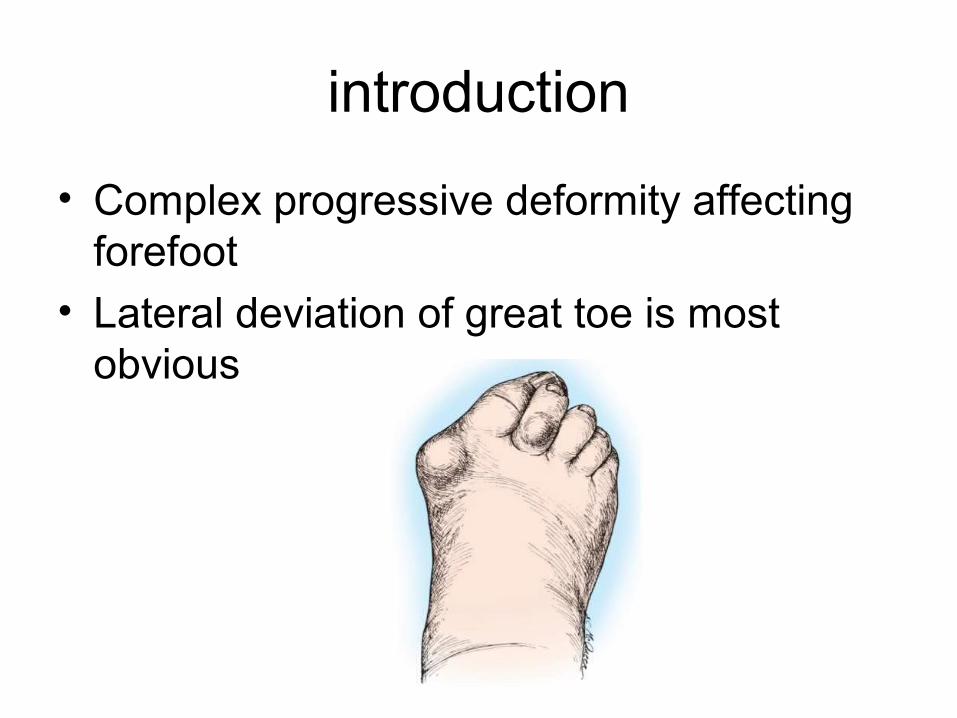
introduction
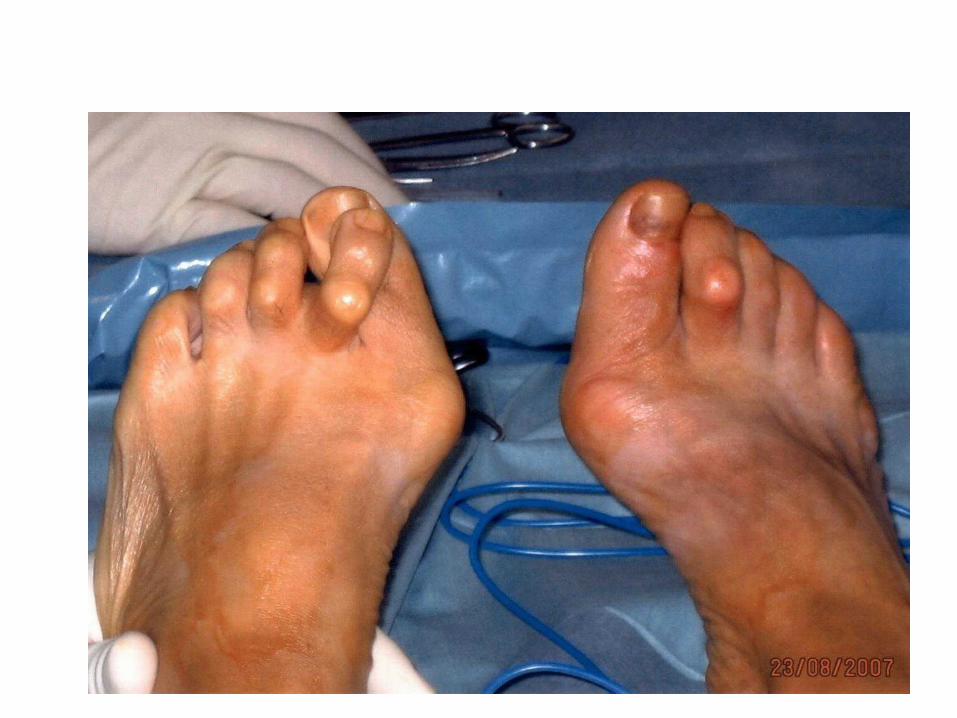
• Complex progressive deformity affecting forefoot
• Lateral deviation of great toe is most obvious
• Rotation of hallux
• Metatarsus primus varus
• Overriding of second toe over the hallux
• Overriding of lateral toes
• Hammer and claw deformities
Bunion
• Swelling that occurs because of medial eminence of metatarsal head
• Overlying bursitis
• Or may be skin callosity
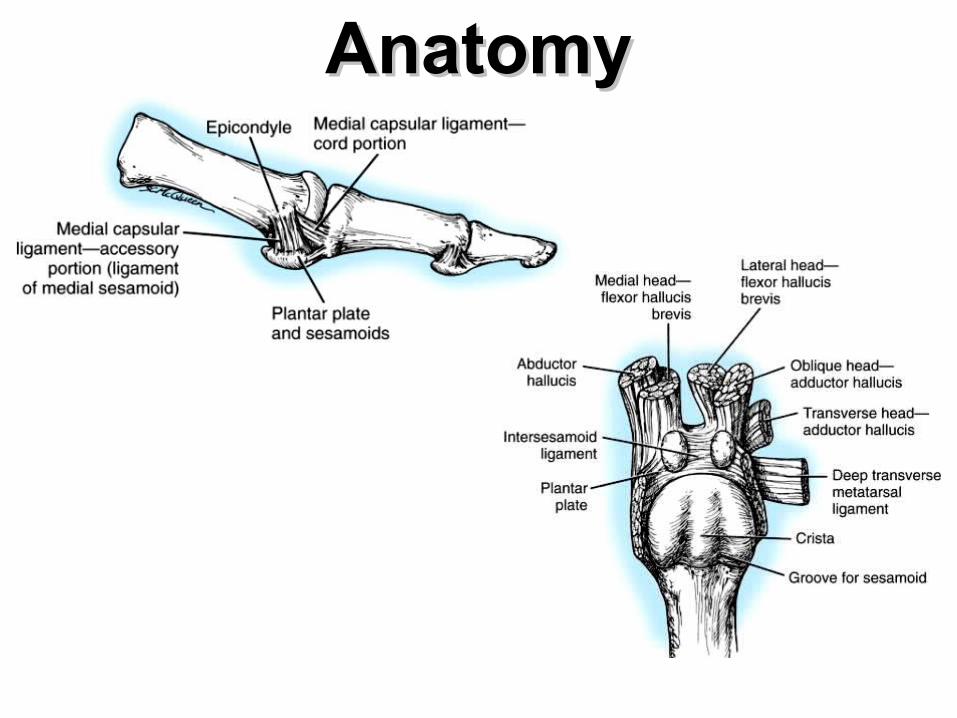
AnatomyAnatomy
PathoanatomyPathoanatomy• LATERAL DEVIATION OF GREAT TOE is primary deformity•Valgus angle of the 1st MTP joint exceeds 30 to 35 degrees•Increase in angle between first and second metatarsal (metatarsus primus varus) •Pronation of the great toe•Subluxation/dislocation of the first metatarsophalangeal joint•Excessive valgus tilt of the articular surface of
the first metatarsal head and proximal phalangeal articular surface
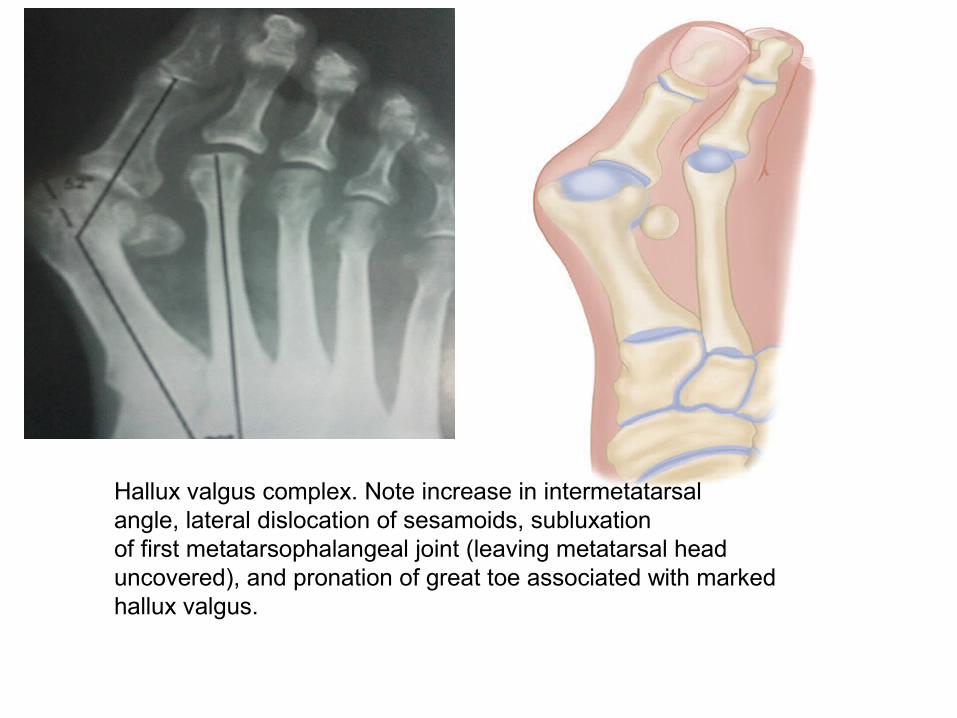
Hallux valgus complex. Note increase in intermetatarsalangle, lateral dislocation of sesamoids, subluxationof first metatarsophalangeal joint (leaving metatarsal headuncovered), and pronation of great toe associated with markedhallux valgus.
Pathogenesis • the abductor hallucis moves plantar ward• Only restraining medial structure is the medial
capsular ligament • The adductor hallucis, which is unopposed by
the abductor hallucis, pulls the great toe further into valgus
• The flexor hallucis brevis, flexor hallucis longus and extensor hallucis increases the valgus moment, further deforming the first ray.
• the metatarsal head to drift medially from the sesamoids.
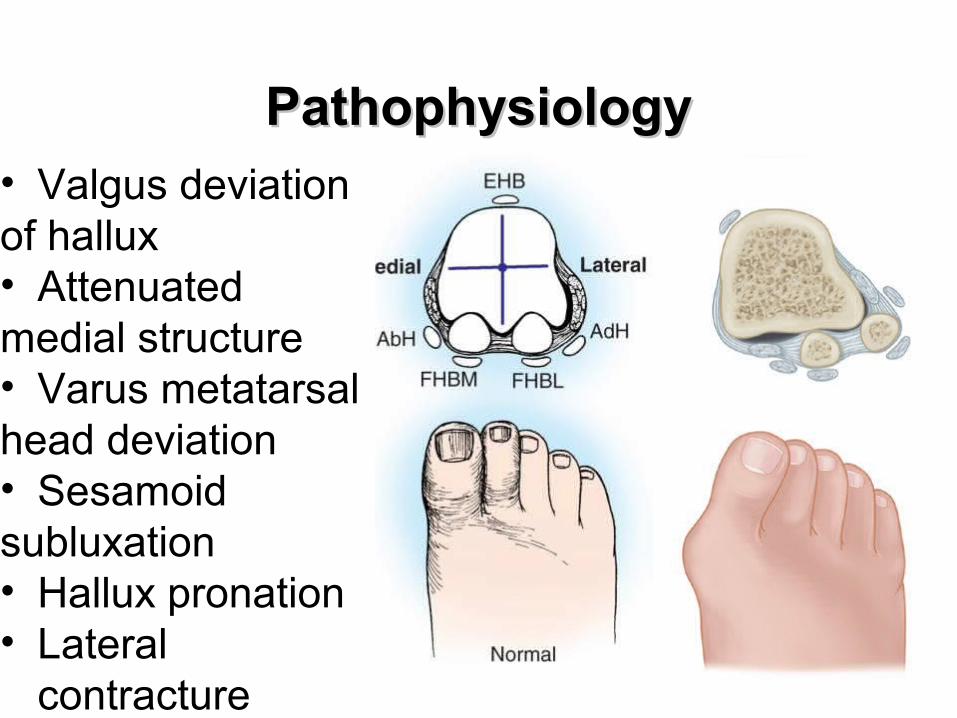
PathophysiologyPathophysiology• Valgus deviation of hallux• Attenuatedmedial structure • Varus metatarsal head deviation • Sesamoidsubluxation • Hallux pronation• Lateral
contracture
• Valgus deformity may be
• congruent or
• incongruent
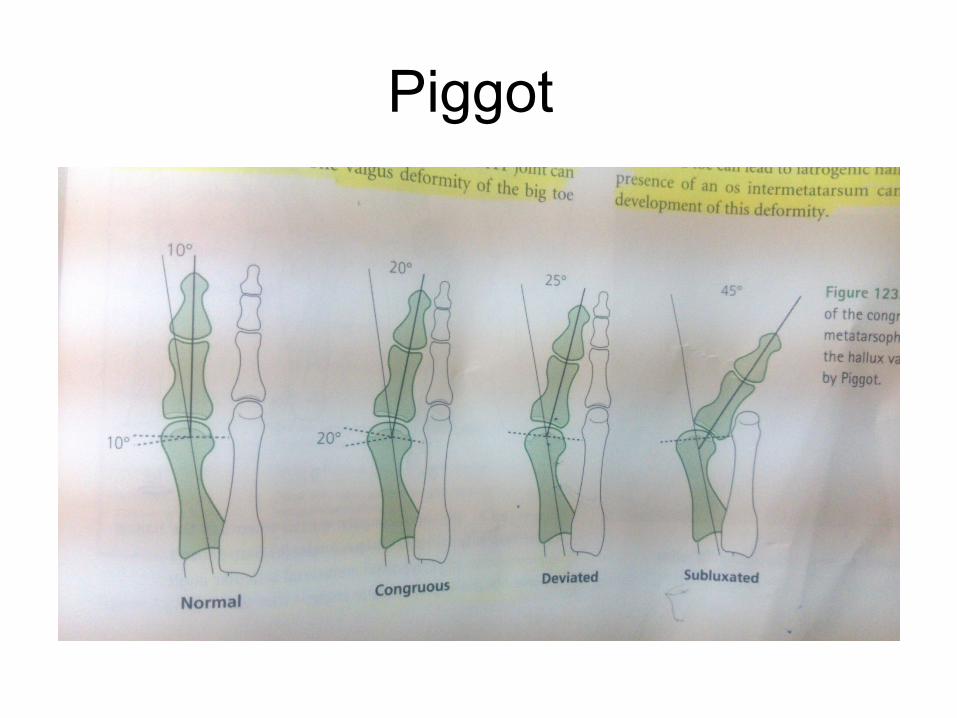
Piggot
EtiologyEtiology
•Female/male = 2:1 to 15:1• Heredity: + FH ~63% -Adolescents
•Essential extrinsic factor = shoe
EtiologyEtiology
•Intrinsic ANOTOMICAL cause• Metatarsus primus varus: juvenile form• First metatarsal length• Hypermobility of first ray• Pronated flatfeet• Ligamentous laxity
• Inflammatory arthropathies
• Spastic disorder
• Trauma
• Amputation of second toe
first variant, the articular surface of the metatarsal head is offset,
resembling a scoop of ice cream sitting at an angle on a cone This has been described as the distal
metatarsal articular angle
Second variant the articular angle of the base of the proximal phalanx
in relation to its longitudinal axis is offset. This has been described as the phalangeal articular angle
Consequences• a hammer toe–like deformity of the second
toe • the splaying of the forefoot • corns often develop• bursal hypertrophy over the medial eminence
of the first metatarsal head (bunion)• Osteoarthritis • Callosity• metatarsalgia.
The entire forefoot must be evaluated for these multiple components of hallux valgus

• Often asymptomatic
• Cosmetic deformity
• Pain
PAIN over the medial eminence (Bunion).
• Pressure from footwear is the most frequent cause of this discomfort.
• Bursal inflammation
• Irritation of the skin
• Breakdown of the skin may be noted.
Physical examination
• Vascular / neurologic status• ROM of MTP joint• Pronation of hallux• Callosities under lesser MTHs• Hammer / claw toes• MTC joint stability• Assess hind foot
Patient evaluation
X-ray
• Standard preoperative radiographs should include
1.Standing dorsoplantar views
2.Standing Lateral views
3.Nonstanding lateral oblique view
4.Axial sesamoid views
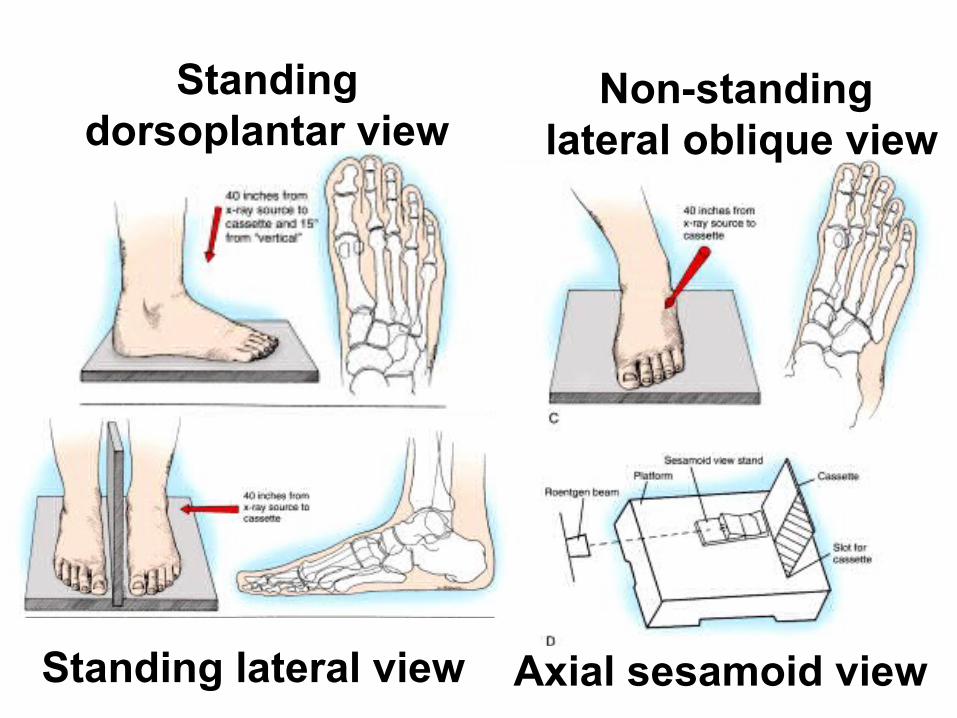
Standing dorsoplantar view
Non-standing lateral oblique view
Standing lateral view Axial sesamoid view
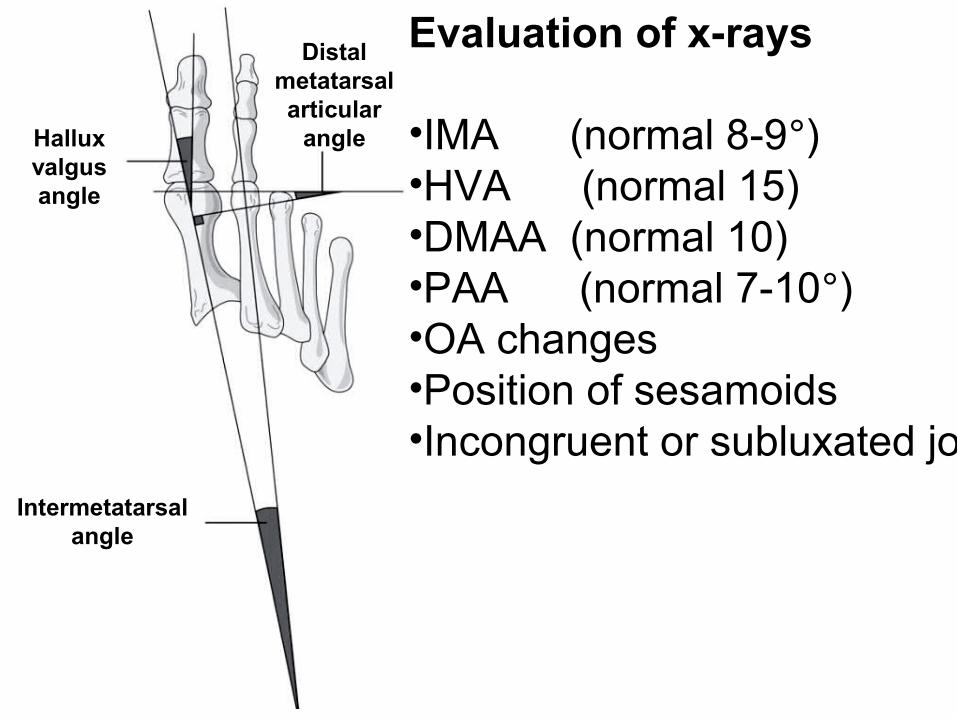
Evaluation of x-rays
•IMA (normal 8-9°) •HVA (normal 15) •DMAA (normal 10) •PAA (normal 7-10°)•OA changes•Position of sesamoids•Incongruent or subluxated joint
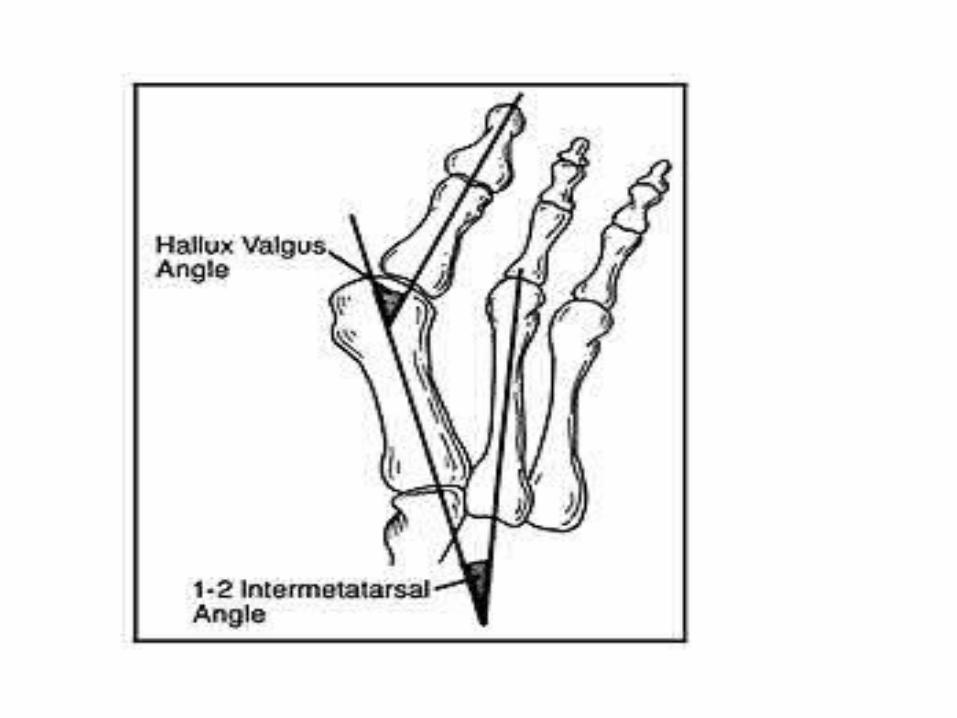
Hallux valgus angle
Intermetatarsal angle
Distal metatarsal articular
angle

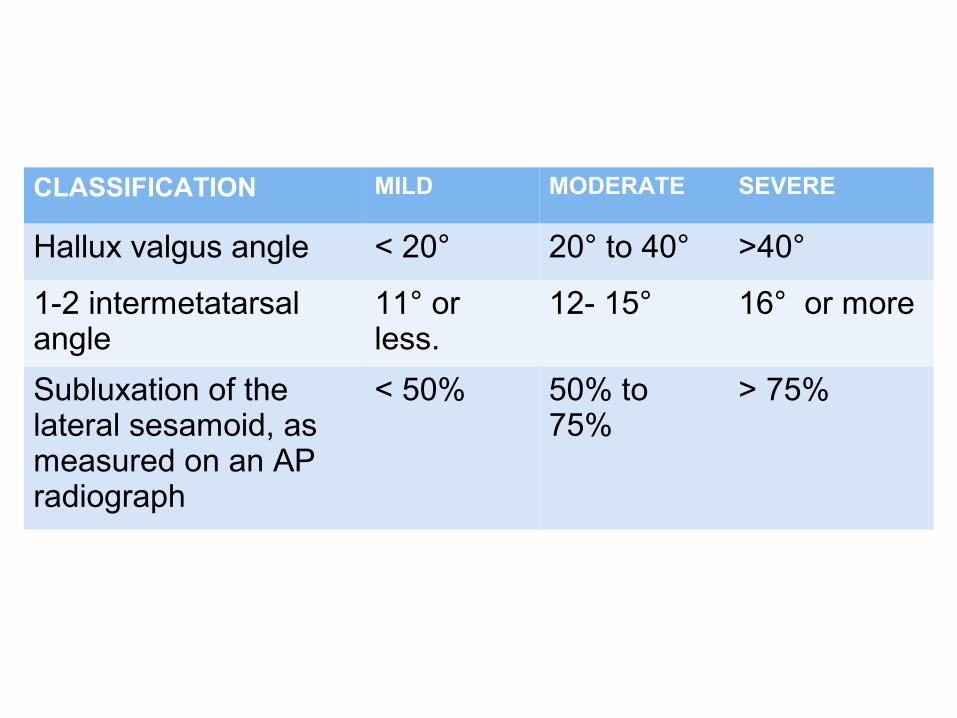
CLASSIFICATION MILD MODERATE SEVERE
Hallux valgus angle < 20° 20° to 40° >40°
1-2 intermetatarsal angle
11° or less.
12- 15° 16° or more
Subluxation of the lateral sesamoid, as measured on an AP radiograph
< 50% 50% to 75%
> 75%

Give initial trial
Shoes with wide toe box
Orthotics• medial arch support• hallux valgus splint
Achilles tendon stretchingExercisesActivity adjustments
Non-operative treatmentNon-operative treatment

•Painful joint ROM•Deformity of the joint complex•Pain or difficulty with footwear•Inhibition of activity or lifestyle
for cosmetic reasons alone is seldom indicated except in an adolescent with a significant progressive deformity. Even the mildest symptoms in an adolescent often worsen
Indications for surgeryIndications for surgery
Associated foot disorders
- Neuritis/nerve entrapment - Overlapping/underlapping 2nd digit - Hammer digits - First metatarsocuneiform joint exostosis - Sesamoiditis - Ulceration - Inflammatory conditions (bursitis, tendinitis)
of 1st metatarsal head
Indications for surgeryIndications for surgery
Extensive peripheral vascular disease Active infection Active osteoarthropathy Septic arthritis Lack of pain or deformity Advanced age Lack of compliance Co-morbidities
Contraindications
Relieve pain
Correct deformity
Preserve MTP joint motion
Surgical Goals
• most procedures to correct hallux valgus still use one or more of the components described:
• Removal of the exostosis• dissection of the bursa• tenotomy and transplantation of the tendons, • removal of the sesamoids• osteotomies
1. Valgus deviation of the great toe
2. Varus deviation of the 1st metatarsal
3. Pronation of hallux and/or 1st
metatarsal
4. Hallux valgus interphalangeus
5. Arthritis and limitation of motion of the
1st metatarsophalangeal joint
6. Length of the 1st metatarsal relative to
lesser metatarsals
Preoperative evaluation
7. Excessive mobility or obliquity of the 1st
metatarsomedial cuneiform joint
8. The medial eminence (bunion)
9. The location of the sesamoid apparatus
10. Intrinsic and extrinsic muscle-tendon
balance and synchrony
Preoperative evaluationPreoperative evaluation
Indications• Stress view radiographs - a firm forefoot wrap
reduces the intermetatarsal angle to a normal value and decreases the hallux valgus angle
• Middle aged• Mild to moderate• a valgus angle at the metatarsophalangeal joint
of 15 to 25 degrees• an intermetatarsal angle of less than 13
degrees, • valgus of the interphalangeal joint of less than
15 degrees• no degenerative changes at the
metatarsophalangeal joint• a history of conservative management failure
Distal Soft tissue handling includes
• Medial eminence removal • Adductor tendon and lateral capsular release• Medial capsular imbrication• Reduction of MTP joint and sesamoids
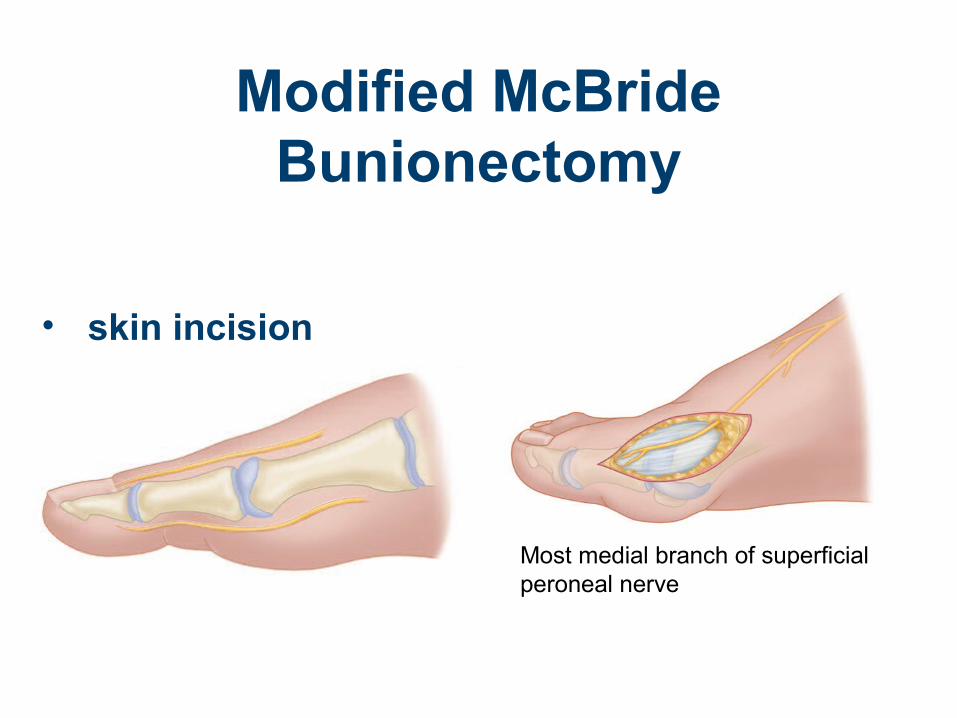
Modified McBride Bunionectomy
• skin incision
Most medial branch of superficial peroneal nerve
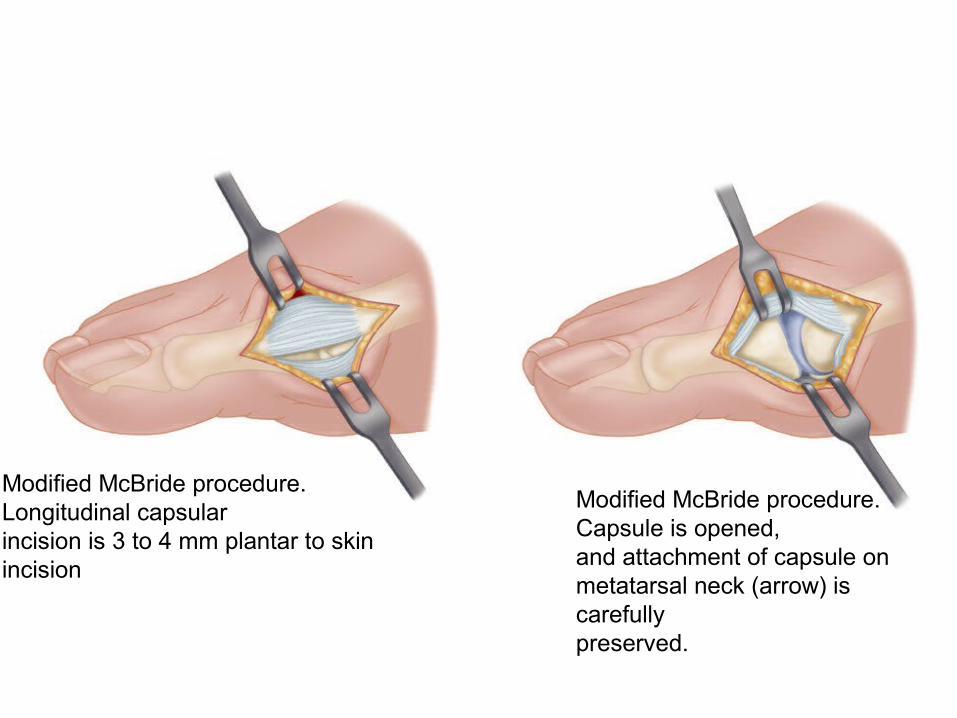
Modified McBride procedure. Longitudinal capsularincision is 3 to 4 mm plantar to skin incision
Modified McBride procedure. Capsule is opened,and attachment of capsule on metatarsal neck (arrow) is carefullypreserved.
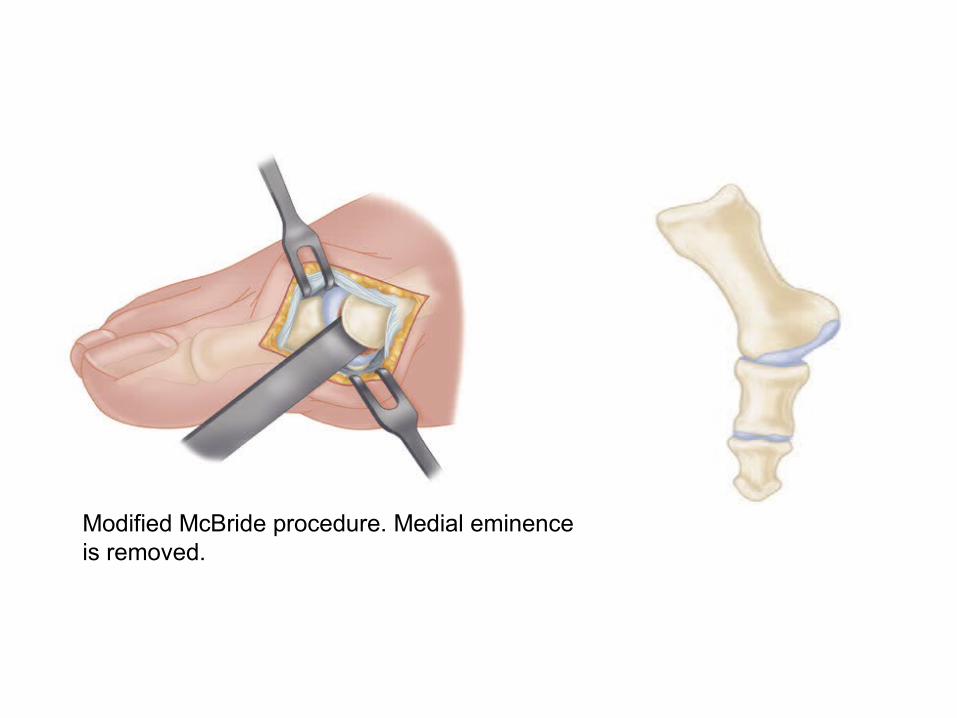
Modified McBride procedure. Medial eminenceis removed.
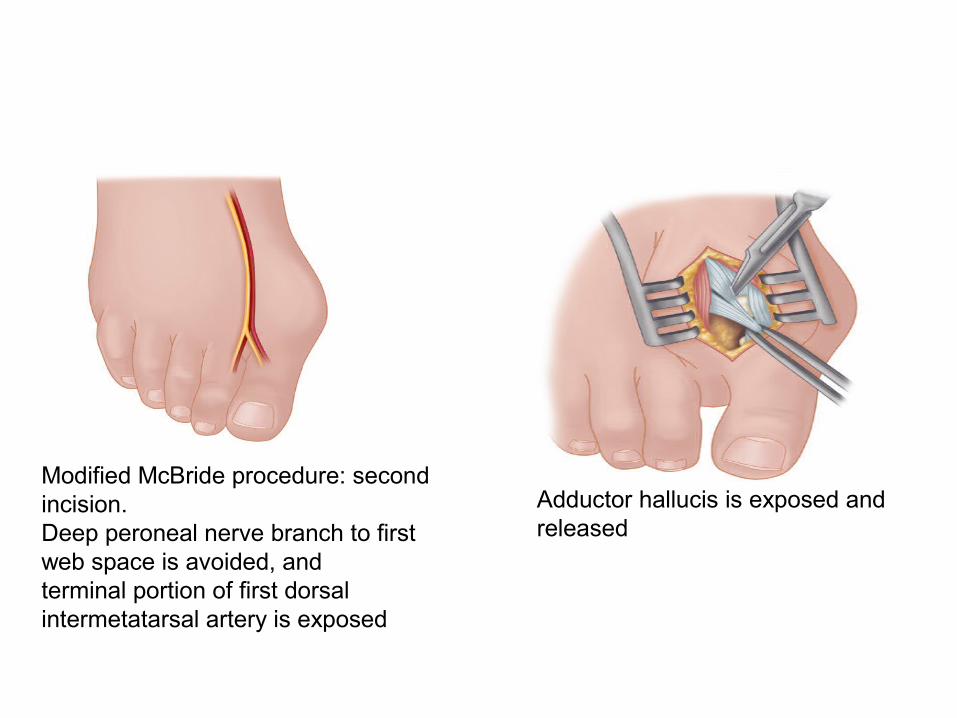
Modified McBride procedure: second incision.Deep peroneal nerve branch to first web space is avoided, andterminal portion of first dorsal intermetatarsal artery is exposed
Adductor hallucis is exposed andreleased
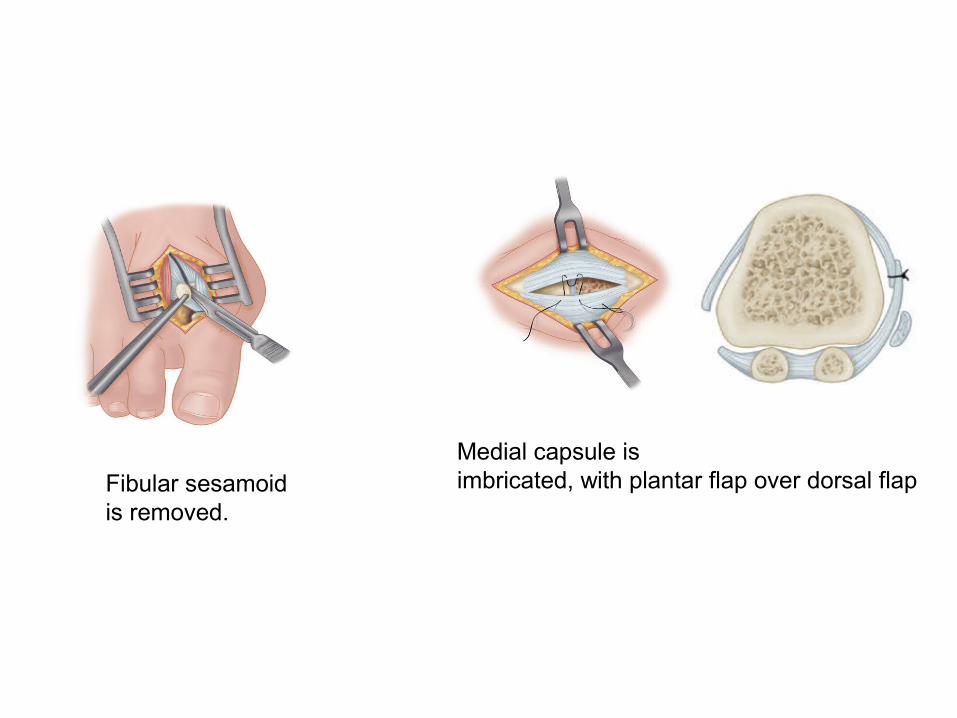
Fibular sesamoidis removed.
Medial capsule isimbricated, with plantar flap over dorsal flap

Toe spacer is worn for 6 weeks after surgery tomaintain medial capsular stabilization
Hallux valgus night splint to be worn for 6 to 8weeks after dressing changes are completed.
Complications
• Recurrence
• Hallux varus
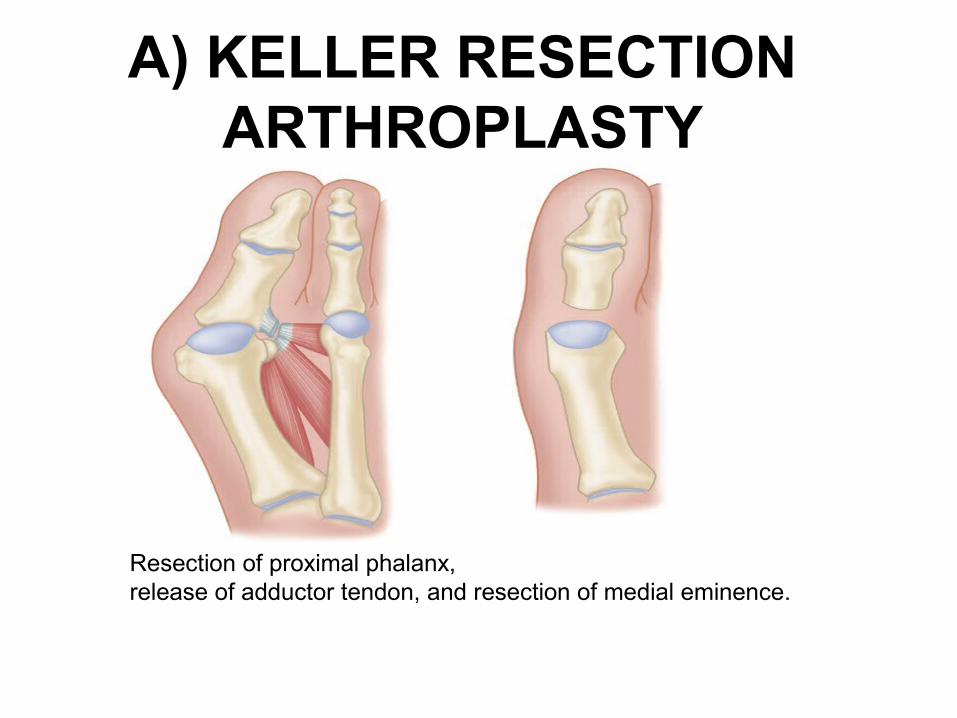
A) KELLER RESECTION ARTHROPLASTY
Resection of proximal phalanx,release of adductor tendon, and resection of medial eminence.
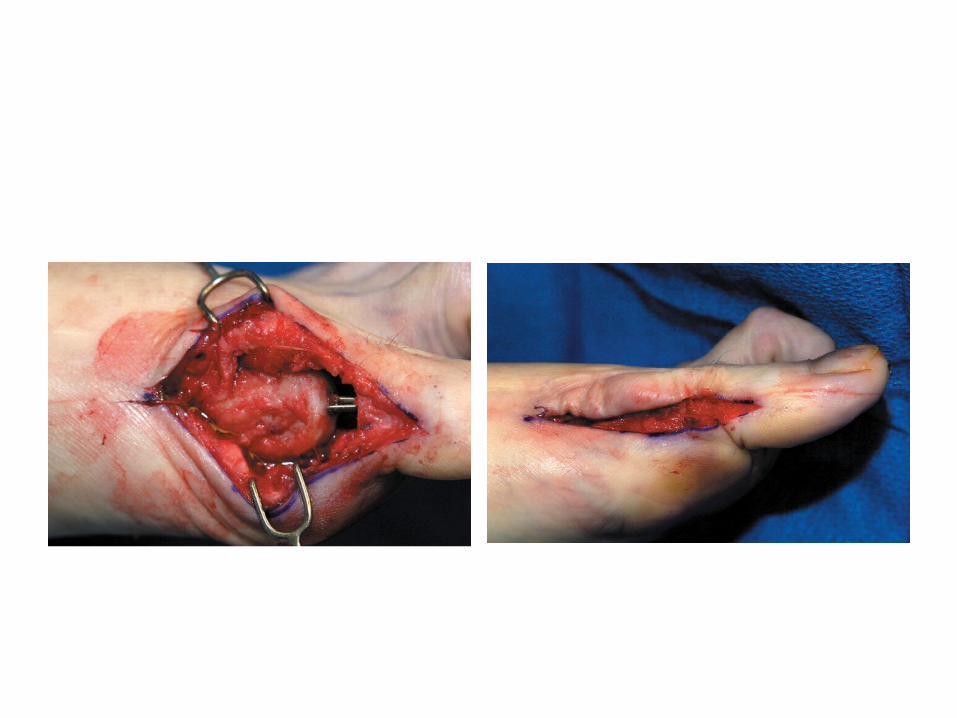
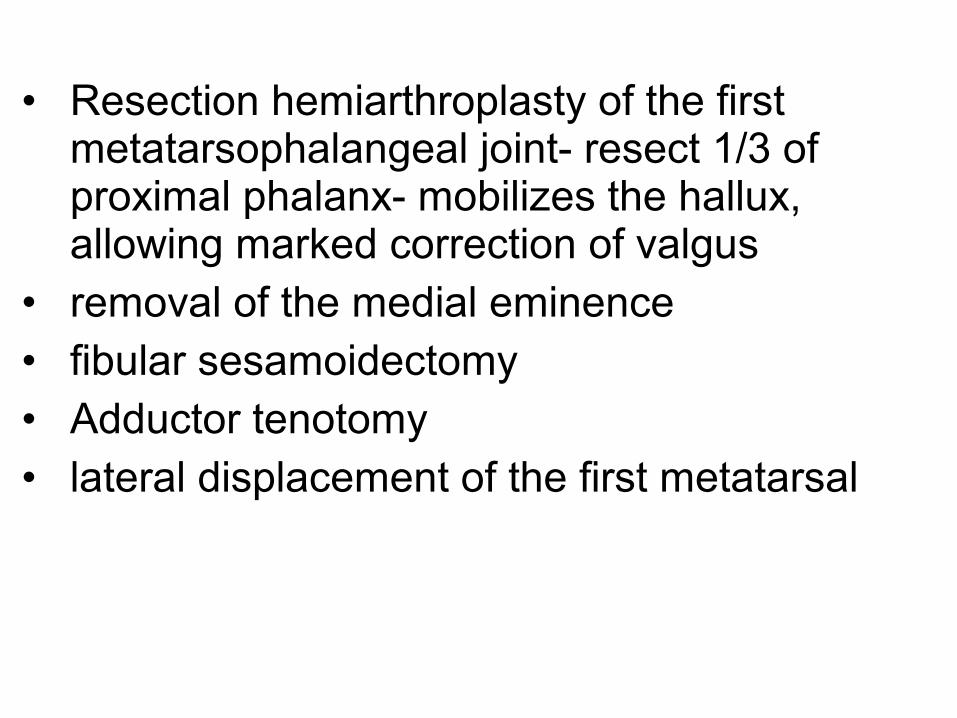
• Resection hemiarthroplasty of the first metatarsophalangeal joint- resect 1/3 of proximal phalanx- mobilizes the hallux, allowing marked correction of valgus
• removal of the medial eminence • fibular sesamoidectomy• Adductor tenotomy• lateral displacement of the first metatarsal
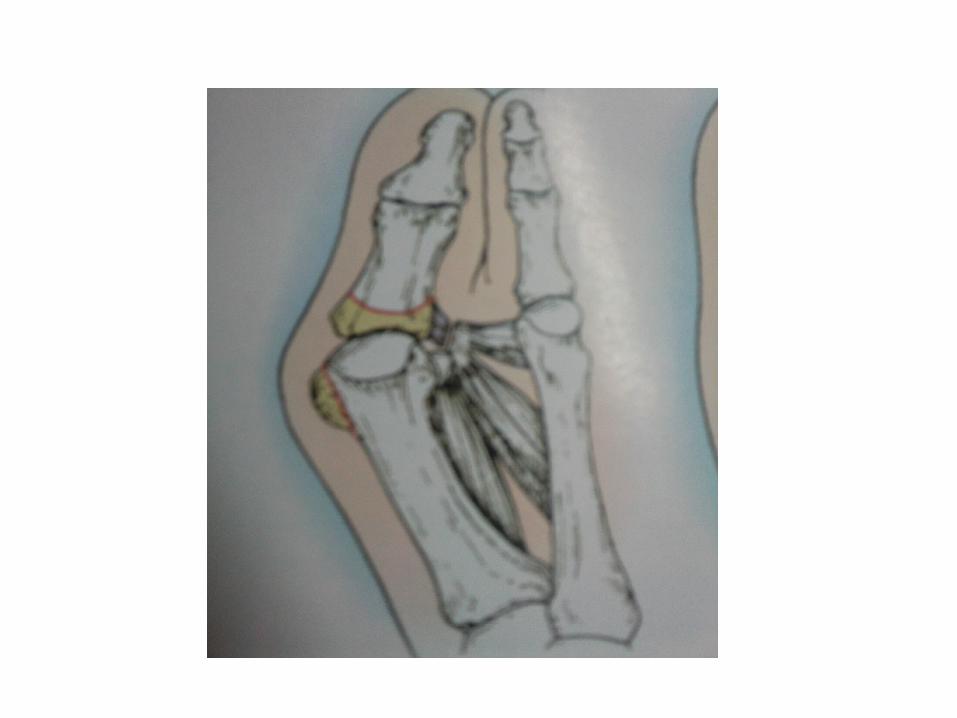
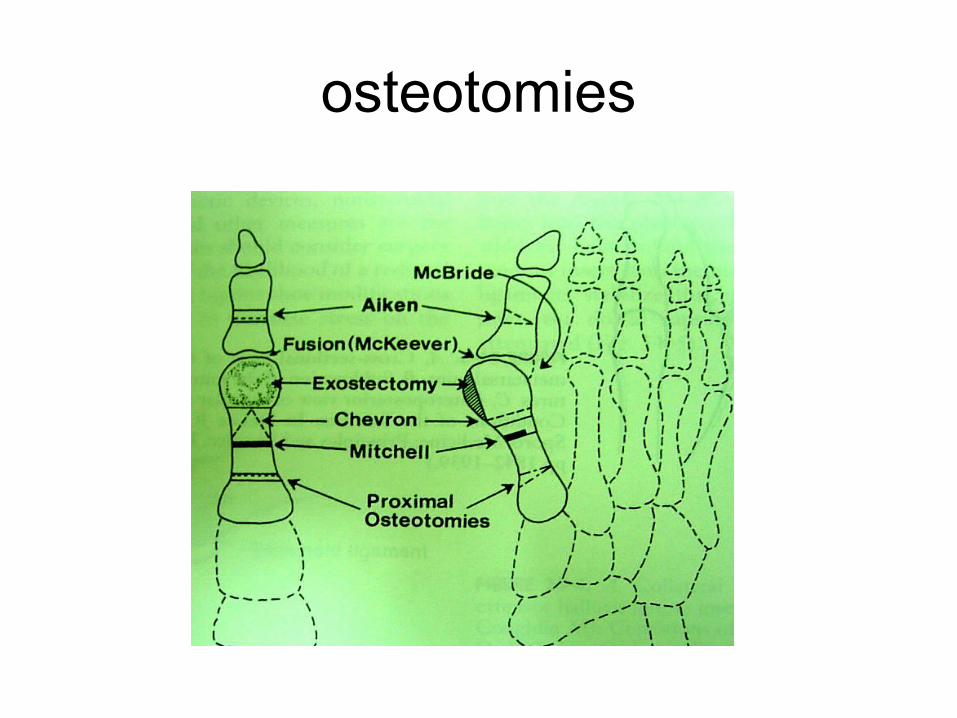
osteotomies
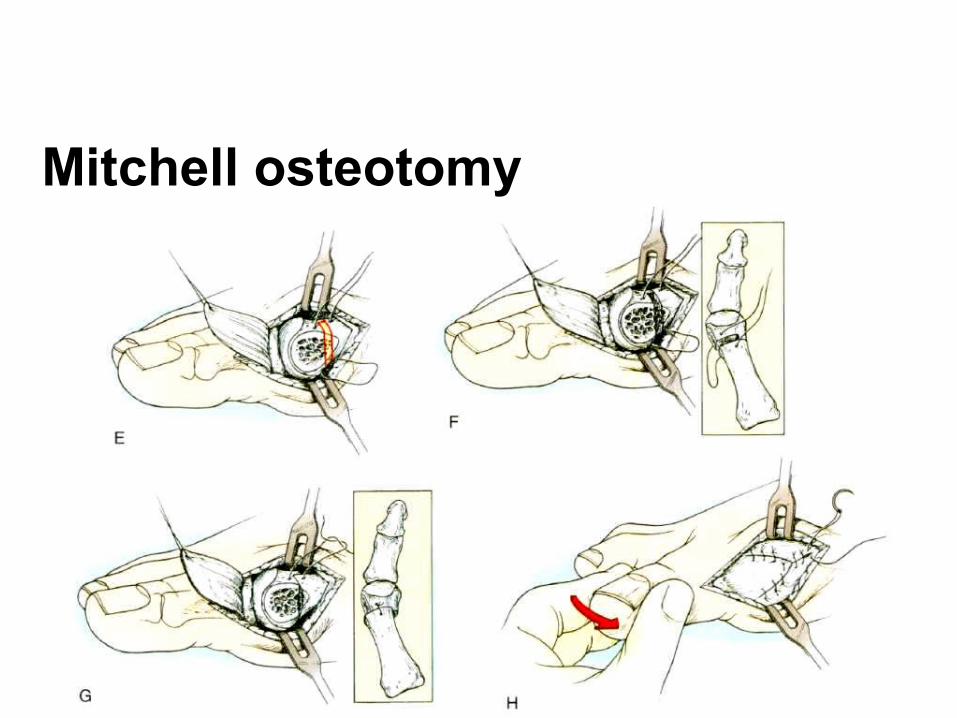
Mitchell osteotomy
• Extracapsuler
• Mild to moderate deformity
• HVA of up to 40 degree
• Excision of medial eminence
• Step cut osteotomy at metaphyseal diphyseal junction
• Medial capsulorrhaphy
Mitchell osteotomy
CHEVRON INTRACAPSULAR OSTEOTOMY
Indications• younger patients (adolescence through the 30s) • hallux valgus angle of 30 degrees or less
• an intermetatarsal angle of less than 13 degrees.
ADVANTAGES• made through cancellous bone• shortens the metatarsal less
• inherently stable
• Fixation of the osteotomy with one or two Kirschner wires, a cortical screw, or a biodegradable pin adds stability to the osteotomy
Consists of
(1) medial eminence removal
(2) a V-shaped intracapsular through the
first metatarsal head in trasverse plane
(3) lateral displacement of the capital
fragment
(4) removal of the resulting projection of the
first metatarsal
(5) medial capsulorrhaphy
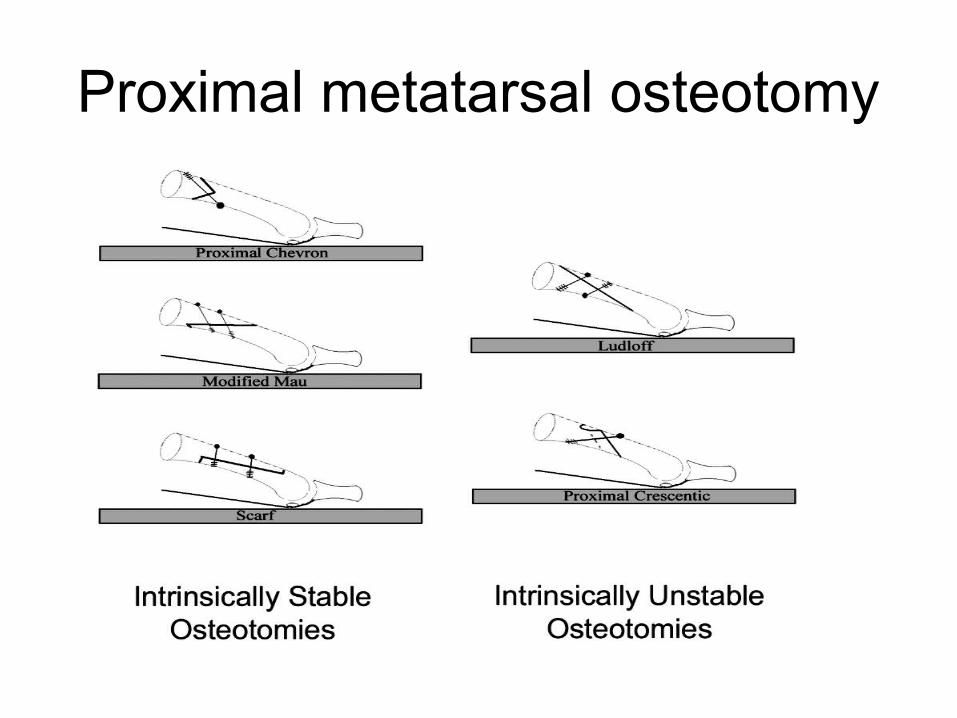
Proximal metatarsal osteotomy
Scarf osteotomy
• HVA > 25,IMA>13
• Z step cut osteotomy of MT shaft
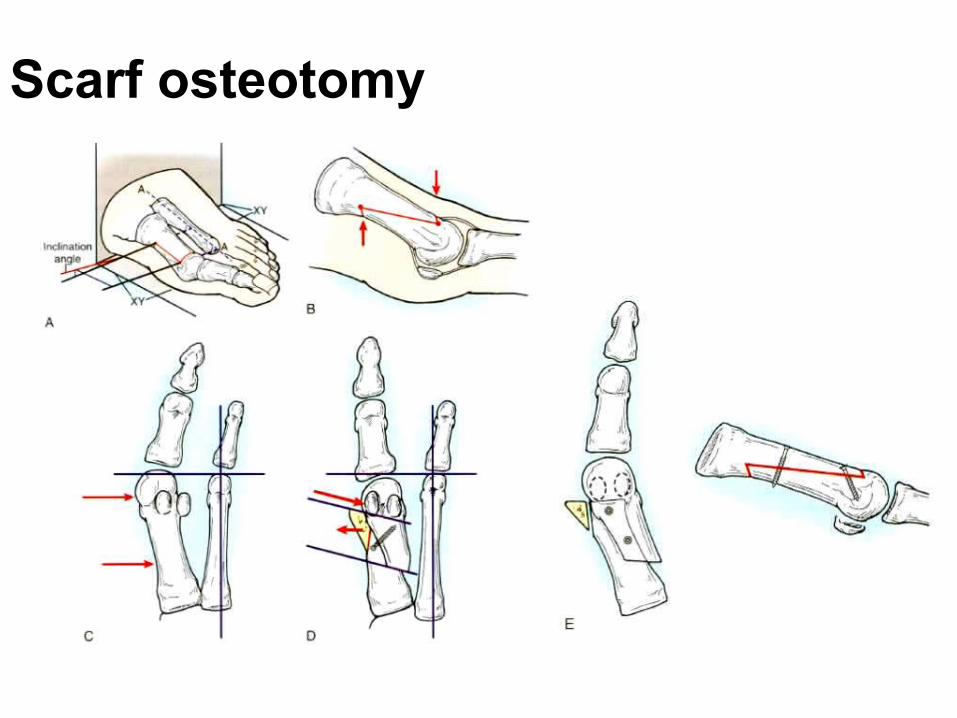
Scarf osteotomy
Ludloff osteotomy
• Oblique osteotomy of 1st metatarsal
• Dorsal proximal to distal planter
D) MEDIAL CUNEIFORM OSTEOTOMY
Indications
in adolescents with open proximal
metatarsal physes
especially patients with an abnormally
wide intermetatarsal angle
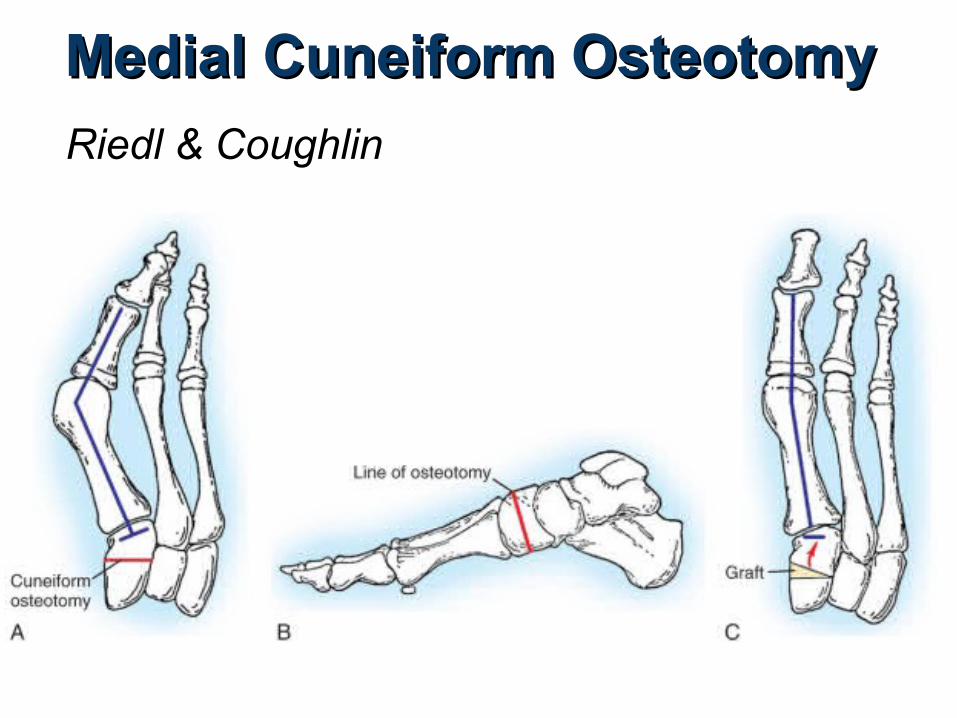
Medial Cuneiform OsteotomyMedial Cuneiform Osteotomy
Riedl & Coughlin
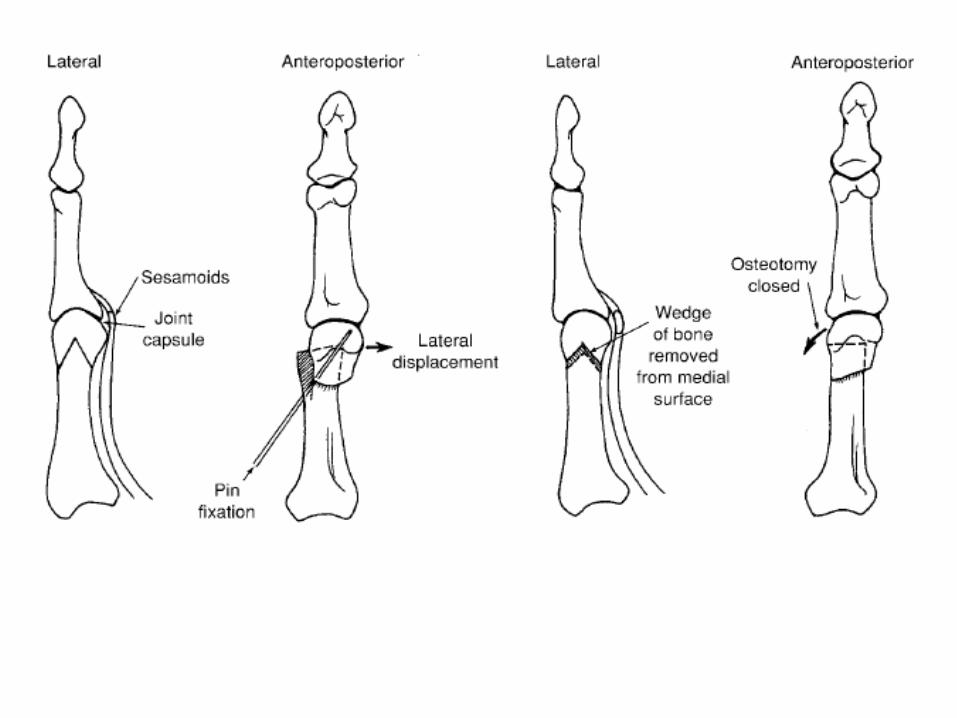
E) PROXIMAL PHALANGEAL OSTEOTOMY (AKIN’S)
• a medially based closing wedge osteotomy at the base of the
proximal phalanx, combined with medial eminence removal
• mostly as an adjunctive procedure to the primary bunion repair
• alone rarely is indicated
• limited value if the sesamoid apparatus is subluxed
• does not correct the principal deforming forces of the adductor
hallucis and the varus of the first metatarsal, so, is indicated
primarily in combination with other procedures , but after which
slight residual valgus deformity remains
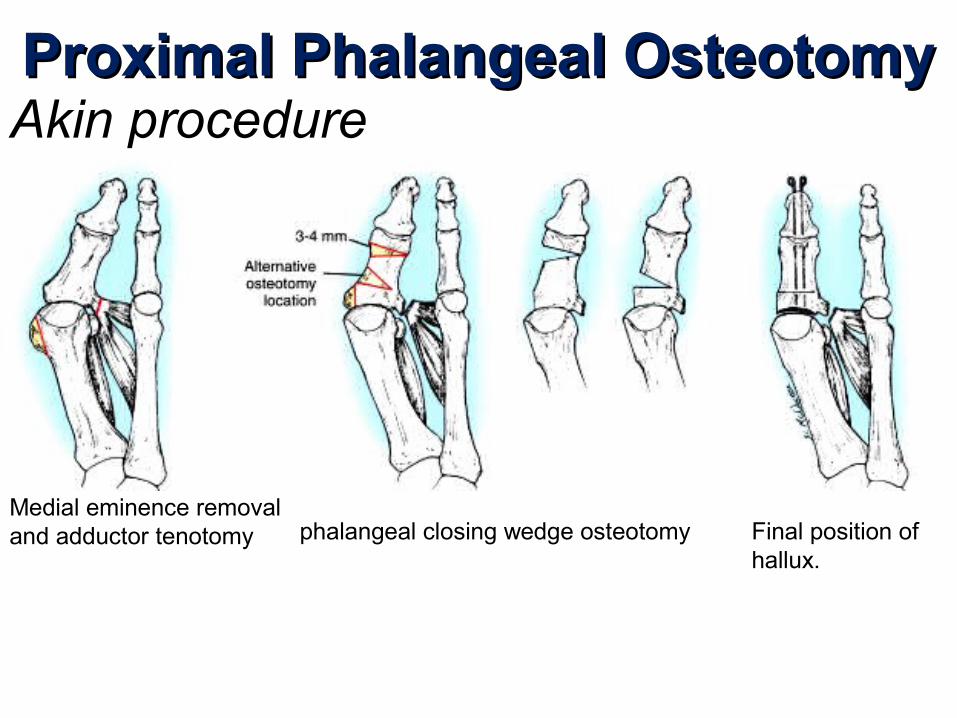
Proximal Phalangeal OsteotomyProximal Phalangeal OsteotomyAkin procedure
Medial eminence removal and adductor tenotomy phalangeal closing wedge osteotomy Final position of
hallux.
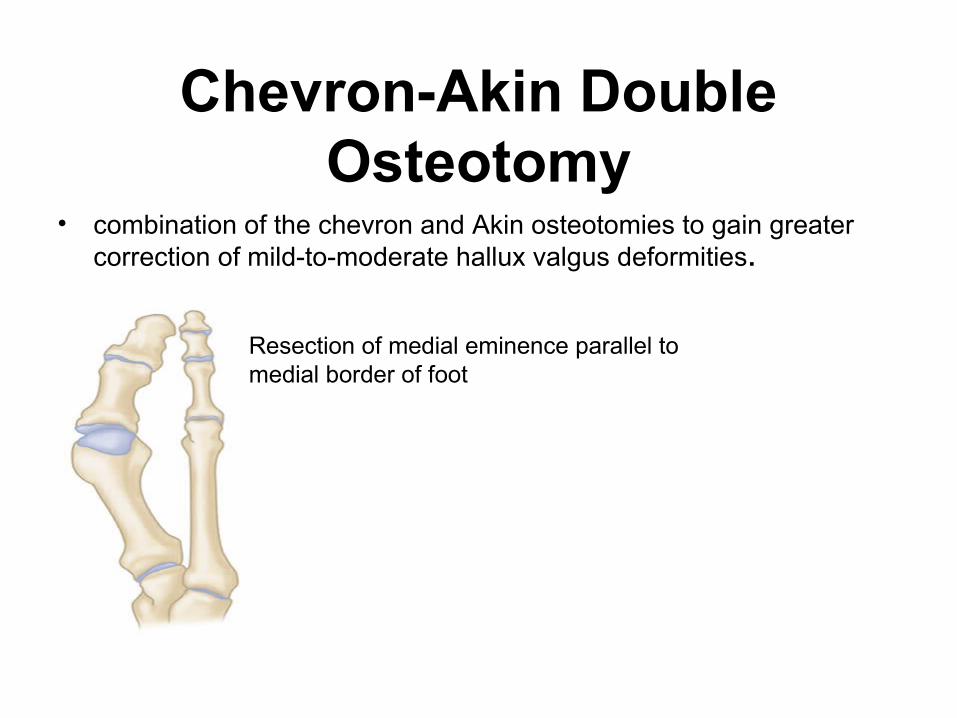
Chevron-Akin Double Osteotomy
• combination of the chevron and Akin osteotomies to gain greater correction of mild-to-moderate hallux valgus deformities.
Resection of medial eminence parallel to medial border of foot
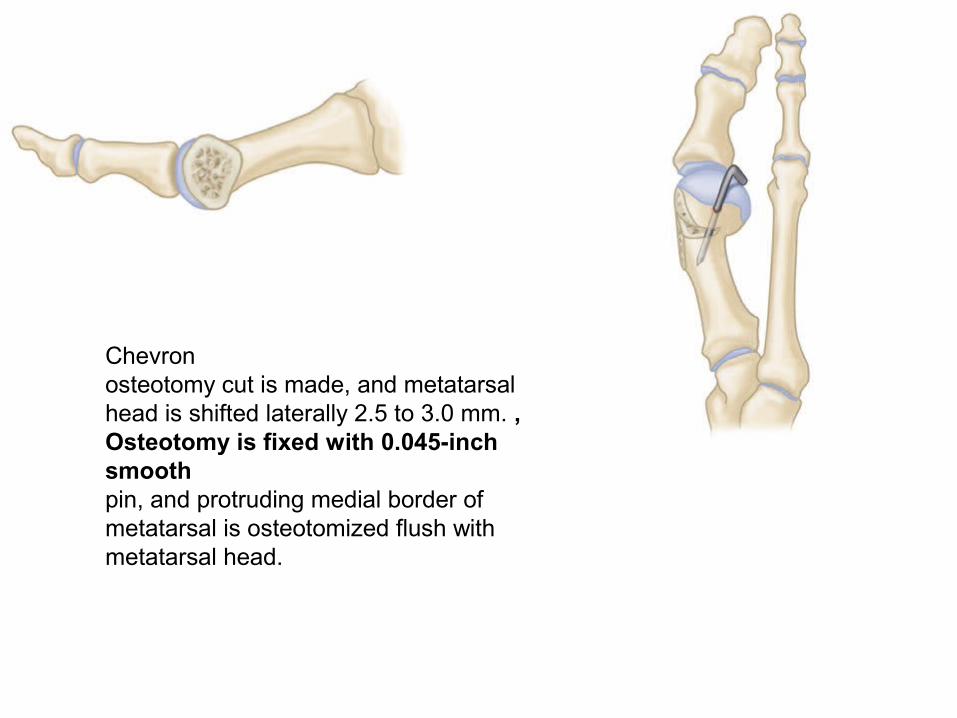
Chevronosteotomy cut is made, and metatarsal head is shifted laterally 2.5 to 3.0 mm. , Osteotomy is fixed with 0.045-inch smoothpin, and protruding medial border of metatarsal is osteotomized flush with metatarsal head.
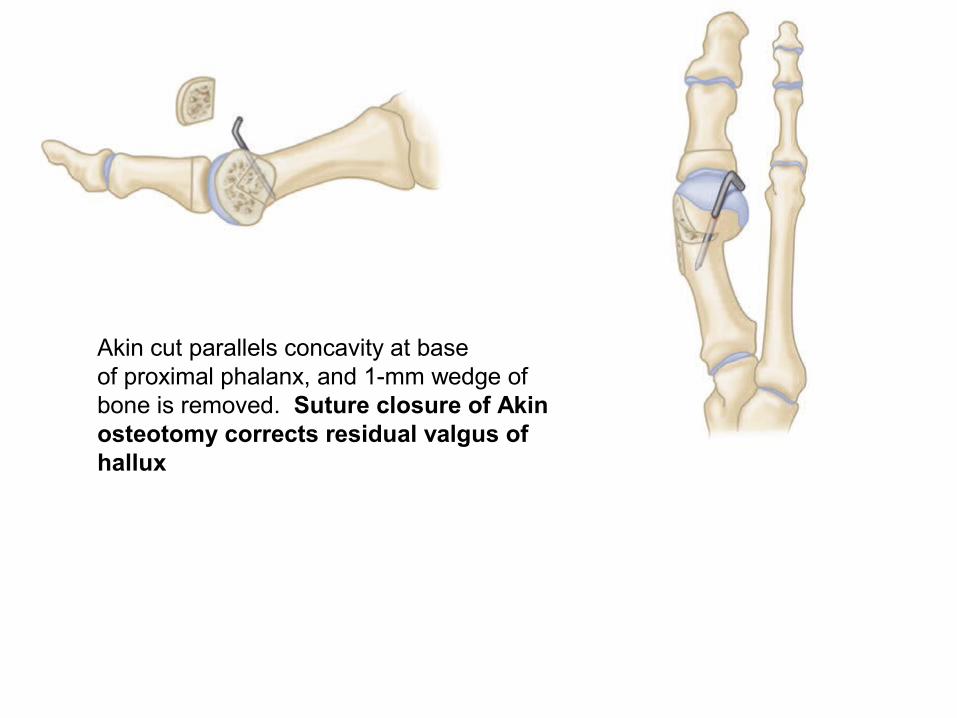
Akin cut parallels concavity at baseof proximal phalanx, and 1-mm wedge of bone is removed. Suture closure of Akin osteotomy corrects residual valgus of hallux
ARTHRODESIS OF THE FIRST METATARSOPHALANGEAL JOINT
Various fixation methods have been described.
one-quarter tubular plate with one oblique
interfragmentary screw
one-third tubular plate
two ⅛-inch Steinmann pins placed
through the hallux into the first metatarsal
Indication 1. Severe deformity (an intermetatarsal angle >20 to 22
degrees, a hallux valgus angle >45 degrees, and severe pronation of the hallux)
2. with Degenerative arthritis / rheumatoid arthritis
3. motion of the metatarsophalangeal joint is limited and painful
4. Recurrent hallux valgus
5. Hallux valgus caused by muscle imbalance in patients with neuromuscular disorders, such as cerebral palsy, to prevent recurrence
6. Posttraumatic hallux valgus with severe disruption of all medial capsular structures that cannot be adequately reconstructed.
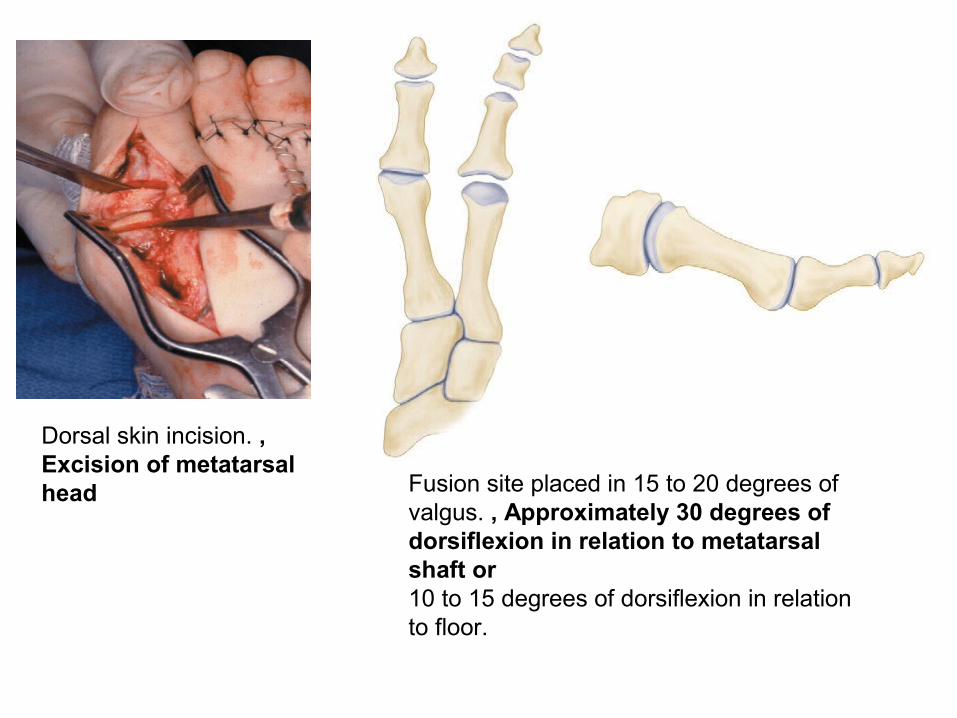
Dorsal skin incision. , Excision of metatarsal head Fusion site placed in 15 to 20 degrees of
valgus. , Approximately 30 degrees of dorsiflexion in relation to metatarsal shaft or10 to 15 degrees of dorsiflexion in relation to floor.
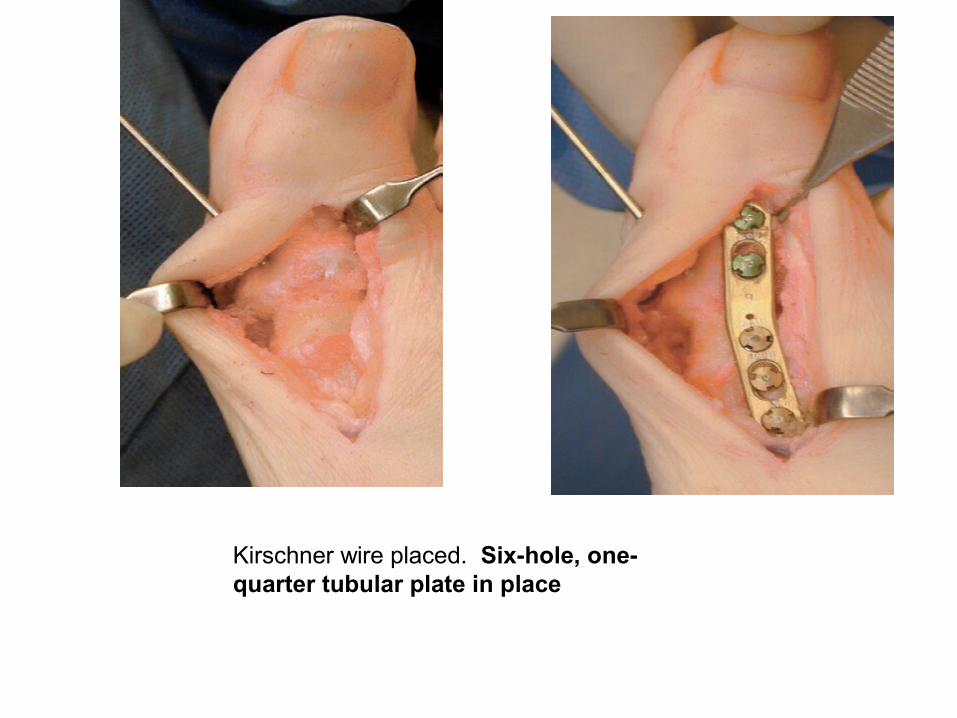
Kirschner wire placed. Six-hole, one-quarter tubular plate in place
• an increased distal metatarsal articular angle may be the defining characteristic of juvenile hallux valgus
. Pain, either at the metatarsophalangeal joint or beneath the
lesser metatarsal heads, may not be the primary complaint in
many instances
Varus of the first metatarsal with a widened intermetatarsal
angle is almost always present
• Hypermobile flatfoot with pronation of the foot during weight
bearing frequently is associated with the deformity
• Recurrence of the deformity is more frequent
• The family history frequently
• Soft-tissue procedures alone are unlikely to result in
permanent correction.
Indicaion for surgery
• Any adolescent 12 to 18 years old
• with cosmetically unattractive hallux valgus deformity
• report to be progressive
• family history is positive for hallux valgus
• Pain and shoe-fitting problems
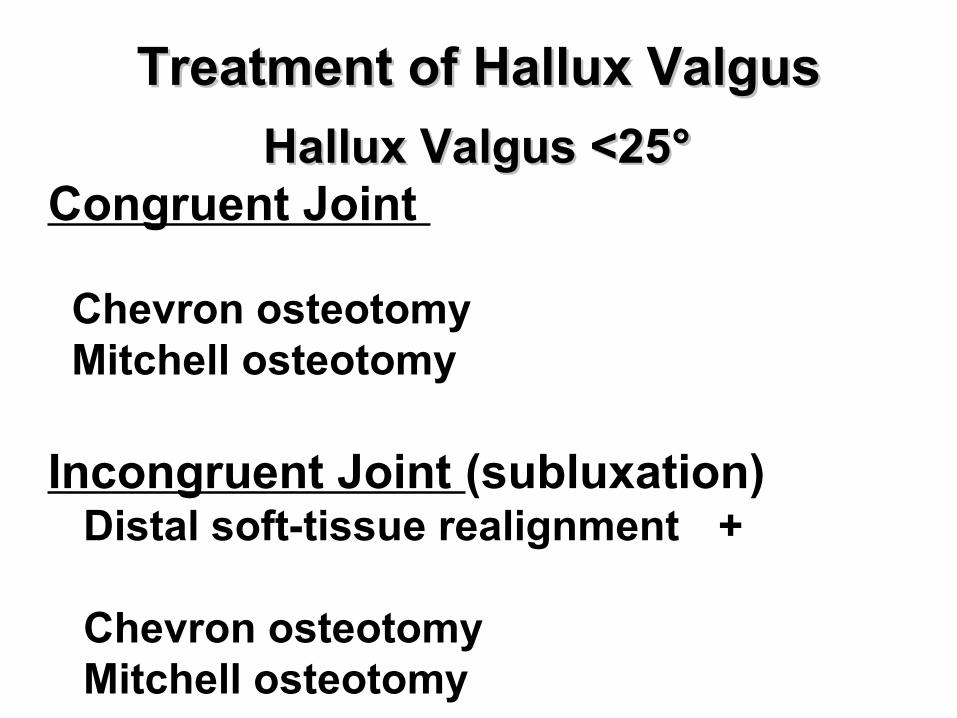
Hallux Valgus <25Hallux Valgus <25°°Congruent Joint
Chevron osteotomy Mitchell osteotomy
Incongruent Joint (subluxation) Distal soft-tissue realignment +
Chevron osteotomy Mitchell osteotomy
Treatment of Hallux ValgusTreatment of Hallux Valgus
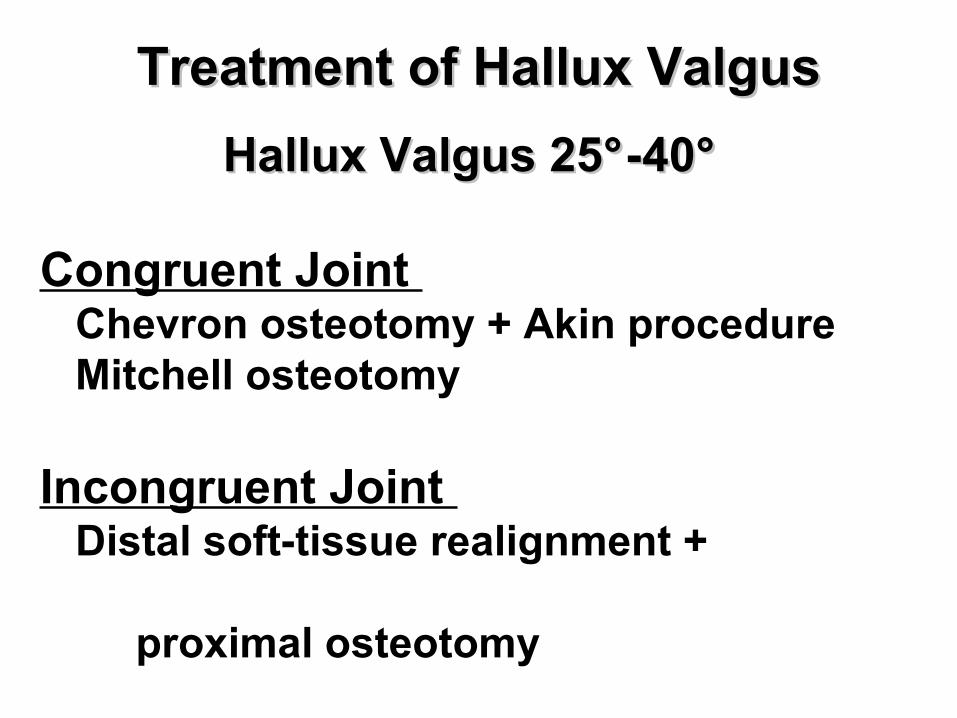
Hallux Valgus 25Hallux Valgus 25°° -40-40°°
Congruent Joint Chevron osteotomy + Akin procedure Mitchell osteotomy
Incongruent Joint Distal soft-tissue realignment +
proximal osteotomy
Treatment of Hallux ValgusTreatment of Hallux Valgus
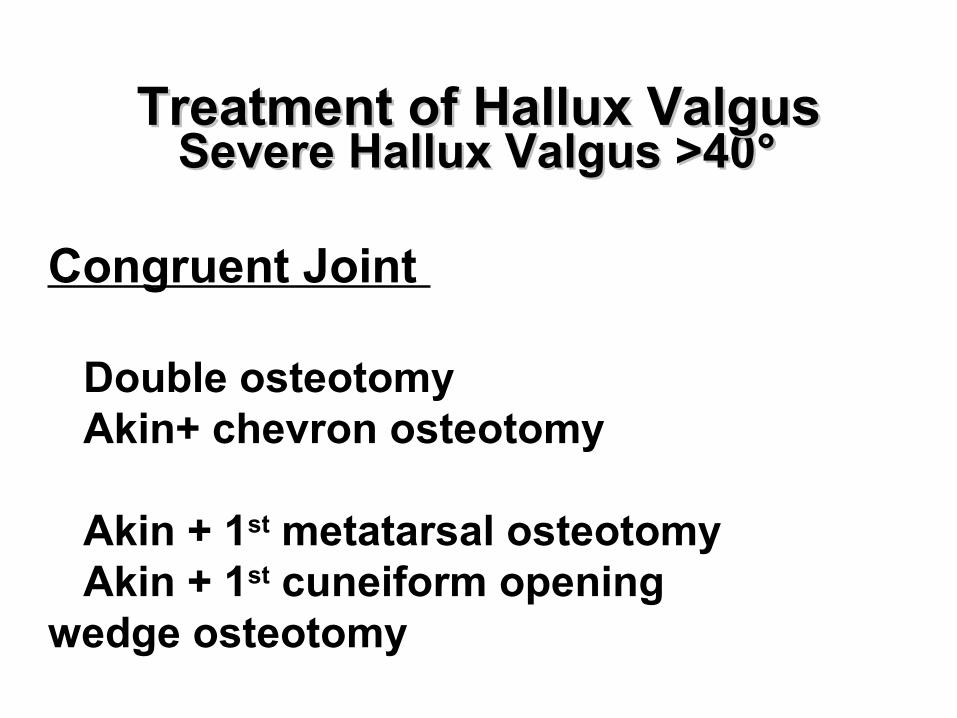
Severe Hallux Valgus >40Severe Hallux Valgus >40°°
Congruent Joint
Double osteotomy Akin+ chevron osteotomy
Akin + 1st metatarsal osteotomy Akin + 1st cuneiform opening wedge osteotomy
Treatment of Hallux ValgusTreatment of Hallux Valgus
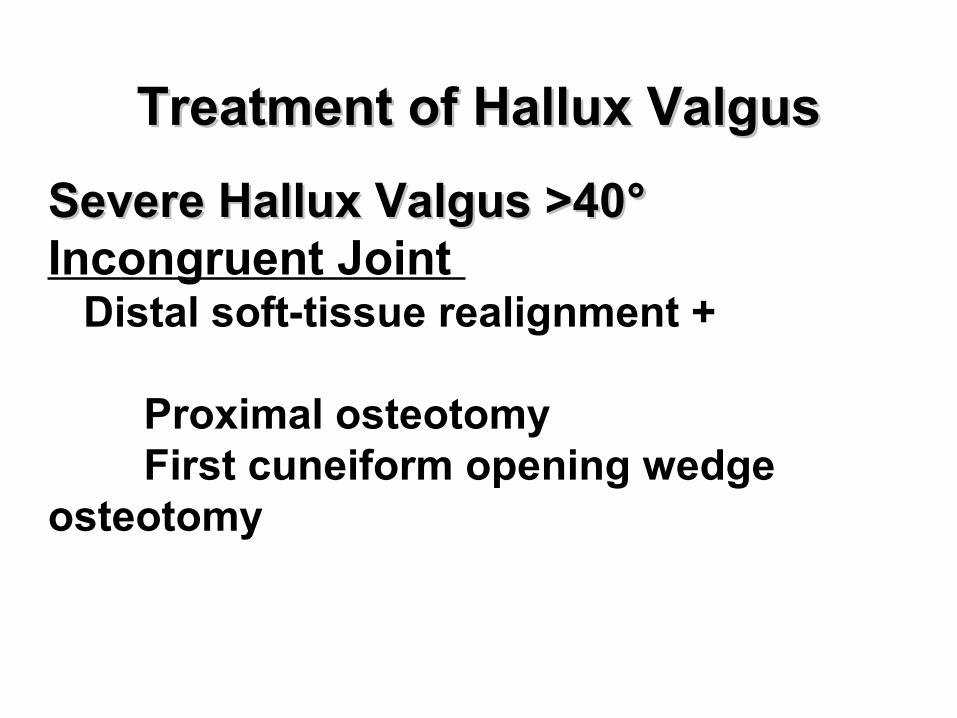
Severe Hallux Valgus >40Severe Hallux Valgus >40°°Incongruent Joint Distal soft-tissue realignment +
Proximal osteotomy First cuneiform opening wedge osteotomy
Treatment of Hallux ValgusTreatment of Hallux Valgus
Hypermobile 1Hypermobile 1stst MTC Joint MTC Joint
Distal soft-tissue realignment + fusion 1st metatarsocuneiform joint
Degenerative joint diseaseDegenerative joint disease
Fusion or Keller procedure or prosthesis
Treatment of Hallux ValgusTreatment of Hallux Valgus
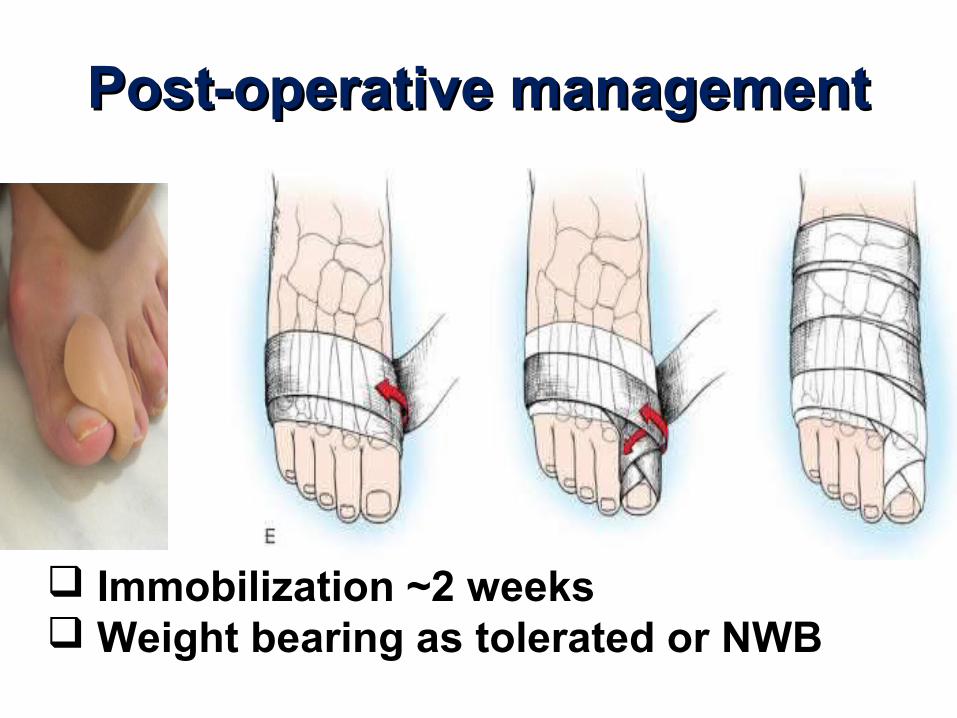
Post-operative managementPost-operative management
Immobilization ~2 weeks Weight bearing as tolerated or NWB
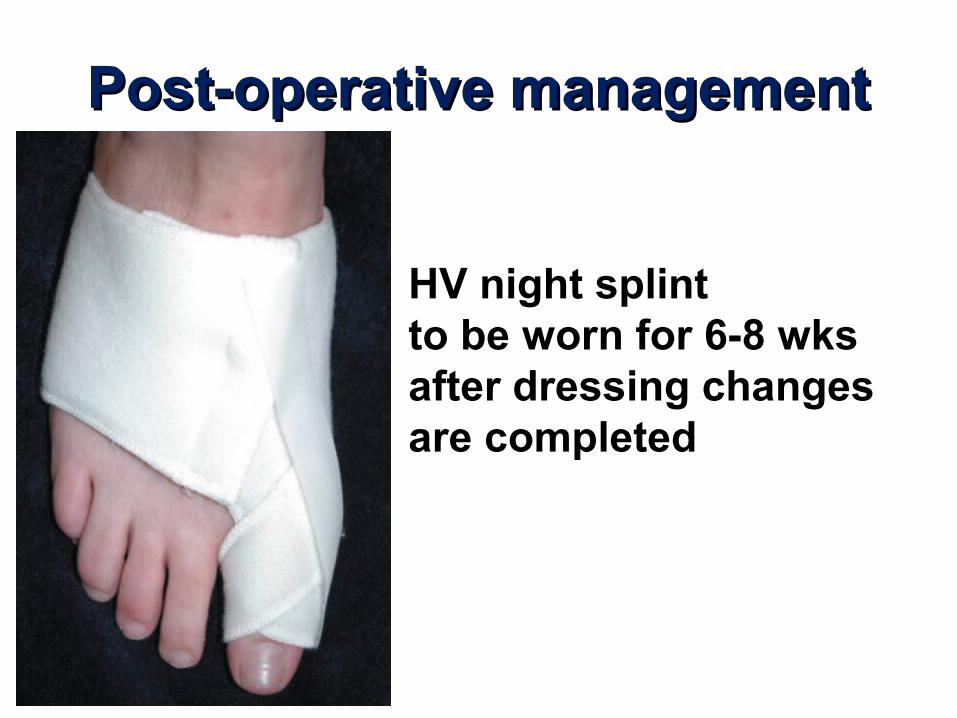
Post-operative managementPost-operative management
HV night splint to be worn for 6-8 wks after dressing changes are completed
Complications of surgery•nonunion
•recurrence of the deformity
•The most troublesome has been metatarsalgia,
attributable to dorsiflexion malunion of the distal
fragment (use of a Kirschner wire for fixation (instead of
sutures) prevented malunion)
•excessive shortening of the metatarsal,
• medial eminence pain
• clawed hallux
• transfer keratotic lesions
• development of the opposite deformity, hallux
varus
PAINFUL HEEL