Embed Size (px)
Citation preview

1Learn…ignorance will disappear of itself…!
….. foundation of clinical medicine
Shashidhar Venkatesh MurthyA/Prof & Head of Pathology
College of Medicine & Dentistry
Clinical Pathology:
RBC 1.4: Congenital Hemolytic Anemia
CPC : Term2 Week1 - Haem 1/2.
System : Haematology - RBC Disorders.
Topic : 1: Anemia Intro 2: IDA, MBA & ACD 3: Acquired HA 4: Congenital HA. 5: Others.
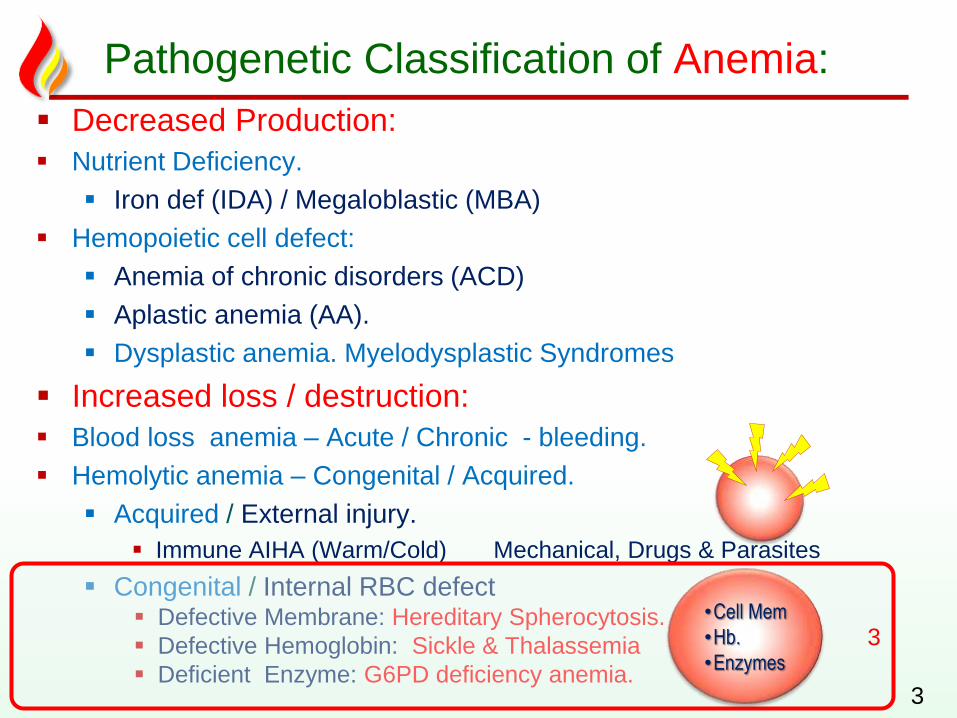
Pathogenetic Classification of Anemia:
Decreased Production:
Nutrient Deficiency.
Iron def (IDA) / Megaloblastic (MBA)
Hemopoietic cell defect:
Anemia of chronic disorders (ACD)
Aplastic anemia (AA).
Dysplastic anemia. Myelodysplastic Syndromes
Increased loss / destruction:
Blood loss anemia – Acute / Chronic - bleeding.
Hemolytic anemia – Congenital / Acquired.
Acquired / External injury.
Immune AIHA (Warm/Cold) Mechanical, Drugs & Parasites
Congenital / Internal RBC defect Defective Membrane: Hereditary Spherocytosis.
Defective Hemoglobin: Sickle & Thalassemia
Deficient Enzyme: G6PD deficiency anemia.3
3•Cell Mem
•Hb.
•Enzymes
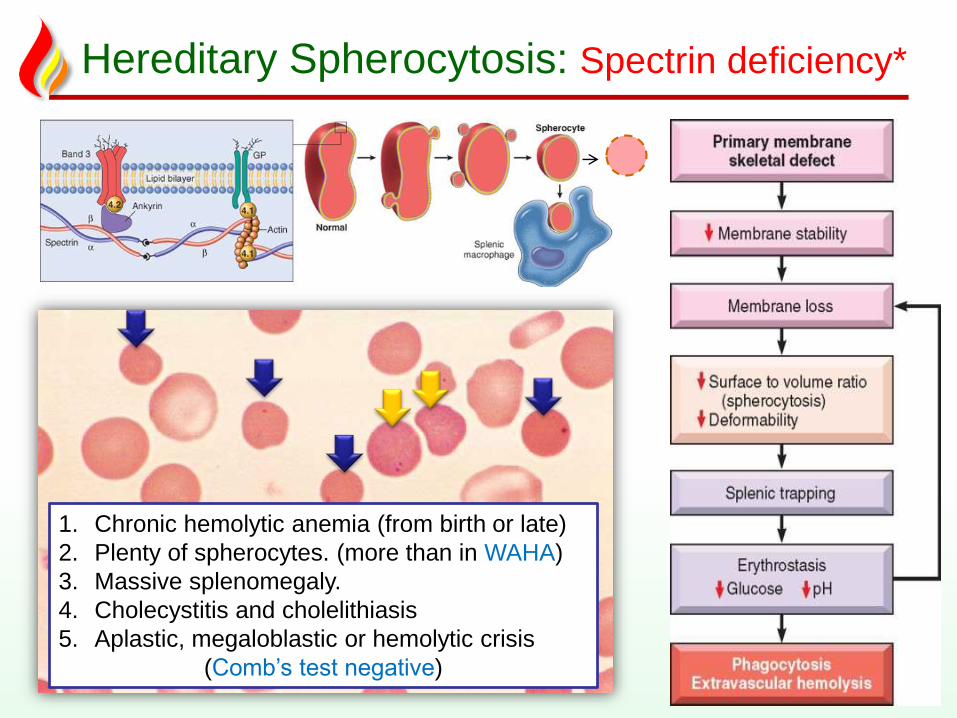
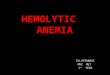
Hereditary Spherocytosis: Spectrin deficiency*
4
1. Chronic hemolytic anemia (from birth or late)
2. Plenty of spherocytes. (more than in WAHA)
3. Massive splenomegaly.
4. Cholecystitis and cholelithiasis
5. Aplastic, megaloblastic or hemolytic crisis
(Comb’s test negative)
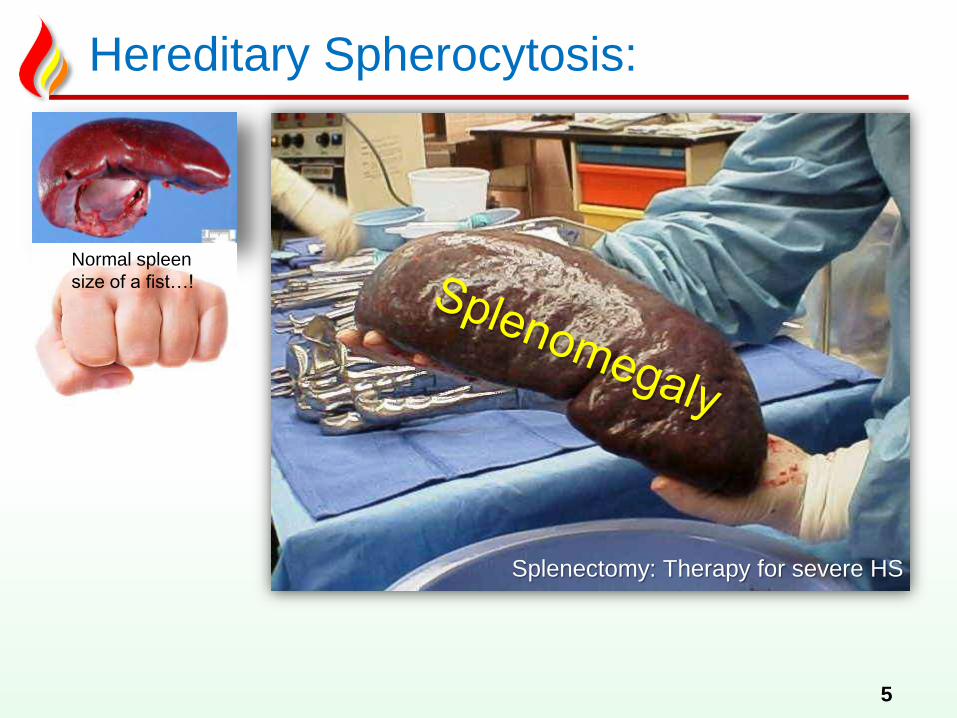
Hereditary Spherocytosis:
5
Normal spleen
size of a fist…!
Splenectomy: Therapy for severe HS
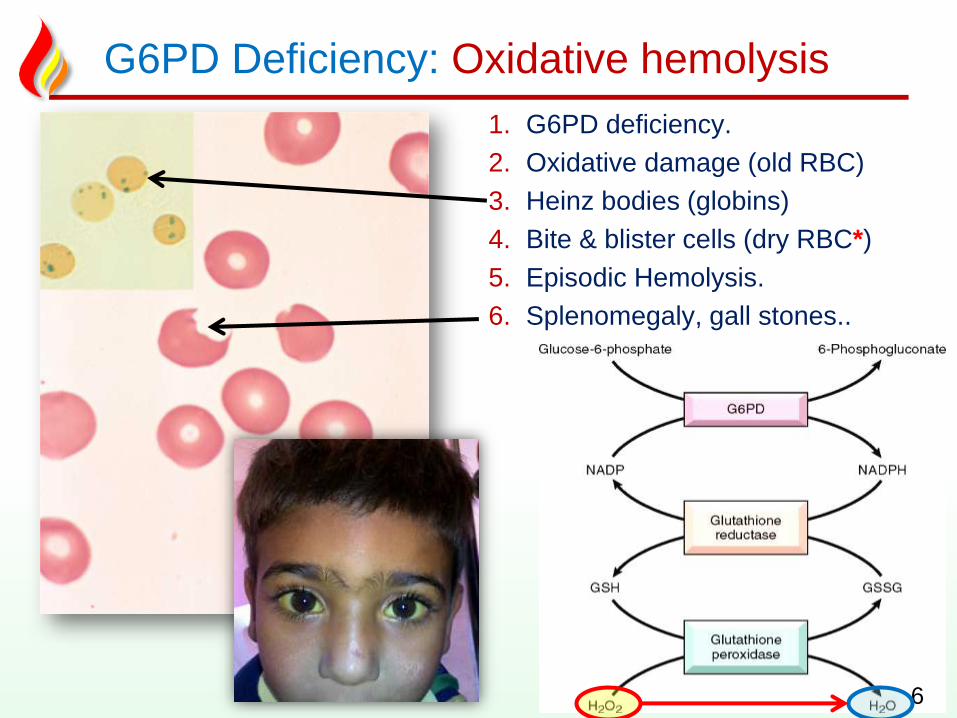
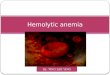
G6PD Deficiency: Oxidative hemolysis
1. G6PD deficiency.
2. Oxidative damage (old RBC)
3. Heinz bodies (globins)
4. Bite & blister cells (dry RBC*)
5. Episodic Hemolysis.
6. Splenomegaly, gall stones..
6
"Thinking should become your
capital asset, no matter whatever
ups and downs come across in
your life.
― Dr. APJ Abdul Kalam, Former President of India..
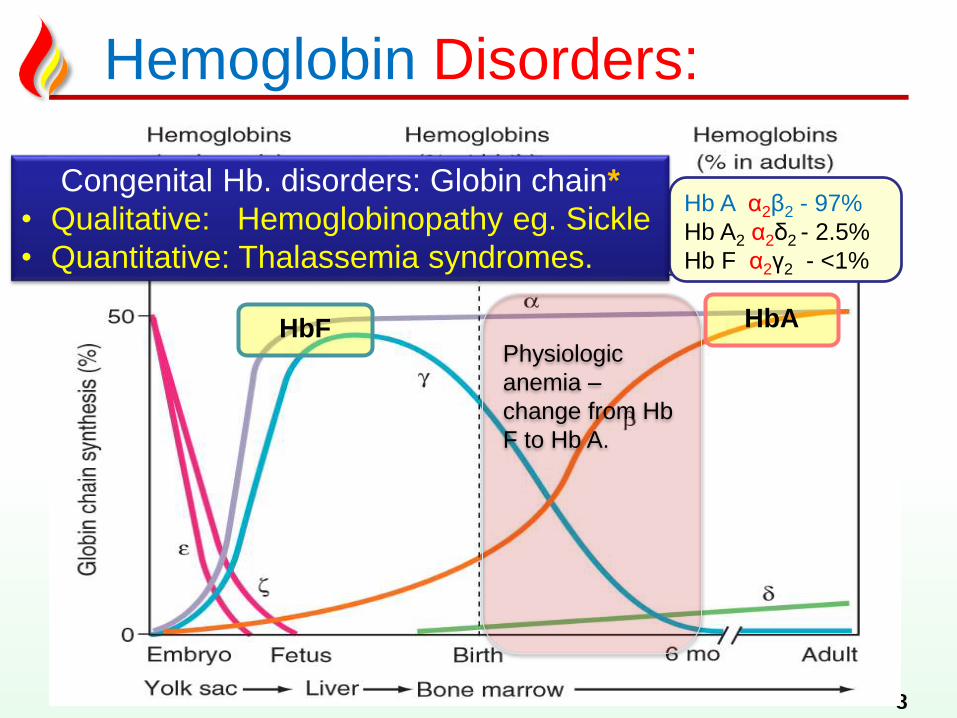
Hemoglobin Disorders:
8
Physiologic
anemia –
change from Hb
F to Hb A.
Hb A α2β2 - 97%
Hb A2 α2δ2 - 2.5%
Hb F α2γ2 - <1%
HbF HbA
Hb F - α2γ2- 75%
Hb A - α2β2 25%
Congenital Hb. disorders: Globin chain*
• Qualitative: Hemoglobinopathy eg. Sickle
• Quantitative: Thalassemia syndromes.
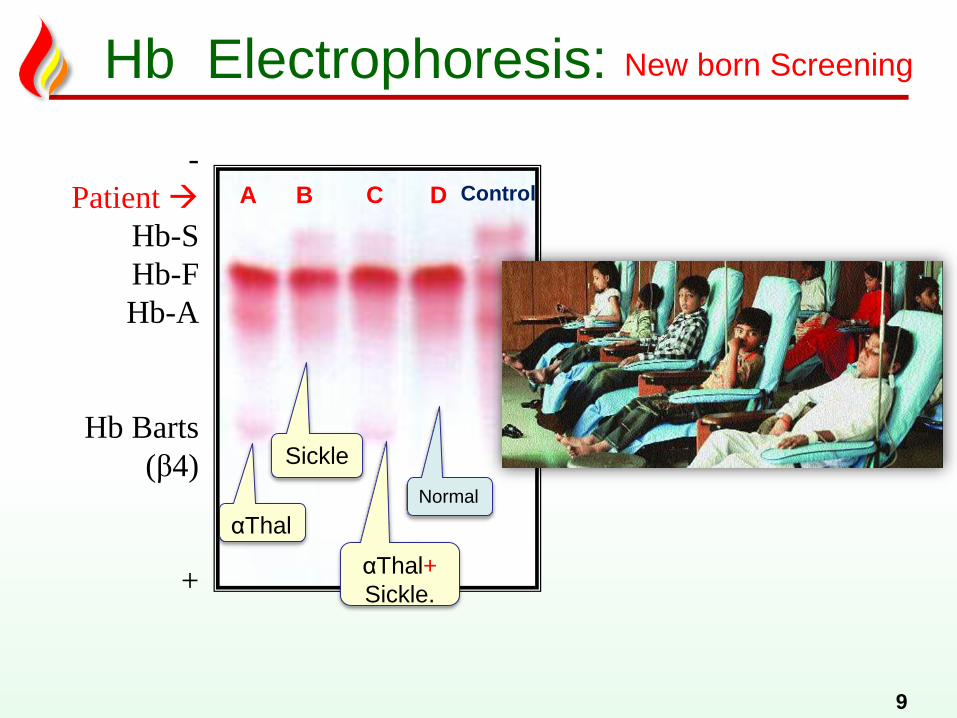
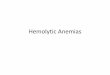
Hb Electrophoresis:
9
-
Patient
Hb-S
Hb-F
Hb-A
Hb Barts
(β4)
+
ControlA B C D
αThal
Normal
αThal+
Sickle.
Sickle
New born Screening
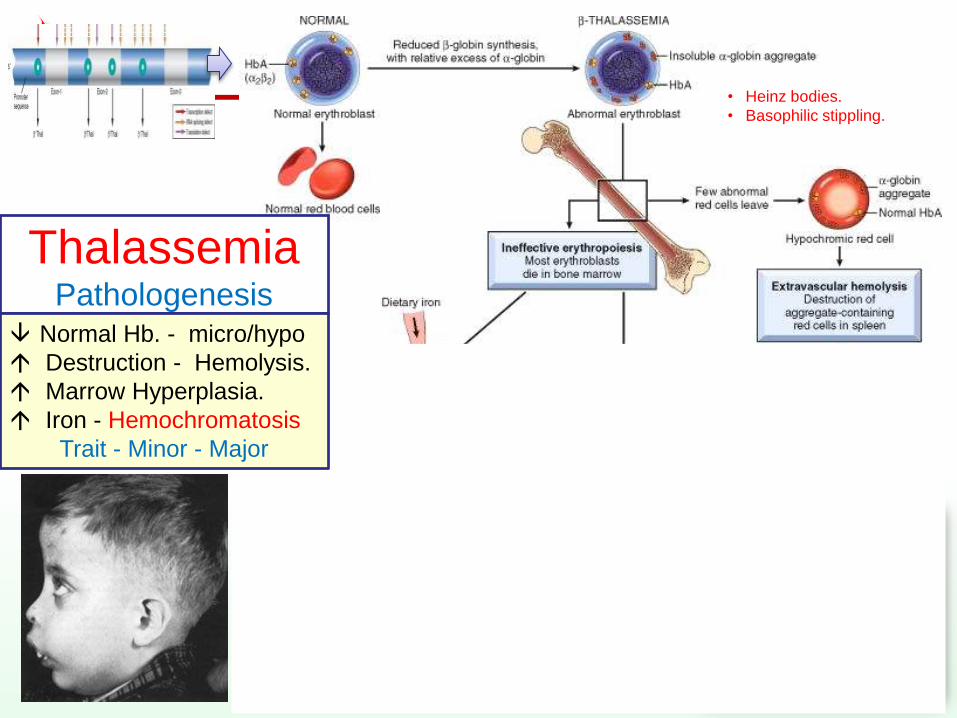
ThalassemiaPathologenesis
10
• Heinz bodies.
• Basophilic stippling.
Normal Hb. - micro/hypo
Destruction - Hemolysis.
Marrow Hyperplasia.
Iron - Hemochromatosis
Trait - Minor - Major
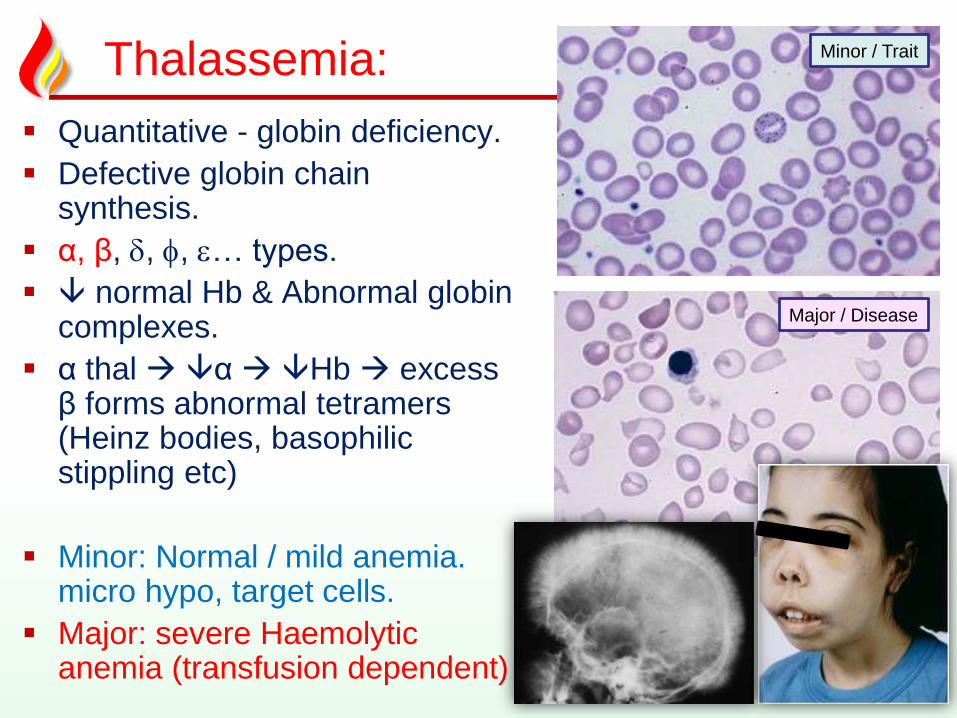
Thalassemia:
11
Quantitative - globin deficiency.
Defective globin chain synthesis.
α, β, , , … types.
normal Hb & Abnormal globin complexes.
α thal α Hb excess β forms abnormal tetramers (Heinz bodies, basophilic stippling etc)
Minor: Normal / mild anemia. micro hypo, target cells.
Major: severe Haemolytic anemia (transfusion dependent)
Minor / Trait
Major / Disease
"Thinking should become your
capital asset, no matter whatever
ups and downs come across in your life.
― Dr. APJ Abdul Kalam, Former President of India..
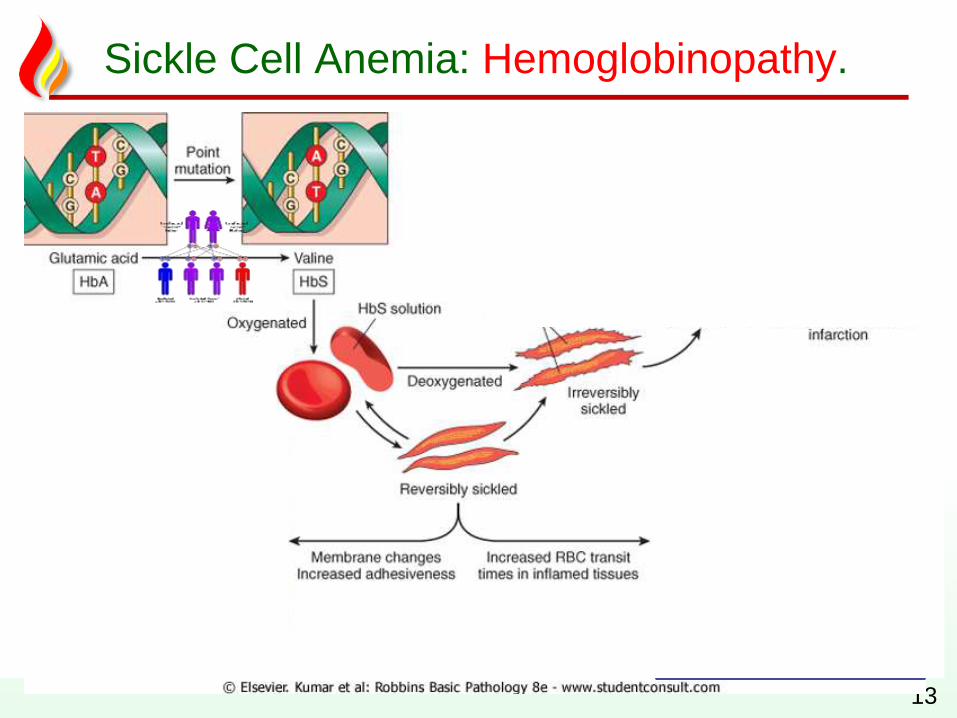
Sickle Cell Anemia: Hemoglobinopathy.
13
Acute Chest Syndrome
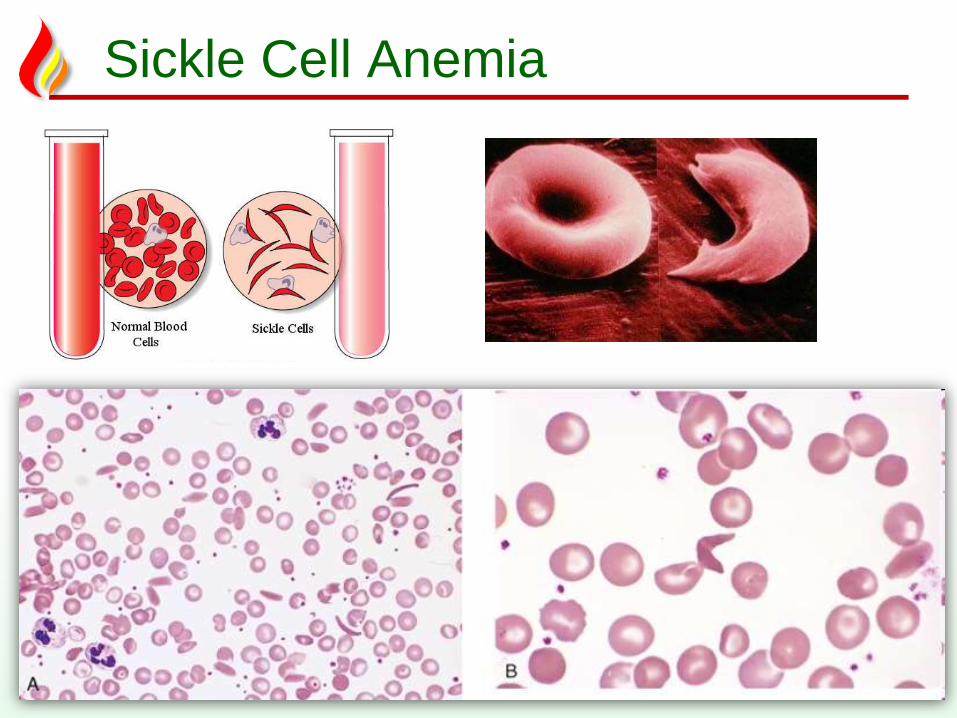
Sickle Cell Anemia
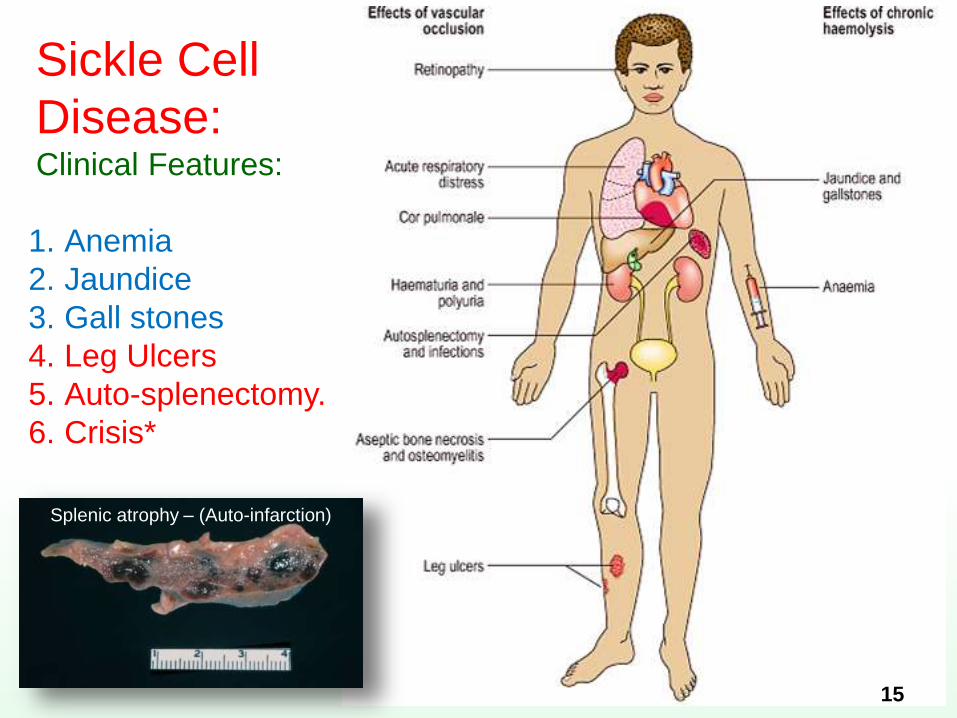
Sickle Cell
Disease:Clinical Features:
15
1. Anemia
2. Jaundice
3. Gall stones
4. Leg Ulcers
5. Auto-splenectomy.
6. Crisis*
Splenic atrophy – (Auto-infarction)
The power of thought is not a
compelling force. It is a building force,
and it is only when used in the latter
sense that desirable results can be
produced.
-- Christian D. Larson
Need help? contact me…
1. Office location: DB39-136 (Townsville)
2. Office Tel: 4781 4566
3. Email: [email protected]
4. Emergency?: 0416933704
Need personal coaching?Email me for an appointment.
You are the stone..
The pessimist waits for better times,
and expects to keep on waiting; the
optimist goes to work with the best
that is at hand now, and proceeds to
create better times.
-- Christian D. Larson