Embed Size (px)
Citation preview
Guidelines for Preventing Medication Errors in Pediatrics
The Pediatric Pharmacy Advocacy Group is a non-profit professional pharmacy association dedicated to improving the healthcare of all chil-dren. The sole purpose of PPAG is to advocate for safe and effective medication use in children through communication, education, and the promotion of research.
Pediatric Pharmacy Advocacy Group | 7975 Stage Hills Boulevard, Suite 6 | Memphis, Tennessee | 38133 Tele: 901.380.3617 | Fax: 901.266.4651 | www.ppag.org
J Pediatr Pharmacol Ther 2001;6:426-42
Endorsed by:
The Institute for Safe Medication Practices is a nonprofit healthcare agency comprised of pharmacists, nurses, and physicians. Founded in 1994, the organization is dedicated to learning about medication errors, understanding their system-based causes, and disseminating practical recommendations that can help healthcare providers, consumers, and the pharmaceutical industry prevent errors.
Brought to you by:

427
The Journal of Pediatric Pharmacology and Therapeutics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
REVIEW
Guidelines for preventing medication errors in pediatrics
Stuart R. Levine, PharmD, Michael R. Cohen, MS, Nicholas R. Blanchard, MEd,Frank Frederico, MS, Merrell Magelli, PharmD, Chris Lomax, PharmD, Gary Greiner,PharmD, Robert L. Poole, PharmD, Carlton K. K. Lee, PharmD, MPH,Anne Lesko, PharmD
From the Institute for Safe Medication Practices, Huntingdon Valley, Pennsylvania and ThePediatric Pharmacy Advocacy Group, Denver, Colorado
Medication errors commonly occur in healthcare facilities. Most literature has centered on med-ication errors and prevention of those errors in facilities that care primarily for adults. This article con-centrates on the medication errors that are common to pediatrics facilities, and recommends strategiesfor reducing the potential for medication errors in those settings. Methods reviewed include lookingat system deficiencies vs. the single practitioner, education programs that reduce the risk of error,strategies for reducing the potential of medication errors, use of automation, and benefits of a comput-erized prescriber order entry system.
Key words: Medication errors, patient safety, medication safety, pediatrics, computerized prescriberorder entry, automated dispensing devices, prescriptions
(J Pediatr Pharmacol Ther 2001;6:427-43)
In August 1998 the draft guidelines werepublished in the Journal of Pediatric PharmacyPractice.1 In order to stimulate discussion on thetopic of preventing errors in the pediatric popula-tion and to refine the draft guidelines this manu-script was written as a collaborative effortbetween the Institute for Safe MedicationPractices (ISMP) and the Pediatric PharmacyAdvocacy Group (PPAG). The following are theresults of that effort and represent the recommen-dations of these two organizations.
Medication error prevention is fundamentalin the care of all patients. Although many med-ication errors go unreported and are often unde-tected with minimal clinical significance, somemedication errors do result in serious morbidityor mortality. Certain patient populations areexposed, by inherent characteristics, to greater
Address correspondence and reprint request to Stuart R. Levine, PharmD, Director of Pharmacy,Alfred I. duPont Hospital for Children, 1600 Rockland Road, Wilmington, Deleware 19803
e-mail address: [email protected]
risk of medication error occurrence andincreased potential for morbidity. The pediatricpopulation is a high-risk group because thenumber of potential adverse drug events isthree times that found in hospitalized adultpatients.1 Factors placing pediatric patients atincreased risk for adverse drug reactions can befound in Table 1.3-9
The special treatment considerations of thispopulation provided impetus for a collabora-tion between the ISMP and the PPAG. A sym-posium was held prior to the 1997 AmericanSociety of Health System Pharmacists Mid-yearClinical Meeting in Atlanta, Georgia. This meet-ing included members of the ISMP and PPAG,as well as a panel of experts in the field. Inhopes of avoiding or decreasing the occurrenceof future medication errors in the pediatric pop-

428
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
ulation, this group discussed challenges involvedin medication error prevention in neonates,infants, and children and addressed methods toovercome these challenges. The session wasaudio taped and later reviewed in order to incor-porate salient points into this document.
Recommendations for the prevention of med-ication errors in the general hospitalized popula-tion11 and in patients receiving cancer chemother-apy12 have been published elsewhere. Whilemany previously published recommendationsapply to the pediatric population, this documentfocuses exclusively on this select patient groupand offers specific recommendations for the pre-vention of medication errors. Some of the recom-mendations presented in this document may reit-erate those published in previous documents.The purpose of this document is to recommenda-tion medication error prevention strategies forconsideration in the development of: 1) organiza-tional systems (e.g, computerized order entry sys-tems, automated dispensing systems, bar coding,robotics); 2) educational systems; and 3) manu-facturing and regulatory systems. The paper willalso suggest medication error prevention strate-gies for individual healthcare professionals.
ORGANIZATIONAL SYSTEMRECOMMENDATIONS
Medication errors rarely occur from the fail-ure of a single element or because of mistakes bysingle practitioner. Rather, medication errors arethe result of the combined effects of “latent fail-ures” in the system and “active failures” by indi-
viduals. Latent failures are weaknesses in thestructure of an organization, such as faulty infor-mation management or ineffective personneltraining, which result from both good- and ill-conceived decisions. By themselves, latent fail-ures are often subtle and may cause no problems.Their consequences are hidden, becoming appar-ent only when they occur in proper sequence andare combined with active failures of individualsto penetrate or bypass the system’s safety nets.Many of the latent and active failures that were atthe root of medication errors are not apparentuntil a root cause analysis is performed.13 For thisreason, providing an optimal level of medicationsafety requires both recognition and correction oflatent failures in the system. This document looksbeyond blaming individuals and focuses on themultiple underlying system enhancements thatcan shape individual behavior and create the con-ditions whereby medication errors may be pre-vented. It is unrealistic to expect absolute perfec-tion or error-free performance from any person.For this reason, it is essential that systems beestablished to minimize the risk of medicationerrors. In order to increase the number of oppor-tunities to detect and prevent medication errors,these systems should be highly redundant andshould be updated as new potential sources oferror are identified. In the post-medication errorevaluation process, system deficiencies should beidentified and corrected before placing all respon-sibility on human error.
Table 1. Factors placing pediatric patients at increased risk for adverse drug reactions3-9
• Different and changing pharmacokinetic parameters between patients at various ages and stagesof maturational development.10
• Need for calculation of individualized doses based on the patient’s age, weight (mg/kg), bodysurface area (mg/m2), and clinical condition.
• Lack of available dosage forms and concentrations appropriate for administration to neonates,infants, and children. Frequently, dosage formulations are extemporaneously compounded andlack stability, compatibility, or bioavailability data.
• Need for precise dose measurement and appropriate drug delivery systems
• Lack of published information or FDA-approved labeling regarding dosing, pharmacokinetics,safety, efficacy, and clinical use of drugs in the pediatric population.
FDA=Food and Drug Administration

429
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
Computerized Order Entry SystemRecommendations
Every healthcare provider has an occasional“bad day” or lapse in personal performance thatcould result in a medication error. For this rea-son, available technology should be used, espe-cially in situations where accuracy is critical. Inhealthcare, computers can provide technologicalsupport by providing information, facilitatingclear and accurate communication, alerting theuser to potential errors, and processing data. Theselection and programming of a computer systemshould be done with medication error preventionin mind. The computerized order entry processwill act as a firewall, which can reduce the risk ofmedication errors that subsequently occur inpatients. A variety of functions should be incor-porated into the “ideal” computer order entrysystem (Table 2).
Another item that should be consideredinvolves site-specific programming choices,which can make a system more helpful in the pre-vention of medication errors. These systems
should use only metric units and institution-approved standardized doses and concentrations.All decimal expressions less than one whole unitshould be preceded by a leading zero (i.e., 0.1 not.1) and whole numbers should not be followed bya trailing zero (1 mg not 1.0 mg).14 The use ofabbreviations for drug names should not be per-mitted. There should be an established link todata entry requiring input of up-to-date patientinformation (e.g., age, weight (in kilograms),allergies, diagnosis). The software should alsoscreen for allergies, large or small dosages, anddrug-drug, drug-nutrient, or drug-disease inter-actions and should sound or flash an alert when apotential problem is identified. For more seriouswarnings, a manual over-ride should be requiredand should be accompanied by appropriate doc-umentation. Caution should be exercised to avoidmanual over-rides for minor problems becausethis promotes automatic manual over-riding thatcould leads to a failure to appreciate the signifi-cance of the alert. Finally, there should be a setand utilize minimum and maximum dose rangebased on pediatric age, weight, and height
Table 2. Functions important to the “ideal” computer order entry system
• Prescriber order entry for verification by nurse and pharmacist
• Computer-generated medication administration records from a common data base shared withthe pharmacy and the prescriber
• For each patient, lists of current medications that are readily accessible by caregivers
• Two-way interface between the pharmacy and other institutional systems (e.g., laboratory, admis-sion and discharge, clinical records)
• Access to historical patient data (i.e., archived information)
• Ability to calculate and verify appropriate height-weight range and dosage for patient
• Access to vital patient and drug information directly from order entry, medication profile, andmedication administration screens
• Ability of system to use patient and drug information to provide unsolicited information duringorder entry to reduce potential for adverse drug events (e.g., drug interactions, contraindications,excessive doses, allergies). This should be part of a comprehensive decision support program.These programs would include checking for laboratory results and advising the prescriber of theneed for dosing modifications for specified medications. Automatic checking should also includedrug-drug interactions, drug-nutrient interactions, drug duplication, therapeutic duplication,contraindicated medications, weight-based dosage checking
• Provide a forced function by limiting the route and frequency by which a drug is ordered

430
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
parameters. Prescriber care sets may also belinked to patient weight in selecting drugdosages. Where applicable, the software shouldinclude set dose limits for single doses, 24-hourdoses, course of therapy, and lifetime doses. Thesystem should also contain a built-in growthchart to alert the user to obvious patient outly-ers.15
Because of the potential for selecting thewrong medication mnemonics should not beused. If it is determined by an organization toemploy mnemonics, then caution should be usedin selecting mnemonics, ensuring that: 1) no twomnemonics are so similar as to promote selectionerrors by bringing dissimilar items onto thescreen at the same time; 2) separate selections areavailable for intravenous products which aregiven by a different route. For example, a sepa-rate computer file should exist for amphotericin Bintranasal administration versus intravenousadministration to prevent IV administration ofthe intranasal dosage form; and 3) potentiallymisleading abbreviations are not incorporated inthe mnemonics.
The final item important in site-specific pro-gramming choices involves the selection of labelsand label set-up programs. These systems shouldensure that:
• labels are easy to read• all vital information is included and extrane-
ous information is excluded• the most important information is empha-
sized through typeface and placement (e.g.,patient name, drug name, concentration,dose, and route)
• appropriate spacing is used between terms• laser printers are used in order to provide the
greatest clarity• leading zeros are used (0.1 mg) and trailing
zeros are omitted (1.0 mg)• dangerous abbreviations are not used.10
Computerized prescriber order entry systemsare one of the many tools that are used as amethod of medication error reduction. No onedevice or technology will eliminate all errors. It isonly through the coordinated use of elements of amedication error reduction strategy that we canimprove the safety of our patients.
Automated Dispensing SystemsRecommendations
In addition to computerized prescriber orderentry, there are several other technologies avail-able to today’s healthcare system. While there aresome timesaving elements associated with tech-nologies, it is important to review their potentialfor errors in the pediatric population.
Automated dispensing devices (ADD) havebecome very common technology. They aredesigned to reduce some of the staffing burdensand allow for reassignment of staff to provideclinical services. While this may be true in somehospitals, implementation of this technology maydecrease the use of traditional methods that areemployed to enhance safety and may actuallyincrease the number of medication errors.Several issues must be in place before ADDs areused (Table 3).
Bar code technology is moving to the patientbedside and can help assure that the right drug,correct time, precise dosage and right patient areselected. It can also document the identity of theperson administering the medication. Because astandardized Universal Product Code (UPC) hasnot been created for the dose level, bar code labelsmust be prepared for each distinct unit dose.
Robotics for centralized automated dispens-ing has increased over the last few years. As withthe ADD, care must be taken not to move awayfrom the unit dosing of medications for the pedi-atric population. In some cases, standardizeddoses can be employed to help implement anduse the robotic technology in the pediatric setting.
Other System Recommendations
While our recommendations apply primarilyto the provision of healthcare in the institutionalsetting, some of the general ideas and principlesmay be adapted for use in other practice settings.Institutions dedicated solely to the treatment ofpediatric patients may find it easier to create andenforce policies and procedures directed towardthe prevention of medication errors in this specif-ic population, but all facilities involved in thetreatment of pediatric patients should assume theresponsibility for identifying and implementing
431
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
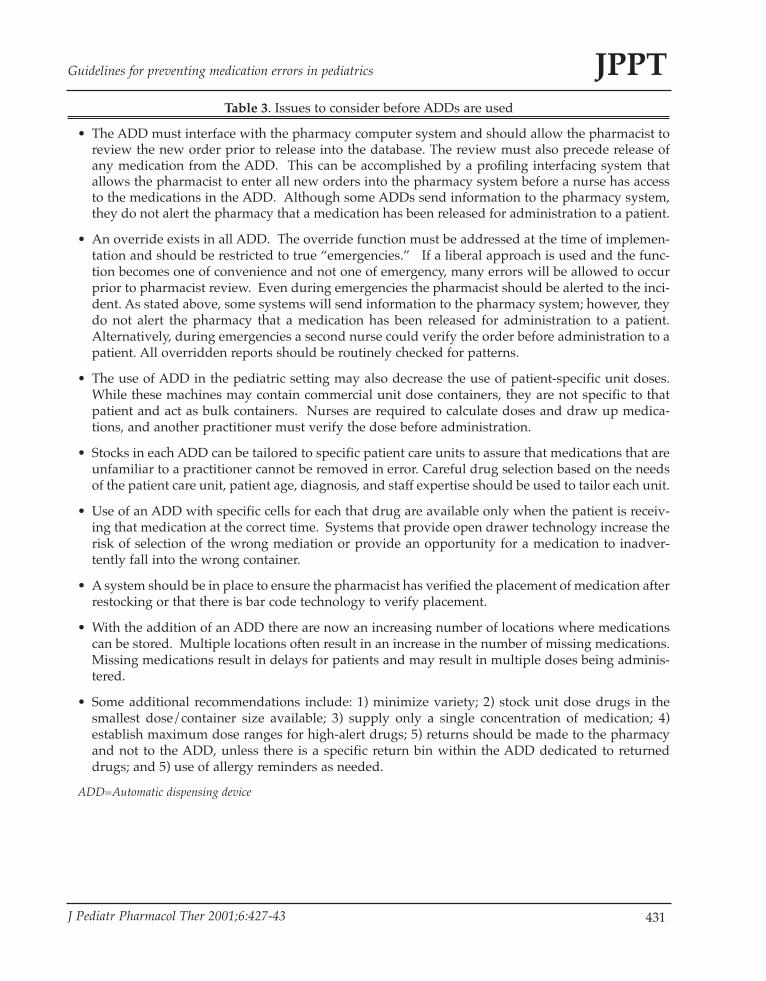
Table 3. Issues to consider before ADDs are used
• The ADD must interface with the pharmacy computer system and should allow the pharmacist toreview the new order prior to release into the database. The review must also precede release ofany medication from the ADD. This can be accomplished by a profiling interfacing system thatallows the pharmacist to enter all new orders into the pharmacy system before a nurse has accessto the medications in the ADD. Although some ADDs send information to the pharmacy system,they do not alert the pharmacy that a medication has been released for administration to a patient.
• An override exists in all ADD. The override function must be addressed at the time of implemen-tation and should be restricted to true “emergencies.” If a liberal approach is used and the func-tion becomes one of convenience and not one of emergency, many errors will be allowed to occurprior to pharmacist review. Even during emergencies the pharmacist should be alerted to the inci-dent. As stated above, some systems will send information to the pharmacy system; however, theydo not alert the pharmacy that a medication has been released for administration to a patient.Alternatively, during emergencies a second nurse could verify the order before administration to apatient. All overridden reports should be routinely checked for patterns.
• The use of ADD in the pediatric setting may also decrease the use of patient-specific unit doses.While these machines may contain commercial unit dose containers, they are not specific to thatpatient and act as bulk containers. Nurses are required to calculate doses and draw up medica-tions, and another practitioner must verify the dose before administration.
• Stocks in each ADD can be tailored to specific patient care units to assure that medications that areunfamiliar to a practitioner cannot be removed in error. Careful drug selection based on the needsof the patient care unit, patient age, diagnosis, and staff expertise should be used to tailor each unit.
• Use of an ADD with specific cells for each that drug are available only when the patient is receiv-ing that medication at the correct time. Systems that provide open drawer technology increase therisk of selection of the wrong mediation or provide an opportunity for a medication to inadver-tently fall into the wrong container.
• A system should be in place to ensure the pharmacist has verified the placement of medication afterrestocking or that there is bar code technology to verify placement.
• With the addition of an ADD there are now an increasing number of locations where medicationscan be stored. Multiple locations often result in an increase in the number of missing medications.Missing medications result in delays for patients and may result in multiple doses being adminis-tered.
• Some additional recommendations include: 1) minimize variety; 2) stock unit dose drugs in thesmallest dose/container size available; 3) supply only a single concentration of medication; 4)establish maximum dose ranges for high-alert drugs; 5) returns should be made to the pharmacyand not to the ADD, unless there is a specific return bin within the ADD dedicated to returneddrugs; and 5) use of allergy reminders as needed.
ADD=Automatic dispensing device

432
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
measures necessary to protect this populationfrom medication errors.
A strong formulary system that is governedby the Pharmacy and Therapeutics (P & T)Committee should be operational and shouldconsist of physicians, pharmacists, nurses, riskmanagers, and other healthcare professionals. Ifthe facility is not dedicated entirely to the treat-ment of pediatric patients, the departmentsshould ensure sufficient representation of all dis-ciplines within this specialty on the P & TCommittee. Alternatively, a subcommittee of theP & T Committee could be appointed to considerand make recommendations regarding pediatric
formulary considerations. The committee shouldcreate and enforce policies regarding evaluation,selection, prescribing, and use of drugs anddevices for pediatric patients within the organ-ized health care setting (Table 4). Likewise, thecommittee should establish standardized dosing,medication concentrations, drug administrationschedules, and abbreviations. The committeeshould also encourage the use of metric units ofmeasurement and the rounding of odd doses.
It is also imperative that policies and proce-dures are developed to ensure adequate person-nel selection, training, supervision, and evalua-tion. These policies and procedures should
Table 4. Formulary management
The P&T Committee should:
• ensure that drugs are appropriate for use in the pediatric population (e.g., concentrations, dosageforms, inactive ingredients).
• guarantee that all devices (e.g., pumps, compounding devices, burette chambers) selected for useare appropriate for the pediatric population. Procedures for appropriate use of all institutionallyaccepted medication administration devices (i.e., enteral and parenteral) should be detailed anddistributed to all patient care areas. These procedures should be delivery system specific and, whenappropriate, drug and/or administration route specific.6,8,16,17 The ability of a device or set to per-mit free-flow should be evaluated prior to acceptance.
• make certain that special oral syringes used within the institution are not compatible with needlesand needleless IV systems or parenteral catheters.
• ensure that appropriate measuring devices should be available for oral administration and param-eters should be set to address minimum measurable volumes for these devices (i.e., measuring 0.2mL in a 10 mL syringe).
• ensure that at the time of formulary review potential medication errors are evaluated. The com-mittee should determine if the medication: 1) sounds (i.e., verbal order confusion) or looks (i.e.,written order confusion) like another drug on formulary; 2) uses packaging that appears similar toother drugs on formulary; 3) requires the performance of certain tests as part of monitoring toassure safely; 4) is associated with clearly defined dosing information; and 5) allows for standard-ized dosing that can be used in order to decrease the number of calculations required.
• approve clinical pathways, protocols, preprinted orders, dose calculation forms, etc. via a multi-disciplinary team or the committee should appoint and oversee a multidisciplinary team for thispurpose.
• be involved in computer software and ADD decisions.
• review methods for ordering total parenteral nutrition and limit choices to mg/kg/day foryounger children and per liter for older children.
P&T = Pharmacy and Therapeutics Committee; ADD = automated dispensing devices

433
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
include proper interviewing procedures, staff ori-entation and development programs (includingthe discussion of medication errors), and shouldconsist of regular (annual, biannual) age-relatedcompetency evaluations that include calculationskills and opportunities for continuing educationspecific to pediatrics.18-22 While it is essential thatpersonnel who regularly serve this patient popu-lation be well trained and competent, it is veryimportant that personnel who work with thispopulation less frequently be competent; there-fore, these personnel should also be required toparticipate in any training and competency eval-uations required of regular employees in thisarea. These policies and procedures should alsoestablish reasonable workload levels and work-ing hours and ensure, through adequate staffing,that these quotas are rarely exceeded.
The work environment where drugs are pre-pared or administered should be free of potentialfactors that contribute to medications errors.These include high noise or traffic, poor lighting,temperature extremes, and distractions or inter-ruptions.
A unit dose dispensing system should be inplace and the pharmacy department, should pre-pare and dispense individual patient doses inready-to-administer form to minimize the needfor manipulation of drug products outside of thepharmacy.3,8,20 In order to facilitate communica-tion and exchange of information among thehealthcare team, pharmacists should be as acces-sible as possible, participating in patient roundsand/or working in or near patient care areas.
A highly redundant system of checks shouldbe instituted for the entire medication deliveryprocess from ordering of the medication, topreparation and dispensing of the drug, toadministration of the medication. This wouldprovide numerous opportunities for the discov-ery of potential medication errors before theyreach the patient.23,24 Documentation of anyrequired change or alteration in medicinal thera-py is also very important. The system shouldprovide for review and verification of the pre-scriber’s original order prior to the dispensing ofthe drug (except in emergency situations). Toprevent the occurrence of drug administrationwithout appropriate review, floor stock should be
eliminated or limited to very low risk medica-tions or automated dispensing modules shouldbe available and all orders should be screened bya pharmacist.14,21
With the increasing use of automated dis-pensing devices pharmacists have lost some con-trol over medication dispensing. A feature avail-able on many automated dispensing systems can,and should, be used to minimize the potentialerror to patients receiving a high-risk drug priorto appropriate order review and verification. Thisfeature enables a lock to be placed on selecteddrugs so that they cannot be retrieved from themachine until the order has been screened andtheir dispensing has been authorized.14
In children’s hospitals, the standard of carecalls for 24-hour pharmacy operation.3 In otherhospitals with pediatric patients, selected med-ications should be available in a designated areawhen a pharmacist does not provide 24-hourpharmacy services and automated dispensingsystems are not in use. After-hours when thepharmacy is closed, pharmacy access by non-pharmacy personnel is deemed unsafe and unac-ceptable. In addition, when 24-hour pharmacyservice is not provided, a pharmacist should beavailable “on-call” to answer questions and pre-pare medications as necessary.
Another potential source for error involvesverbal ordering. This practice should be avoidedwhenever possible. Policies and proceduresshould be established and should specify accept-able circumstances for this practice and personnelpermitted to accept this type of order. Directiveto repeat back the order for verification and clearrequirements for documentation of these orders,including the time frame in which the prescribermust verify and sign the order should be includ-ed in the policies. The use of computerized pre-scriber order entry, approved and preprintedorders, and facsimile transmission of ordersshould be used to the maximum extent possibleto eliminate verbal ordering.
Clear and accurate labeling of all drug andnutrition products is very important. Labelsshould clearly express all pertinent informationrequired for verification of contents by otherhealthcare professionals. Auxiliary labels shouldalso be used in situations where they might

434
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
emphasize an important aspect of the product.With respect to the safe use of medications,
there should be an ongoing, multidisciplinaryprogram of quality improvement and peer reviewthat includes a formal drug-use evaluation pro-gram, and a system for monitoring, reporting,and reviewing medication errors. Policies shouldbe established that not only eliminate the fear ofreporting errors, but encourage an increased dis-cussion of errors that have occurred in-house andelsewhere in the practice of medicine.21 A newslet-ter or other hospital- or department-wide publi-cation should be created for the dissemination ofthis information.23 One of the most importantmethods for preventing adverse drug events isfor institutions to seek and use knowledge fromother institutions that have already solved similarproblems. Staff should regularly monitor publi-cations such as the ISMP Medication Safety Alert!,the FDA Medical Bulletin, and other publicationsthat contain such information. Ultimately, thereshould be a mechanism to provide feedback to allstaff members on current and common types ofmedication errors within their healthcare system.In those facilities with medical residents, it is ben-eficial to establish a relationship with the chiefresidents and incorporate medication error reduc-tion strategies within the resident training cur-riculum.
All healthcare workers involved in patientcare should have ready access to appropriate andcurrent clinical information about patients (e.g.,weight, medications, allergies, diagnoses, labora-tory values) to aid in the appropriate selection ofmedications, calculation of doses, and evaluationof orders. Current references should be easilyaccessible when they are need and should belocated through out the facility. These referencesshould include Internet access to medical infor-mation, texts and publications, and institution-specific resources. Information available in thereferences should include appropriate uses of themedication, precautions, drug-drug interactions,drug-nutrient interactions, adverse effects,instructions for administration or infusion meth-ods, usual doses, and patient information andinstructions.10 Expired texts must not be used forroutine drug information because updated infor-mation or corrections of previous errors will not
be available. Computerized up to date druginformation systems (i.e., CD-ROM), such asMicromedex® or Facts and Comparisons® shouldbe available to healthcare providers for ease ofaccess to current information. Centrally updatedcomputerized systems have the advantage of lim-iting the availability of outdated references andproviding timelier updating of information.Institution-specific references should be created,incorporating standardized doses accepted by theinstitution, standardized concentrations availablewithin the institution, and osmolality informationfor intravenous and oral medications.7,25 Otherinstitution-specific information, such as restric-tions on prescribing or administration imposedby hospital policy may also be included.7,25 Thesereferences should be available in all areas wheremedications are prescribed, prepared, monitored,and administered, and as a pocket-sized version(hardcopy or electronic) for convenient carrying.23
A critical care drug (emergency medication)dosage calculation sheet should be completedand required for each pediatric critical carepatient. Standard sheets for a spectrum ofweights should be available as a reference in theevent that a patient requires emergency treatmentprior to the completion of their individualizeddosage sheet.26,27
Policies should be established that requiredocumentation of the actual time of medicationadministration, rather than simply documentingadministration, which can lead to the assumptionthat every dose is administered exactly on sched-ule. Where appropriate, method of administra-tion should also be recorded. Newer technologieswill allow for the electronic documentation ofadministration. Precise information facilitatesaccurate interpretation of laboratory data, phar-macokinetic calculations, and appropriate doseand/or interval adjustments.4,28
EDUCATIONAL SYSTEMRECOMMENDATIONS
An early step toward the prevention of med-ication errors is the education of healthcare pro-fessionals involved in medication prescribing,preparation, labeling, dispensing, monitoring,and administration. Training programs for all

435
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
healthcare professionals should include a varietyof items on errors (Table 5).30
In order for physicians to be prepared toenter practice their training should includeinstruction in the basic requirements of prescrip-tion writing. They should know that every pre-scription should be printed legibly and shouldcontain a variety of information (Table 6). At aminimum, items to be included on the prescrip-tion include the patient’s name, date of birth, cur-rent weight, allergies, and any additional patient-specific data appropriate to the circumstance. Inaddition, generic drug name, drug strength orconcentration, dose volume expressed in metricunits dosage form, quantity to be dispensedexpressed in metric units, complete directions foruse including dose, any calculations used indetermining the dose, route of administration,and frequency of dosing, purpose of the drug, thenumber of authorized refills or intended durationof therapy, and prescriber’s name should beincluded with each prescription. Additionally,instruction should address what not to incorpo-rate in a prescription (e.g., certain dangerous
abbreviations, leading and trailing zeros).9-11
These practices would save physicians time, aswell as the time of other healthcare professionals,and help avoid medication errors.26,30
Writing Discharge Prescriptions
Continuity of care is a method of reducingpotential medication errors. Almost 70% of hos-pital admissions related to adverse drug eventsare associated with patient compliance.33 Cleardirections for the patient or caregiver, as well asthe community pharmacist or nurse will assist inincreasing compliance. Continuity begins withthe prescription. Elements of a prescription aredepicted in Table 6.
MANUFACTURING AND REGULATORYSYSTEMS
Historically, pharmaceutical manufacturershave rarely conducted research in the pediatricpopulation. This lack of research occurs of a vari-ety of reasons including liability concerns, greater
Table 5. Suggested components for training programs for all healthcare professionals
Training programs for all healthcare professionals should include:
• courses to build and reinforce communication skills among healthcare professionals and improvecommunication with patients and their caregivers. It is important for all healthcare professionalsto learn the real potential for human error23 and to recognize the need to function as a team usingeach other as resources to achieve optimal patient care. Instruction in medication error preventionshould also be included at the earliest levels of all healthcare training programs and as part of ori-entation programs within each organized healthcare facility.
• instruction and practice in performing the mathematical calculations used in patient care. Testingshould be performed to assure that common causes of medication errors are recognized and under-stood. This includes unit conversions, calculations of dose, calorie and fluid requirements, and dos-ing intervals, and pharmacokinetic calculations. With more practice comes greater confidence andfewer errors.18,26,30 Errors involving 10-fold over- or under-doses are common. Other commonerrors involve calculating intravenous (IV) infusion rates, using a daily dose as the individual doseor dividing a daily dose by the time interval instead of the number of times to be administered perday (i.e., dividing a daily dose by 6 for an every six hour schedule).
• extensive education regarding patient populations such as pediatric patients with special needsand treatment considerations.3
• instruction and education with regard to patient monitoring. Health care providers should beskilled in interpretation of laboratory data, physical signs and symptoms, and adverse drug reac-tion recognition and reporting.
436
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
investments of time and money to conduct clini-cal trials in this population, and (perhaps mostsignificantly), a limited economic return becausethis population comprises only a small portion ofthe pharmaceutical market. The lack of pediatricresearch by pharmaceutical manufacturers hasresulted in the majority of drugs entering themarket and being used “off-label” in neonates,infants, or children with little or no dosing, phar-macokinetic, safety, efficacy, or clinical data.Pharmaceutical manufacturers and FDA havebecome increasingly aware of the challenges fac-ing pediatric healthcare professionals. Althoughthis population has long been recognized asunique and referred to as “therapeutic orphans,”
only recently have changes have occurred thatnow require new medications to be evaluated inpediatric patients.34
In addition to guidelines published previous-ly for pharmaceutical manufacturers and regula-tory agencies regarding the naming, labeling, andpackaging of drug products, the following arerecommended:
1. More research should be conducted in pedi-atric patients to determine safety and efficacyin neonates, infants, and children. Thereshould be established pediatric dosage guide-lines, including the dosing adjustmentsrequired for renal and hepatic dysfunction.The industry should identify pediatric-specif-
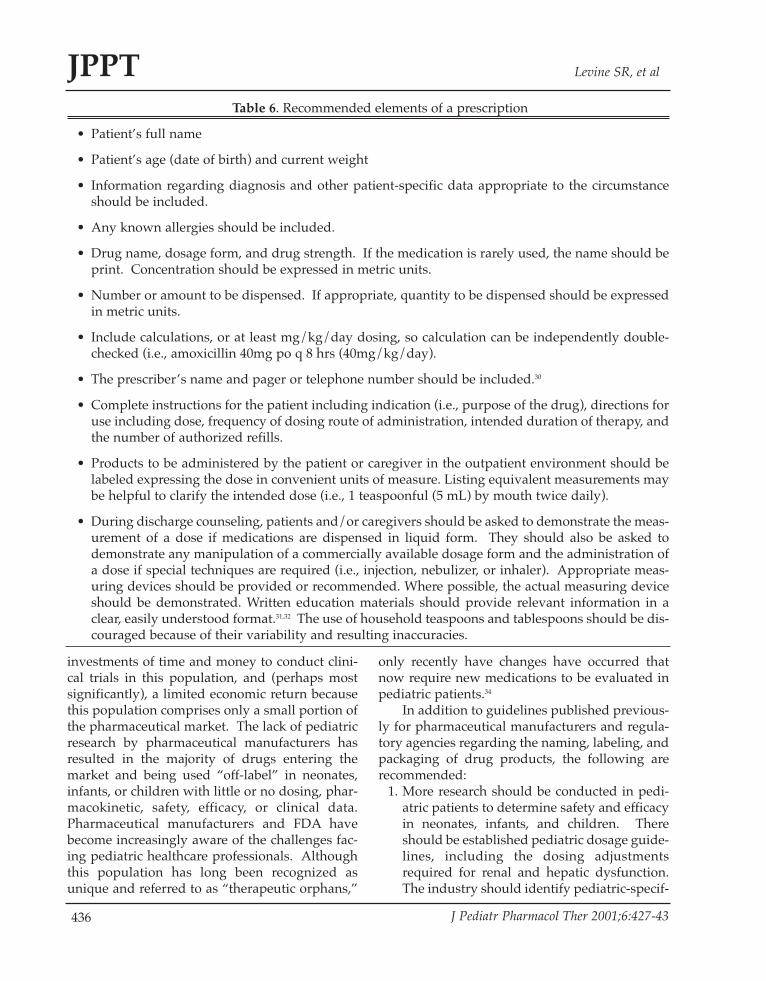
Table 6. Recommended elements of a prescription
• Patient’s full name
• Patient’s age (date of birth) and current weight
• Information regarding diagnosis and other patient-specific data appropriate to the circumstanceshould be included.
• Any known allergies should be included.
• Drug name, dosage form, and drug strength. If the medication is rarely used, the name should beprint. Concentration should be expressed in metric units.
• Number or amount to be dispensed. If appropriate, quantity to be dispensed should be expressedin metric units.
• Include calculations, or at least mg/kg/day dosing, so calculation can be independently double-checked (i.e., amoxicillin 40mg po q 8 hrs (40mg/kg/day).
• The prescriber’s name and pager or telephone number should be included.30
• Complete instructions for the patient including indication (i.e., purpose of the drug), directions foruse including dose, frequency of dosing route of administration, intended duration of therapy, andthe number of authorized refills.
• Products to be administered by the patient or caregiver in the outpatient environment should belabeled expressing the dose in convenient units of measure. Listing equivalent measurements maybe helpful to clarify the intended dose (i.e., 1 teaspoonful (5 mL) by mouth twice daily).
• During discharge counseling, patients and/or caregivers should be asked to demonstrate the meas-urement of a dose if medications are dispensed in liquid form. They should also be asked todemonstrate any manipulation of a commercially available dosage form and the administration ofa dose if special techniques are required (i.e., injection, nebulizer, or inhaler). Appropriate meas-uring devices should be provided or recommended. Where possible, the actual measuring deviceshould be demonstrated. Written education materials should provide relevant information in aclear, easily understood format.31,32 The use of household teaspoons and tablespoons should be dis-couraged because of their variability and resulting inaccuracies.

437
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
ic adverse drug reactions and should includeinformation in ‘a’ through ‘e’ in the officialproduct labeling. Formulate standard guide-lines must be in place for the extemporaneouscompounding of pediatric dosage forms fromcommercially available dosage forms whennecessary. These guidelines must includedata regarding product stability, compatibili-ty, and bioavailability. Companies shouldalso develop drug delivery devices and infu-sion systems appropriate for pediatricpatients of all ages.
2. Increase commercially available pediatricdosage forms, especially for those drug prod-ucts with pediatric indications. This wouldensure that dosage form and concentrationare appropriate for the pediatric populationand intended route of administration andwould facilitate accurate measurement ofdoses.3,8,17 Dose volumes of oral liquids andintravenous medications should be largeenough to measure accurately, but not toolarge to create a medication administrationchallenge. Oral products should be availablein palatability of dosage forms. Finally,appropriateness of all ingredients, includinginactive ingredients (e.g., preservatives suchas benzyl alcohol) should be considered. 3,8,10,17
3. Because look-alike products may lead tomedication errors, similar proprietaryappearances of packaging and labelingshould be avoided for both prescription andnon-prescription drug products.
4. Look-alike or sound-alike trademarked andgeneric names, as well as brand name lineextensions, should be avoided for prescrip-tion and non-prescription drug products,including store or generic brand over-thecounter products. What is known as “tall-man lettering” should be utilized to distin-guish medications with similar looking brandand generic names (i.e., hydrOXYzine vs.hydrALAzine).
5. Manufacturers should employ failure modeand effects analysis or similar techniques thatrequire practitioners to systematically assessthe potential for error with packaging, label-ing, and nomenclature prior to marketlaunch.13
6. Standardization of uniform bar coding thatwould be compatible with computer systemsused in organized healthcare settings shouldbe developed.
7. Standardization of calcium, zinc, and ironproduct concentrations should occur.9 Thismight include standardizing the ordering ofthese products to milliequivalents, millimolesor milligrams of the elemental product.
8. Healthcare professionals should be informedabout new drugs and their indications usingunbiased information and educational pro-grams. At a minimum, education shouldinclude indications for use, adverse drugreactions, and drug-drug and drug-nutrientinteractions.
9. Labeling of non-prescription medicationsmust clearly differentiate between multipleconcentrations. It should also provide clearwarnings, and usage and dosing informationfor patients and caregivers.35 Dosage infor-mation should be expressed as units of meas-ure that correspond to the calibration on thedosing device. Information should be includ-ed that warns that the measuring device doesnot necessarily represent one dose. Ideally,dosing devices should be calibrated in onlyone system of measure, preferably the metricsystem, contain no abbreviations, and bemarked in a contrasting color.36
HEALTHCARE PROFESSIONALS
Although errors are most often due to systemdeficiencies or failure, individual healthcare pro-fessionals also play a role in the prevention ofmedication errors. Every healthcare professionalshould accept responsibility for providing his orher patients with the best care possible by:37
1. keeping informed of medical knowledge,especially as it pertains to the treatment ofpediatric patients through review of the med-ical literature review, continuing educationprograms, and communication with otherhealthcare professionals.
2. actively participating as a member of thepatient care team, sharing information, wel-coming the input of colleagues, and beinginvolved in staff development and education

438
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
programs.3. carefully performing and double-checking
calculations to ensure correctness.19,20
4. consulting literature, references, and/or col-leagues when unsure of appropriate prescrip-tion, preparation, or administration of a drugproduct or pediatric treatment requirements.
5. ascertaining that all pertinent patient infor-mation is available and current so that apatient’s total status and appropriateness oftherapy can be evaluated.
6. focusing on a single task, avoiding distrac-tions and interruptions whenever possible, tomaintain concentration.
7. participating in multidisciplinary committeesto improve system functions.
Recommendations for Prescribers
The first individual who can take steps to pre-vent the occurrence of a medication error is theprescriber. Drug orders should be legible. Directprescriber computer order entry is preferable andshould be used by all institutions and all pre-scribers.38 Handwritten prescriptions or ordersincrease the occurrence of transcription errorsand fail to utilize the information and safetychecks available via the computer system. Whenprescriber computer order entry is not available,prescribers with poor handwriting should printor type medication orders. Preprinted orders areanother option for the prescriber with poor hand-writing; however, a multidisciplinary team of theP&T Committee must approve these.
Drug orders should be complete and shouldinclude the components described in Table 6.Likewise, prescribers should also adopt the fol-lowing measures to ensure that the clear intent ofthe order is communicated.
1. Drug name should be either the official(generic) or trademarked name clearlyspelled. For those medications that containmultiple ingredients, the use of the tradename is more appropriate. When the tradename is used, the generic ingredients shouldalso be listed on the label. Abbreviations ofthe name, acronyms, and chemical or locallycoined names should not be used becausethey might be misunderstood.
2. Instructions should be written out, ratherthan expressed using abbreviations that areambiguous or not approved within the insti-tution.
3. Vague instructions, such as “take as direct-ed,” should not be used.
4. Because many medications are available invarying strengths or concentrations, dosagestrengths or concentrations and volumesshould be expressed in exact metric units(e.g., mg, units), rather than dosage formunits (e.g., # tablets, vials, ampules, capsules,mL).
5. A leading zero should always precede deci-mal expressions less than one (i.e., 0.1 mg),but a trailing zero should never follow awhole number (i.e., 1.0 mg).
6. To facilitate verification of the appropriate-ness of the dose by other healthcare profes-sionals, any calculations used in determiningthe dose should be included in the medica-tion order.
7. For medications other than most topicallyadministered, both the calculated dose ANDthe mg/kg or mg/m2 dose upon which thedose is based should appear in all medicationorders for pediatric patients. This simple stephelps assure that a nurse and/or pharmacistdo not misread an order. It also promotesaccurate dose calculation by facilitatingredundant checks by nurses and pharmacists.
8. If the order is for a drug product that is not onformulary or for a new dosage of a formularymedication, the prescriber should provideinformation with the order or in the patient’schart for other healthcare professionals. Useof a non-formulary medication introduces anew drug into the system that healthcare pro-fessionals may not recognize; thereby,increasing the risk of error. A healthcareprovider may assume that it is another drugthat sounds, or looks similar to an agent withwhich they are familiar. Use of non-formula-ry items should be limited for the above rea-sons.
9. If doses are changed for an ambulatorypatient, new prescriptions should be writtenand remaining refills of previous dosesshould be canceled. This information should

439
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
be communicated to the pharmacy providingoutpatient services.In situations where the use of verbal pre-
scriptions or orders is necessary, the prescribershould dictate the order slowly and clearly,spelling the drug name and any other words thatmay be misheard. Likewise, the prescribershould restate numbers that may be confused(i.e., 15 as “one five”). In order to verify accuracy,the prescriber should have the recipient repeatthe order back to him or her. The prescribershould also be certain to verify the transcribedorder within a designated time frame.36
When possible, without compromisingpatient care, odd dosages should be rounded-offfor more convenient and accurate measurement.When appropriate, prescribers should writeorders for commercially available drug products,rather than dosage forms prepared by manipula-tion of commercially available products. If at allpossible, drugs should be prescribed for oraladministration, rather than by injection.Prescribers should consider consolidating stylesof managing patients. A variety of ways of man-aging a patient’s medical condition are possibleand are considered good medicine that is costeffective. However, diversity in writing medica-tion orders may lead to confusion and errors.Consolidating styles in an intensive care unit set-ting so that all drips are written as eithermcg/kg/minute or mg/kg/hour can avoid cal-culation errors that occur secondary to movingback and forth between systems.
The prescriber should also counsel thepatient and his or her caregiver, familiarizingthem with the name, indication, route of adminis-tration, dose, dose frequency, potential adverseeffects, and how adverse effects might be man-aged for each medication the patient is receiving.
Recommendations for Pharmacists
Because of their specialized knowledge ofmedications and their role in the drug distribu-tion process, pharmacists are in a unique positionto prevent medication errors and ensure appro-priate medication use. Pharmacists should inter-act with other members of the healthcare team todevelop, implement, and monitor a therapeutic
plan to achieve optimal care for each individualpatient, making efforts to detect and resolvedrug-related problems before they reach thepatient. Pharmacists must also pay close attentionto their portion of the drug distribution process,carefully reviewing prescriptions and preparingand dispensing medications, while serving as thedrug information specialist. Suggestions thatmay assist pharmacists in preventing medicationerrors while fulfilling these responsibilities arefound in Table 7.
Prior to patient discharge, the pharmacistand/or nurse should make certain that patientsand/or their caregivers have all the necessarydrug information and knowledge to correctlymeasure and administer doses. It is also impera-tive that they have appropriate equipment forcorrect measurement and administration of theprescribed dose. The patient and/or caregivershould also be asked to demonstrate how theywould prepare and administer doses to verifythat they are prepared to perform these tasks. Ifproblems or difficulties are exposed, furthercounseling and teaching are in order.
Recommendations for Nurses
Nurses are in a position too not only identifyprescribing and dispensing errors, but to preventthese errors from reaching the patient.Medication administration is an important step inmedicinal therapy. There are no additional oppor-tunities to detect potential medication errorsbeyond this step. Nurses are, in fact, the final“gatekeeper” for the hospitalized patient.Therefore, nurses must be especially vigilant toprevent medication errors. The following aresuggested measures nurses can take to preventmedication errors.
1. Review the patient’s medication administra-tion record (MAR) to insure that all ordershave been transcribed correctly, all informa-tion is complete, and there are no therapeuticduplications, allergies, or drug-drug, drug-nutrient or drug-disease interactions. If anyquestions arise, the order should be verifiedagainst the original prescriber order, refer-ences and/or colleagues should be consultedas necessary, and the prescriber should be
440
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
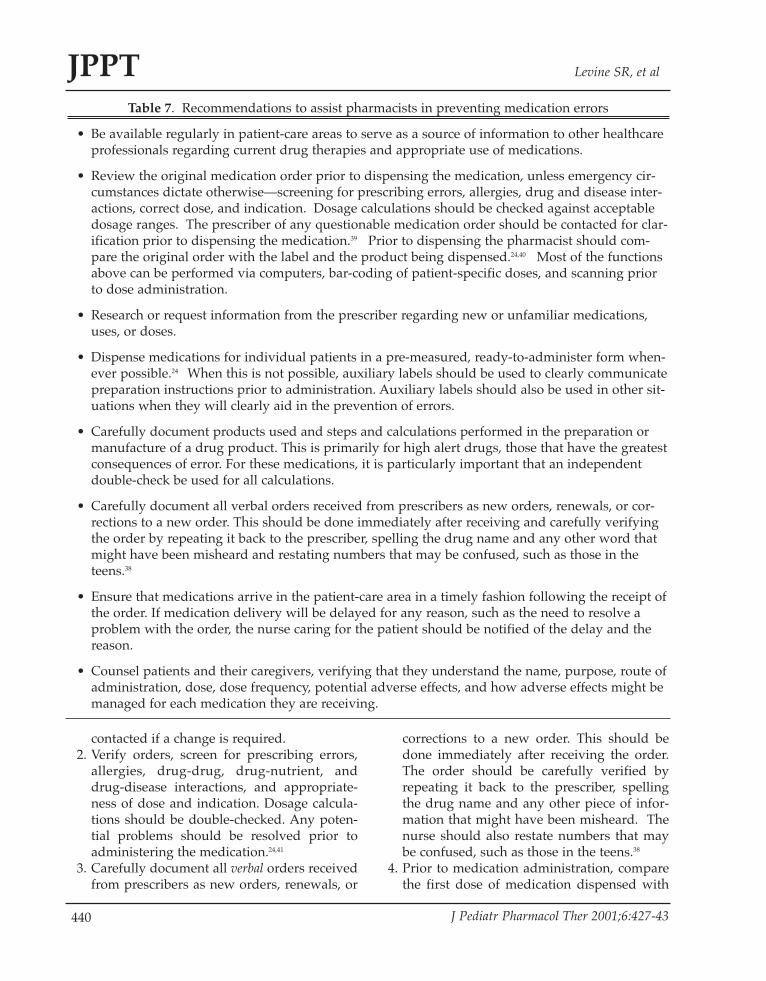
contacted if a change is required.2. Verify orders, screen for prescribing errors,
allergies, drug-drug, drug-nutrient, anddrug-disease interactions, and appropriate-ness of dose and indication. Dosage calcula-tions should be double-checked. Any poten-tial problems should be resolved prior toadministering the medication.24,41
3. Carefully document all verbal orders receivedfrom prescribers as new orders, renewals, or
corrections to a new order. This should bedone immediately after receiving the order.The order should be carefully verified byrepeating it back to the prescriber, spellingthe drug name and any other piece of infor-mation that might have been misheard. Thenurse should also restate numbers that maybe confused, such as those in the teens.38
4. Prior to medication administration, comparethe first dose of medication dispensed with
Table 7. Recommendations to assist pharmacists in preventing medication errors
• Be available regularly in patient-care areas to serve as a source of information to other healthcareprofessionals regarding current drug therapies and appropriate use of medications.
• Review the original medication order prior to dispensing the medication, unless emergency cir-cumstances dictate otherwise—screening for prescribing errors, allergies, drug and disease inter-actions, correct dose, and indication. Dosage calculations should be checked against acceptabledosage ranges. The prescriber of any questionable medication order should be contacted for clar-ification prior to dispensing the medication.39 Prior to dispensing the pharmacist should com-pare the original order with the label and the product being dispensed.24,40 Most of the functionsabove can be performed via computers, bar-coding of patient-specific doses, and scanning priorto dose administration.
• Research or request information from the prescriber regarding new or unfamiliar medications,uses, or doses.
• Dispense medications for individual patients in a pre-measured, ready-to-administer form when-ever possible.24 When this is not possible, auxiliary labels should be used to clearly communicatepreparation instructions prior to administration. Auxiliary labels should also be used in other sit-uations when they will clearly aid in the prevention of errors.
• Carefully document products used and steps and calculations performed in the preparation ormanufacture of a drug product. This is primarily for high alert drugs, those that have the greatestconsequences of error. For these medications, it is particularly important that an independentdouble-check be used for all calculations.
• Carefully document all verbal orders received from prescribers as new orders, renewals, or cor-rections to a new order. This should be done immediately after receiving and carefully verifyingthe order by repeating it back to the prescriber, spelling the drug name and any other word thatmight have been misheard and restating numbers that may be confused, such as those in theteens.38
• Ensure that medications arrive in the patient-care area in a timely fashion following the receipt ofthe order. If medication delivery will be delayed for any reason, such as the need to resolve aproblem with the order, the nurse caring for the patient should be notified of the delay and thereason.
• Counsel patients and their caregivers, verifying that they understand the name, purpose, route ofadministration, dose, dose frequency, potential adverse effects, and how adverse effects might bemanaged for each medication they are receiving.

441
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
the original prescriber order and the medica-tion administration record (MAR). The nurseshould confirm that the correct medication,dose, and dosage form have been provided.Obviously, any concerns (e.g., the need formultiple dosage units to obtain a single dose;inappropriate dosage form or volume for theindividual patient) should be addressed priorto administration of the drug. Subsequent tothis dose, medications should be verifiedagainst the MAR. Transcribed MARs forfuture doses must be verified with the oldMAR to assure accurate transcription.Medications should not be removed frompackaging until they are ready for adminis-tration.21
5. Verify patient identity prior to administrationof any medication.21 When appropriate andreasonable, patients or caregivers should betold the name and purpose of each medica-tion when each dose is given. This aids inpatient education and gives the patient anopportunity to become more involved in hisor her care and prevent possible medicationerrors. If the patient questions a medication,the nurse should listen, answer questions,and (if appropriate) verify the order andproduct before administering the medication.
6. Administer all doses at scheduled times,unless the patient is unavailable or there areproblems with the order or medication thatneed to be resolved. Medication administra-tion should be documented as soon as it iscompleted; thereby, recording the actual timethe dose was administered. An electronicmedical administration record (MAR) withscannable bar-coded patient-specific doseswill greatly reduce administration errors.
7. Contact a pharmacist regarding missingdoses, rather than “borrowing” from anotherpatient or stockpiling unused medications.
8. Understand the correct operation of medica-tion-administration devices and be aware ofthe potential for errors that may occur withthe use of these devices (e.g., programmablepumps).
9. Counsel patients and their caregivers, verify-ing that they understand the name, purpose,route of administration, dose, dose frequency,
common adverse effects, and how adverseeffects might be managed for each medica-tion they are receiving. Provide drug infor-mation at discharge and assure understand-ing by the patient/caregiver.
Recommendations for Patients and Caregivers
All caregivers and all but the youngestpatients should be given the opportunity to beinvolved in the patient’s drug therapy. To active-ly participate in their therapy, the patient or care-giver must be informed about every medicationprescribed and administered and must be encour-aged to ask questions and raise concerns. A well-informed patient or caregiver feels less helpless ina situation that they do not control and also pro-vides an extra opportunity to prevent the occur-rence of a medication error. Patient and/or care-giver education should be considered a standardof care and policies should be created to increasethe involvement of these individuals in treat-ment. The following recommendations areoffered to patients and caregivers to assist them inoptimizing their drug therapy and preventingmedication errors (Table 8).10
An important part of patient education is dis-charge counseling. Continuity of care should bestressed. Some ways that this may be accom-plished include:42 1) to ensure availability of simi-lar products and concentrations that were usedduring hospitalized dispense discharge prescrip-tions through an outpatient pharmacy affiliatedwith the institution; and 2) having caregivers filldischarge prescriptions at the outpatient pharma-cy they normally patronize so that errors mightbe discovered and discharge counseling can becustomized to the products and concentrationsdispensed.
CONCLUSIONS
This document makes recommendations forthe prevention of medication errors in pediatricpatients, incorporating the suggestions of health-care professionals involved in the daily treatmentof this patient population. By working togetheras a patient-care team medication error occur-rence can be minimized through education,
442
JPPT Levine SR, et al
J Pediatr Pharmacol Ther 2001;6:427-43
development of effective systems, individualefforts, and by healthcare professionals. Whenerrors do occur, it is important to first minimizethe effect on the patient and then to learn from theerror and improve the system to prevent similaroccurrences in the future.
ACKNOWLEDGEMENTS
We appreciate the participation of YvonneD’Antonio, PharmD, Safe MedicationManagement Fellow at the Institute for SafeMedication Practices and the Center for ProperMedication Use for developing the frameworkused to stimulate discussion at the ASHP confer-ence. We thank Dean Bennett, RPh, and TheresaForbes, PharmD, at the Alfred I. duPont Hospitalfor Children, Wilmington, Delaware, for theirreview and comments of the final guidelines.
REFERENCES
1. Cohen MR, Blanchard N, Frederico F, Magelli M,Lomax C, Greiner G, et al. Draft guidelines forpreventing medication errors in pediatrics. JPediatr Pharm Prac 1998;189-202.
2. Kaushal R, Bates DW, Landrigan C, McKenna KJ,Clapp MD, Federico F, et al. Medication errors andadverse drug events in pediatric inpatients. JAMA2001;285:2114-20.
3. Pediatric Pharmacy Administrative GroupCommittee on Pediatric Pharmacy Practice.Pediatric Pharmacy Practice Guidelines. Am J HospPharm 1991;48:2475-7.
4. Nahata MC. Pediatric drug therapy II—Drugadministration errors. J Clin Pharm Ther1988;13:399-402.
5. McQueen KD, Orma P, Larkin S. Reemergingchildhood diseases. Am Pharm 1995;NS35:43-52
6. Nahata MC. Pediatrics. In: DiPiro JT, Talbert RL,Hayes PE, Yee GC, Matzke GR, Posey LM, eds.Pharmacotherapy: A Pathophysiologic Approach. 2nded. Norwalk: Appleton & Lange;1993;56-63.
7. Wong AF, Cupit GC. Neonatal Therapy. In: Koda-Kimble MA, Young LY, eds. Applied Therapeutics:The Clinical Use of Drugs. 5th ed. Vancouver:Applied Therapeutics, Inc; 1992.78-1-78-3.
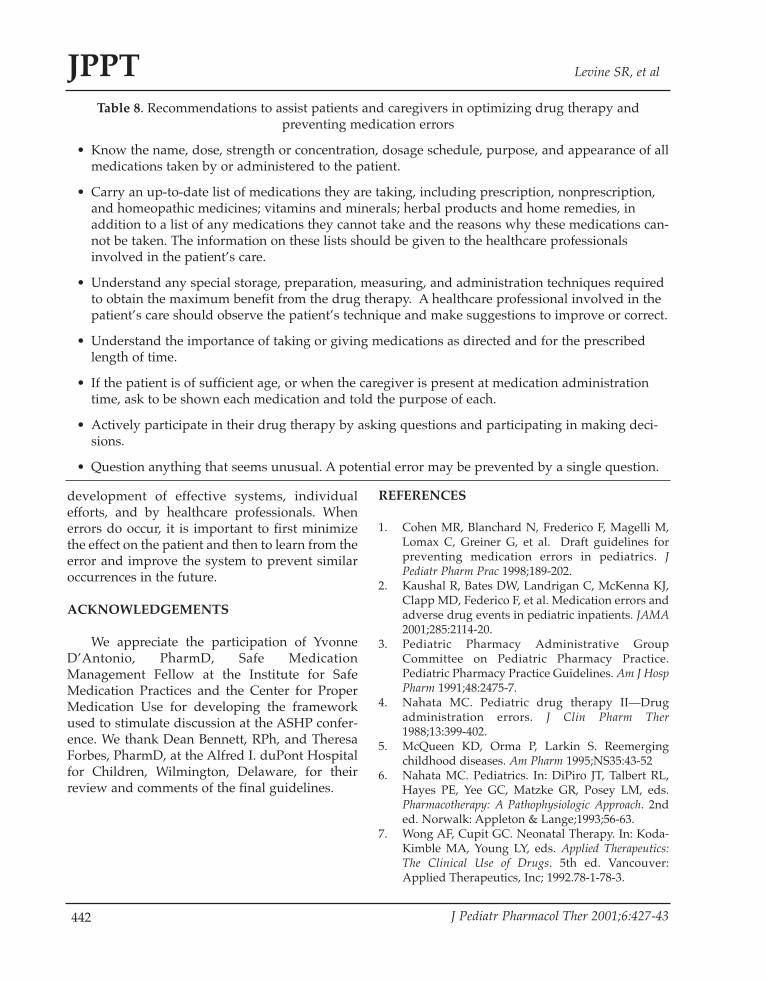
Table 8. Recommendations to assist patients and caregivers in optimizing drug therapy andpreventing medication errors
• Know the name, dose, strength or concentration, dosage schedule, purpose, and appearance of allmedications taken by or administered to the patient.
• Carry an up-to-date list of medications they are taking, including prescription, nonprescription,and homeopathic medicines; vitamins and minerals; herbal products and home remedies, inaddition to a list of any medications they cannot take and the reasons why these medications can-not be taken. The information on these lists should be given to the healthcare professionalsinvolved in the patient’s care.
• Understand any special storage, preparation, measuring, and administration techniques requiredto obtain the maximum benefit from the drug therapy. A healthcare professional involved in thepatient’s care should observe the patient’s technique and make suggestions to improve or correct.
• Understand the importance of taking or giving medications as directed and for the prescribedlength of time.
• If the patient is of sufficient age, or when the caregiver is present at medication administrationtime, ask to be shown each medication and told the purpose of each.
• Actively participate in their drug therapy by asking questions and participating in making deci-sions.
• Question anything that seems unusual. A potential error may be prevented by a single question.
443
Guidelines for preventing medication errors in pediatrics JPPT
J Pediatr Pharmacol Ther 2001;6:427-43
8. Leff RD, Roberts RJ. Problems in drug therapy forpediatric patients. Am J Hosp Pharm 1987;44:865-70.
9. Blanchard NR, Naughton M. Pediatric dosing con-cerns: An opportunity for pharmacists. Hosp PharmTimes 1996(August) 1HPT-3HPT.
10. Gupta A, Waldhauser LK. Adverse drug reactionsfrom birth to early childhood. Pediatr Clin NorthAm 1997;44:79-92.
11. American Society of Hospital Pharmacists. ASHPguidelines on preventing medication errors in hos-pitals. Am J Hosp Pharm 1993;50:305-14.
12. Cohen MR, Anderson RW, Attilio RM, et al.Preventing medication errors in cancer chemother-apy. Am J Health Syst Pharm 1996;53:737-46.
13. Cohen MR. Medication Errors. Principles andTechniques of Safe Medication Use. AmericanPharmaceutical Association. Washington, 1998.
14. Lilley LL, Guanci R. Careful with the zeros! Howto minimize one of the most persistent causes ofgross medication errors. Am J Nurs 1997;97:14.
15. Trinkle R, Wu JK. Errors involving pediatricpatients receiving chemotherapy: a literaturereview. Med Pediatr Oncol 1996;26:344-51.
16. Huddleston K, Creekmore P, Wood B.Administration of infant formula through theintravenous route: consequences and prevention.MCN American J Matern Child Nurs 1994;19:40-2.
17. Roberts RJ. Issues and problems associated withdrug delivery in pediatric patients. J ClinPharmacol 1994;34:723-4.
18. Bayne T, Bindler R. Medication calculation skills ofregistered nurses. J Contin Educ Nurs 1988;19:258-62.
19. Koren G, Barzilay Z, Greenwald M. Tenfold errorsin administration of drug doses: a neglected iatro-genic disease in pediatrics. Pediatrics 1986;77:848-9.
20. Koren G, Haslam RH. Pediatric medication errors:predicting and preventing tenfold disasters. J ClinPharmacol 1994;34:1043-5.
21. Thigpen J. Minimizing medication errors. NeonatalNetw 1995;14;2:85-6.
22. Folli HL, Poole RL, Benitz WE, Russo JC.Medication error prevention by clinical pharma-cists in two children’s hospitals. Pediatrics1987;79:718-22.
23. Kennedy D. Medication “safety checks” in pedi-atric acute care. J Intraven Nurs 1996;19:295-302.
24. Johnson KB, Butta JK, Donohue PK, Glenn DJ,Holtzman NA. Discharging patients with prescrip-tions instead of medications: sequelae in a teach-ing hospital. Pediatrics 1996;97:481-5.
25. Hard R. Pharmacists work on pediatric dosageproblems. Hospitals 1992;66;46,48.
26. Potts MJ, Phelan KW. Deficiencies in calculation
and applied mathematics skills in pediatricsamong primary care interns. Arch Pediatr AdolescMed 1996;150:748-52.
27. Hazinski MF. Reducing calculation errors in drugdosages: the pediatric critical information sheet.Pediatr Nurs 1986;12:138-40.
28. Rosati JR, Nahata MC. Drug administration errorsin pediatric patients. QRB Qual Rev Bull1983;9:212-3.
29. Perlstein PH, Callison C, White M, Barnes B,Edwards NK. Errors in drug computations duringnewborn intensive care. Am J Dis Child1979;133:376-9.
30. Walson PD, Hammel M, Martin R. Prescriptionwriting by pediatric house officers. J Med Educ1981;56:423-8.
31. McMahon SR, Rimsza ME, Bay RC. Parents candose liquid medication accurately. Pediatrics1997;100:330-3.
32. Chater RW. Pediatric dosing: tips for tots. AmPharm 1993;NS33:55-6.
33. Senst B, Achusim LE, Genest RP, Cosention LA,Ford CC, Little JA, et al. Practical approach todetermining costs and frequency of adverse drugevents in a healthcare network. Am J Health SystPharm 2001;58:1126-32.
34. Spielberg SP. Pediatric therapy for the new millen-nium. J Pediatr Pharmacol Ther 2001;6:6-9.
35. Simon HK, Weinkle DA. Over-the-counter medica-tions. Do parents give what they intend to give?Arch Pediatr Adolesc Med 1997;151:654-6.
36. Litovitz T. Implication of dispensing cups in dos-ing errors and pediatric poisonings: a report fromthe American Association of Poison ControlCenters. Ann Pharmacother1992;26:917-8.
37. Fox GN. Minimizing prescribing errors in infantsand children. Am Fam Physician 1996;53:1319-25.
38. West DW, Levine S, Magram G, et al. Pediatricmedication order error rates related to the mode oforder transmission. Arch Pediatr Adolesc Med1994;148:1322-6.
39. Grinder DE, Massanari M. Verifying appropriate-ness of dosages prescribed in a pediatric hospital.Am J Hosp Pharm 1992;49:2778-9
40. Rupp MT, DeYoung M, Schondelmeyer SW.Prescribing problems and pharmacist interven-tions in community practice. Med Care 1992;30:926-40.
41. Greve P. The smaller the patient, the bigger therisk. RN 1990;53:77-80.
42. Davis NM. A well-informed patient is a valuableasset. Am J Nurs 1994;94:16.