Embed Size (px)
DESCRIPTION
A case by case presentation of Gout cases. For Health care professionals but all welcome.
Citation preview

Dr. Ronan KavanaghDr. Ronan KavanaghConsultant RheumatologistConsultant Rheumatologist
Galway ClinicGalway Clinic

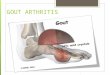
Severe pain big toe 3 days
Just returned from golfing trip Thailand
PMHx: Hypertension
Thiazide diuretic
A Medical Colleague in
his 50’s

InvestigationsWCC 13ESR 50, CRP 60Uric acid 325 (normal)
InvestigationsWCC 13ESR 50, CRP 60Uric acid 325 (normal)

Uric acid levels normal in 30-50% acute attacks
Uric acid levels normal in 30-50% acute attacks
What about the normal uric acid?
What about the normal uric acid?

IF URIC ACID NORMAL, REPEAT 2 WEEKS AFTER AN
ATTACK
IF URIC ACID NORMAL, REPEAT 2 WEEKS AFTER AN
ATTACK

What about this?

Treatment?

Treatment of Acute Gout
Treat early
Encourage oral intake fluids
Full dose NSAID
Prednisolone 30-40mg til attack settles then rapid taper
Colchicine: 1mg stat and 500mcg 6hrly til settles

9
Joint aspiration and injection
QuickTime™ and aH.264 decompressor
are needed to see this picture.
It is possible to find crystals in asymptomatic joints between attacks

Diagnosis
Uric acid may be normal (check after 2
weeks)
Don’t treat hyperuricaemia
Aspirate joints for definitive diagnosis
Can aspirate joint after event

Any other tests?

Renal function
Weight measurement
Don’t forget the BP!
Fasting lipids
• (Hypertriglyceridaemia)
Fasting glucose / dipstick urine
Uric acid excretion?

6 weeks later6 weeks later• The patient returns and reports four
additional acute gouty attacks that responded to colchicine
• On Allopurinol 300mg once daily
• ‘Worse’ since starting
• BP is 130/80 with lisinopril.
• The patient returns and reports four additional acute gouty attacks that responded to colchicine
• On Allopurinol 300mg once daily
• ‘Worse’ since starting
• BP is 130/80 with lisinopril.

COMMON REASONS FOR LACK RESPONSE
Starting Allopurinol during an attack
No prophylaxis
Stopping allopurinol during an attack
Dose of allopurinol too low

URIC ACID 390 (NORMAL RANGE <
430)

TARGET URIC ACID
EULAR suggest < 360 umol/l1
British Society for Rheumatology < 300 umol/l2
(‘normal’ lab range <430)

17

18
Allopurinol

MEDICAL MANAGEMENT OF CHRONIC GOUT
MEDICAL MANAGEMENT OF CHRONIC GOUT
Start allopurinol gently (ideally not during acute attack)
100mg od after a week to 300mg od
Co-prescribe prophylaxis for 1st 6 weeks
Colchicine 500mcg odLow dose NSAID (avoid in this patient)Low dose steroids (Pred 5-7.5mg daily)
Check Urate after a month

Most require 300MG – 500mgMost require 300MG – 500mg
Doses of up to 800MG may be requiredDoses of up to 800MG may be required
Increase monthly dose depending on uric acid Increase monthly dose depending on uric acid levelslevels
Typically 100MG – 300MG – 500MG – 600MG – Typically 100MG – 300MG – 500MG – 600MG – 800MG800MG
Keep uric acid < 300Keep uric acid < 300
ALLOPURINOL

Allopurinol sensitivityRare
Severe reactions < 0.1%
More common in patients with renal impairment*
More common higher doses
Skin rashes 3%
Mild LFT abn.
Stop if rash occurs
Avoid with Azathioprine and mercaptopurine*Arthritis Rheumatism 2009, S60; 761

Treatment adherence rates after 1 year
Pharmacotherapy. 2008;28(4):437-443

What about alcohol?
Alcohol reduces renal urate excretion
Increasing hepatic production of uric acid
Dehydration and acidosis
Reduces metabolism of allopurinol to active metabolite
Beer contains guanosine which is converted to urate
Alcohol reduces renal urate excretion
Increasing hepatic production of uric acid
Dehydration and acidosis
Reduces metabolism of allopurinol to active metabolite
Beer contains guanosine which is converted to urate

24
I suppose I’ll have to give up the drink then?
O.R. = 2.5 O.R. = 1
O.R. = 1.6
Choi HK et al. Lancet 2004; 363: 1277–81
x2 x2
x2

25

26
I might as well drink wine.......
O.R. = 2.5 O.R. = 1O.R. = 1.85
X2 X2X2

Advise to drinkers
•Don’t drink to excess if your father had gout
•If you drink to excess don’t forget to eat
•If you do eat, rethink your diet
•If you are on allopurinol watch yoour urate when you drink!

28

29
Low purine diets

30
What about diet?
Dietary trends increasing prevalence of Gout Associated with Obesity and Insulin resistance
Low purine diet Unpalatable Small reduction uric acid (max 10%)
Current diet focus on: Wt management Moderation of meat and seafood Restriction non complex carbohydrates

31
Diet continued
Regular intake of low fat dairy products reduces attacks
Drinking 5-8 glasses water in 24hrs before attack reduces attacks by 40%
Not as important if gout well controlled with meds

32
A word about tophi

33

34

35

Gout and renal impairment
Uric acid 640
Creatinine 150
eGFR = 30mls/min
47% of patients with gout in general practice have eGFR < 60 mls /min

Gout in renal failureNeed to reduce dose of Allopurinol in renal
failure
Reduced dose means reduced efficacy
Risk of Allopurinol toxicity higher in pts with renal failure (still rare)

38

Asymptomatic hyperuricaemia

Do we need to treat hyperuricaemia?
Strongest risk factor for gout but
0.5% yearly inc. if uric acid 420-530 μmol/l
4.5% if uric acid > 540 μmol/l
Double risk of uric acid renal stones
Renal damage?
Hypertension?
Cerebrovascular disease?

41
“Evidence does not yet support the general treatment of asymptomatic hyperuricaemia to reduce cardiovascular risk”
NEJM 2008;359:11811-21

Alternatives to allopurinol
Probenecid 250mg bd increasing to 1g tds
Less effective if renal impairment
Losartan
Fenofibrate (Lipantil)
Vitamin C

Uricase


45

46

47

48

49

50

Take home pointsUric acid may be normal (check after 2 weeks)
Check Uric acid after a month on treatment
Aim for Urate < 300 with treatment
Many patients need more than 300mg allopurinol
Don’t start Allopurinol during an attack
Don’t stop Allopurinol during an attack
Co-prescribe NSAID / low dose colchicine for 1st 6 weeks
Look for metabolic syndrome

Take home points
Consider reducing dose allopurinol in renal impairment
Consider Febuxostat in allopurinol sensitivity
80mg starting dose increasing to 120mg if necessary

QuickTime™ and aH.264 decompressor
are needed to see this picture.
QuickTime™ and a decompressor
are needed to see this picture.
QuickTime™ and aH.264 decompressor
are needed to see this picture.
Musicians clinic

‘‘Keeping the show Keeping the show on the road’on the road’
Musicians Health Musicians Health ConferenceConference
20122012
‘‘Keeping the show Keeping the show on the road’on the road’
Musicians Health Musicians Health ConferenceConference
20122012

Saturday October Saturday October 13th 201213th 2012
Radisson Hotel Radisson Hotel GalwayGalway

Cheers