Embed Size (px)
DESCRIPTION
present strategy in INDIA for Measles elimination
Citation preview

Presented By: Dr.Preetam Kumar Kar
Facilitators: Dr.Dipanweeta RoutrayDr.Manoj Kumar Dash
Department of COMMUNITY MEDICINES.C.B MEDICAL COLLEGE AND HOSPITAL
CUTTACK.

LAYOUT OF PRESENTATION
Introduction
Background
Vision & Goals of Global Measles elimination Strategic Plan 2012
Guiding Principles to Eliminate Measles
Strategy to Eliminate Measles
Initiatives in India
Challenges in Implementing the Strategic Plan
Conclusion
Bibliography
2

3

Background of measles Elimination
4

GLOBAL SCENARIO
Measles is endemic virtually in all parts of the world.
In 2000: 5.35 lakh children died of measles, themajority in developing countries (WHO report).
Burden accounted for 5% of all under- five mortality.
Epidemics occur when proportion of susceptible childrenreaches about 40 percent.
5

GLOBAL SCENARIO
All 35 countries in the Americas eliminated measles in 2002.
The Western Pacific Region
European and
Eastern Mediterranean
African
SE Asian countries
6
reduced measles cases between 2009 and 2012 and is now on the verge of measles elimination.
focusses on measles control i.e reduction of measles morbidity and mortality in accordance with the target.

7

Number of estimated measles deaths (in thousands) globally
2000-2010
8
Source: who global measles & rubella strategic plan 11
535.3 528.8 484.3373.8 331.4 227.7384.8
177.9
139.3
137.5130.1

INDIAN SCENARIO
In India 2011- 33,634 cases with 56 deaths.
Leading cause of child deaths.
The national routine measles vaccination coverage is 69% (DLHS-3).
Draft Comprehensive Multi Year Strategic Plan (2010-17) for immunisation of India the country with an objective of reducing measles related mortality by 90% by 2013 compared to 2000.
9

10

MEASLES AS AN ELIMINABLE DISEASE
1. Humans are the only reservoir for measles virus.
2. Accurate diagnostic tests for measles.
3. Effective interventions.
4. Life long immunity.
5. Sustained interruption of measles virus transmission.
11

12

VISION
Achieve and maintain a world without measles .
GOALS
A. By end 2015 Reduce global measles mortality by at least 95%
compared with 2000 estimates. Achieve regional measles elimination goals.
B. By end 2020 Achieve measles elimination in atleast five WHO regions.
13

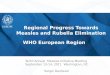
Regional Measles & Rubella Elimination Goals
WHO world map of regional goals for the elimination of measles and either the elimination or control of rubella
14

WHO defines elimination of measles as absence of
endemic measles for a period of >=12 months in
presence of adequate surveillance.
One indicator of measles elimination is a sustained
measles incidence of <1/10 lakh population.
15
DEFINITION

16

1. COUNTRY OWNERSHIP AND
SUSTAINABILITY
National governments and civil society to work
together.
2. ROUTINE IMMUNIZATION AND HEALTH
SYSTEMS STRENGTHENING
Robust and effective health and immunization
systems, particularly a strong national EPI.
3. EQUITY
Specifically target children missed by routine services,
including underserved, migrant and poor children.17

4. LINKAGES
With polio eradication:
Providing polio vaccination during measles SIAs , facilitate
both polio eradication & measles control & elimination.
With other proven child survival interventions:
The routine measles vaccination visit at nine months
is widely used to provide vitamin A supplementation.
18

19

The strategy for 2012–2020 builds on the experiences in the Americas and in countries in other WHO regions that successfully eliminated indigenous transmission of measles.
High coverage with two doses of MCV serves as the foundation required to ensure high population immunity against measles.
20

Component 1. ACHIEVE AND MAINTAIN HIGH LEVELS OF
POPULATION IMMUNITY
Vaccination Coverage >=95% with each of the two doses
of MCV.
Unvaccinated children old enough to receive MCV1 (9 or
12 months).
Strengthening routine immunization - critical component.
Catch up and follow up.
21

Component 2.
MONITOR DISEASE USING EFFECTIVE SURVEILLANCE
AND EVALUATE TO ENSURE PROGRESS
Effective surveillance needed to provide information :
1. To set priorities
2. Plan activities
3. Allocate resources
4. Implement prevention programmes
5. Respond to outbreaks
6. Evaluate control measures
22

Component 3.DEVELOP AND MAINTAIN OUTBREAK
PREPAREDNESS AND RESPOND RAPIDLY TO
OUTBREAKS
In elimination setting :
Single case outbreak rapid investigation
and response.
In emergency setting:
Urgent coordinated SIAs include
Vit. A supplementation prevent outbreaks and
child mortality.
23

Component 4.COMMUNICATE AND ENGAGE TO BUILD
PUBLIC CONFIDENCE
Community awareness regarding
a. Immunization rights
b. Benefits
c. Safety
d. Available services
Will promote public acceptance and participation.
24

Component 5.PERFORM RESEARCH AND DEVELOPMENT
CDC in May 2011 highlighted critical research areas
necessary to achieve measles eradication:
1. Measles epidemiology
2. Assessing vaccine efficacy and effectiveness
3. Needle free vaccine delivery methods
4. Improved methods for laboratory testing for
measles
25

5. New immunization strategies.
6. Improved methods to monitor and evaluate vaccination
programmes.
7. Improved messages and strategies to communicate with
potential beneficiaries and their families.
8. Economic analyses of different strategic options and
mathematical modeling.
26
Component 5.PERFORM RESEARCH AND DEVELOPMENT….contd

27

ACCELERATED MEASLES CONTROL
STRATEGIES
1. Improve and sustain RI coverage (MCV-1).
2. Provide a second opportunity for measles immunization to all
eligible children (MCV-2).
3. Sensitive, laboratory supported measles outbreak surveillance
for case/outbreak confirmation.
4. Fully investigate all detected measles outbreaks and ensure
appropriate case management.
28

LEGEND
2012
2011
Dhenkanal
Ganjam
Jajpur
Kalahandi
Khurda
Koraput
Malkangiri
Nabarangpur
Nayagarh
Rayagada
Bargarh
BolangirBoudh
Sonepur
Sambalpur
Angul
Balasore
Bhadrak
Deogarh
Jharsuguda
Keonjhar
Mayurbhanj
Sundargarh
Jagatsingpur
Kendrapara
Puri
Cuttack
Gajapati
ANDHRA
PRADESH
JHARKHAND
N
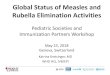
Reported Measles Outbreaks in the years
2011, 12 & 13
Kandhamal
2011, 2012 & 2013
201329Source: SMO , NPSP unit Ganjam

CASE OF CLINICAL MEASLES
Any person in whom clinician suspects measles infection
OR
Any person with fever and maculo papular rash with Cough / Coryza / CONJUNCTIVITIS
OR
A death which occurs within one month of onset of measles
30
For epidemiological investigation, clinical measles would be a case within last 3 months.

CONFIRMATION OF OUTBREAK
By Serology
Positive Measles IgM antibody in any of the 5 blood samples collected during the outbreak and tested in a WHO accredited Laboratory.
(Measles negative samples are tested for Rubella)
31

Desk Review of Measles data every Tuesday at district level
Identify blocks with 5 cases or 1 death in a week
WHICH POTENTIAL OUTBREAKS TO INVESTIGATE?
Any death in a block5 cases in a block
IF YESConduct preliminary field search in area to look for additional cases
Assess if these cases are clustered in same/ adjacent villages
IF ADDITIONAL CASES FOUND (~10 CASES)conduct detailed investigation: HTH search, Serology from 5 cases,
Rx for all cases (Vit A, ORT etc.) 32

PLANNING FOR MEASLES OUTBREAK
INVESTIGATIONSERT
Members: CMO. District Surveillance Officer RCH Officer / DIO Epidemiologist Pediatrician / physician Laboratory Specialist Statistical Officer Surveillance Medical Officer (SMO) others from the district as appropriate (partner
representatives)
The local MO to be co-opted at the time of the outbreak investigation.
33

2. ASSIGNING OUTBREAK NUMBER & PRELIMINARY
SEARCH
Assigning an Outbreak Number
MOB-ST-DIS-YY-NUM
MOB-0R-GJM-14-001
The PHC MO should ensure that the village/ locality of the area is searched for additional cases.
The outcome of the search should be communicated to the RCH Officer.
The RCH Officer/ SMO/IDSP-SO should decide if the outbreak needs to be investigated in detail.
The state should be notified using the VPD-OB001 form
34

3. MOBILIZATION OF THE EPIDEMIC RESPONSE
TEAM
When: As soon as an outbreak is identified.
Why: For detailed outbreak investigation at the outbreak locality.
Who: The CMO of the district convenes a meeting of all members of the ERT.
For: Micro planning the outbreak Investigation.
35

Form VPD-OB003
Village / Area: ________________ PHC:_________________ Block:__________________________ District:__________________________ State:___________________
Outbreak ID: _________________________________ Report sent by:_____________________Date Sent: ____________
Sex
Date of last
measles
vaccine
Date of onset
of rash
If died, date of
death
Date of blood
specimen
collection
M/F Years Months dd/mm/yyyy dd/mm/yyyy dd/mm/yyyy dd/mm/yyyy
Unknown Unknown
Unknown Unknown
Unknown Unknown
Yes
No
Yes Yes
No No
Yes
Setting: Urban / Rural
No
Age
Yes Yes
No No
Patient's name, father's name
and address
Patient
number
Received
measles
vaccine
(circle)
MEASLES OUTBREAK INVESTIGATION: DATA ON CASES
Death
(circle)
36

Steps contd…..
Children suffering from Measles should be given
First dose of Vit A by health worker and informed of second dose.
Supervisor to follow up with second dose
of Vit A.
Manage the existing cases.
Ask the family to report occurrence of new Measles cases to the local health worker/nearest health center immediately.
37

6-7. COLLECTION AND SHIPMENT OF SPECIMENS
TO THE LABORATORY

SPECIMEN COLLECTION & PROCESSING
Co
lle
ct s
eru
m i
n
lab
ele
d s
teri
le v
ials
Cen
trif
uge
Clo
tted
Blo
od
Leave at Room Temp for clot formation (30 mins.)
Centrifuge @ 1500 RPM – 10 Min
Storage

8. DATA ANALYSIS
Defining the outbreak in terms of time, place & person
Age distribution
Proportion of cases vaccinated in different age groups (How is RI performance?)
CFR
Mapping of cases: particular areas or communities of village affected.
Calculation of attack rates and vaccine efficacy if community survey done.

9. REPORT WRITING AND FEEDBACK
Share the experience with programme implementers (form VPD – OB004).
Document for comparison in the future Learning for an evolving programme.
To be sent to state government, IDSP, GoI and NPSP.

Form VPD-OB004
Outbreak ID: _______________________
Notification
Source of notification: Weekly report / Active case search / Media / Other
Index case reported by:______________ Name of DIO:________________________
Designation:____________________ Name of SMO:_______________________
Date of notification of index case: ______________
MEASLES OUTBREAK INVESTIGATION: SUMMARY
Desk review: date________________________ findings________________________________________________________
Date/s of preliminary search:__________________________
Number of health facilities searched: ___________________ Number of sub-centers/ urban wards searched: _________
Number of areas* searched:__________________ Total number of clinical measles cases:__________
Date of Epidemic Response Team meeting: ____________________
Whether considered as an outbreak requiring house to house investigation: Yes / No
If No, reason: No clustering of cases Low case count
Others (specify ) ________________________________________________________________
If Yes, provide details of outbreak investigation below
Preliminary investigation including desk review


10. INITIATING ACTIONS
State level action
Collect data to guide development of policy.
Taking next step in measles control.
District Level action
Prevent death – Vit-A, ORT. Antibiotics, Referral chain.
Ensure availability of vaccines.
Improve routine immunization.
Targeting populations at risk.
Local level actions
Ensuring vaccine is available in all sessions.
Ensure that sessions are not missed.
Ensure coverage is complete in the target population.

45

1. FINANCIAL RISKS
Sufficient predictable and sustainable funds .
2. HIGH POPULATION DENSITY AND HIGHLY
MOBILE POPULATIONS
The highly infectious nature of measles makes
control and elimination very challenging.
3. CONFLICT AND EMERGENCY SETTINGS
Humanitarian crises
46

3. WEAK IMMUNIZATION SYSTEMS AND
INACCURATE REPORTING OF VACCINATION
COVERAGE
High infectiousness & high rate of clinical disease.
Strengthening routine immunization systems.
4. MANAGING PERCEPTIONS AND
MISPERCEPTIONS
When individuals no longer see cases of a
previously common disease they begin to believe
the vaccine no longer provides benefits.
47

CONCLUSION
Improving measles vaccination coverage and reducing measles-related deaths is a global imperative, particularly as it relates to the United Nation’s Millennium Development Goal 4 (MDG4), which aims to reduce the overall number of deaths among children by two-thirds between 1990 and 2015.
We must work together to increase and sustain the socio-political and financial commitments required to end the devastation associated with preventable measles.
48

TAKE HOME MESSAGEReverse the resurgence of measles,achieve the 2015 mortality-reduction target& look beyond, to reap the tremendouslong-term humanitarian and economic benefits associated with a world free of measles.


BIBLIOGRAPHY
1.Levels & trends in child mortality report 2011: Estimates developed by the UN Inter-agency Group for Child Mortality Estimation. New York, NY, United Nations Children’s Fund, 2011 (http://www.childinfo.org/files/Child_Mortality_Report_2011.pdf, accessed 11 March 2012).
2. Wolfson LJ et al. Estimates of measles case fatality ratios: a comprehensive review of community-based studies. International Journal of Epidemiology, 2009, 38:192–205.
3. WHO/UNICEF Global Plan for reducing measles mortality 2006–2010 (http://whqlibdoc.who. int/hq/2005/WHO_IVB_05_11_eng.pdf).
4. Strebel PM et al. A world without measles. Journal of Infectious Diseases, 2011, 203:S1–S3.
5.Park’s textbook of Preventive and Social Medicine 22nd edition.
6.Health Policies and programmes in India.dr. D.K.Taneja..
51