Embed Size (px)
DESCRIPTION
INTRODUCTION TO FUNGAL INFECTIONS, Classification of Fungal Infections (mycoses), Pityriasis versicolor, Tinea nigra, Black piedra, White piedra
Citation preview

https://www.facebook.com/groups/dermatologycourseonline/
• Historically it was thought that fungi were plants that did not need photosynthesis.
• But now fungi are classified in their own kingdom, separate from plants and animals because:
1- The cell walls of plants are made of cellulose whereas the walls of fungal cells are made of chitin
2- Plants require only simple inorganic compounds such as carbon dioxide and water to grow. Fungi require a diet of complex organic molecules to thrive.
• Fungi are parasites or saprophytes i.e. they live off living or dead organic matter.
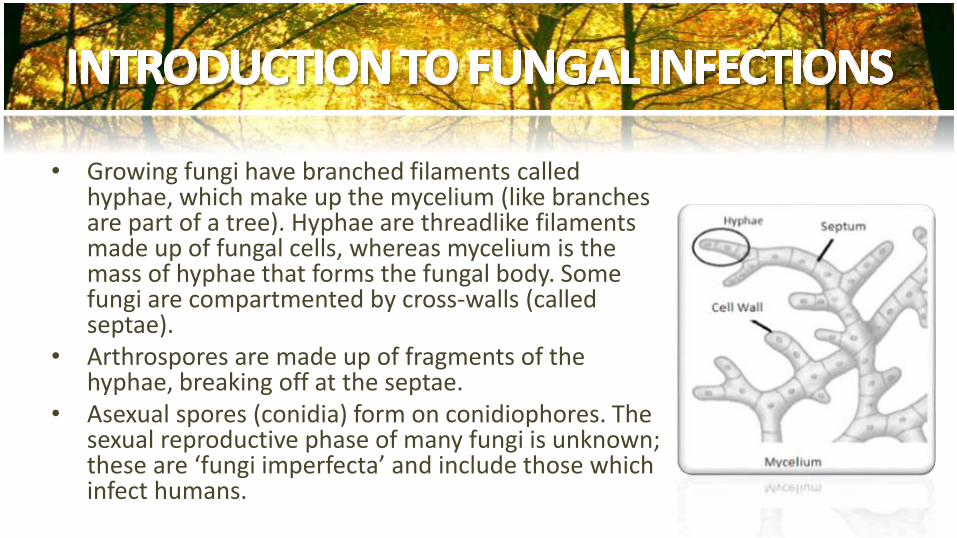
• Growing fungi have branched filaments called hyphae, which make up the mycelium (like branches are part of a tree). Hyphae are threadlike filaments made up of fungal cells, whereas mycelium is the mass of hyphae that forms the fungal body. Some fungi are compartmented by cross-walls (called septae).
• Arthrospores are made up of fragments of the hyphae, breaking off at the septae.
• Asexual spores (conidia) form on conidiophores. The sexual reproductive phase of many fungi is unknown; these are ‘fungi imperfecta’ and include those which infect humans.
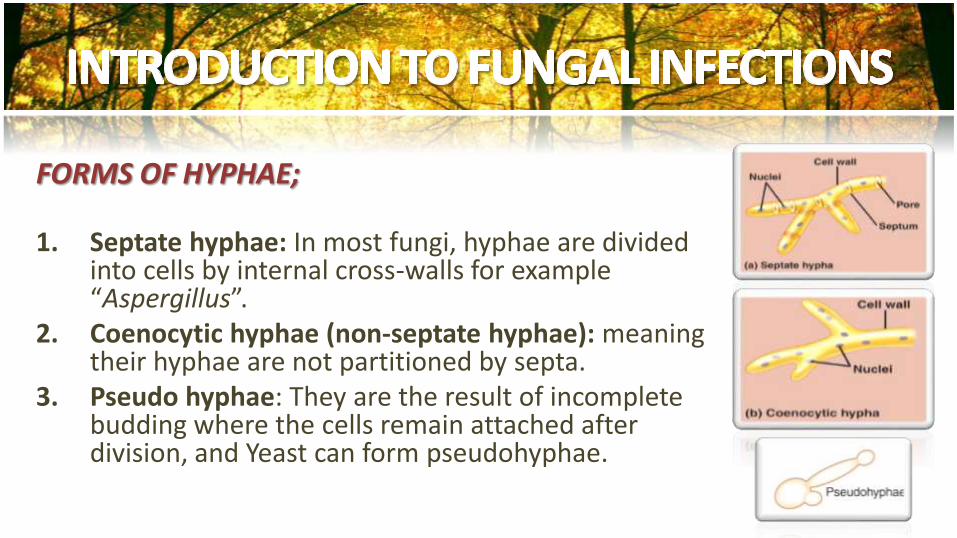
FORMS OF HYPHAE;
1. Septate hyphae: In most fungi, hyphae are divided into cells by internal cross-walls for example “Aspergillus”.
2. Coenocytic hyphae (non-septate hyphae): meaning their hyphae are not partitioned by septa.
3. Pseudo hyphae: They are the result of incomplete budding where the cells remain attached after division, and Yeast can form pseudohyphae.
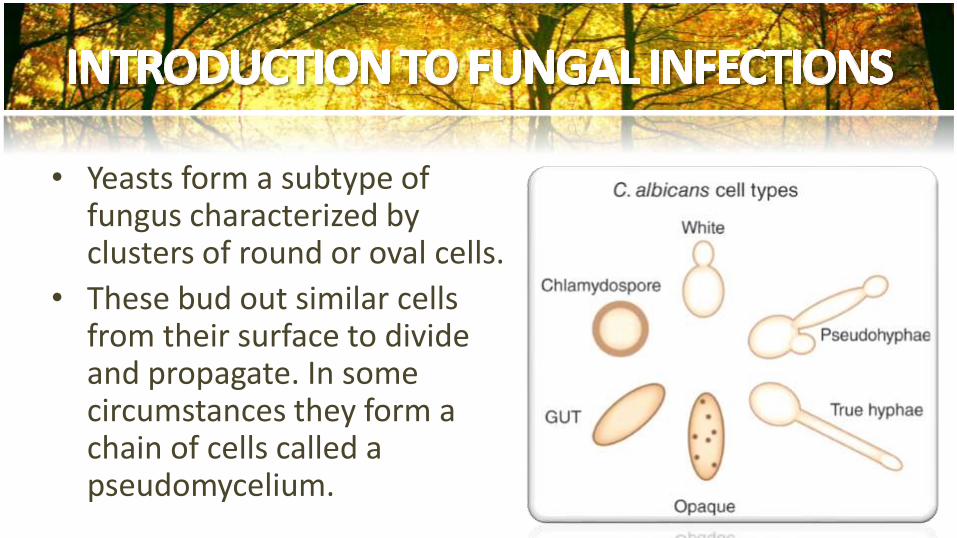
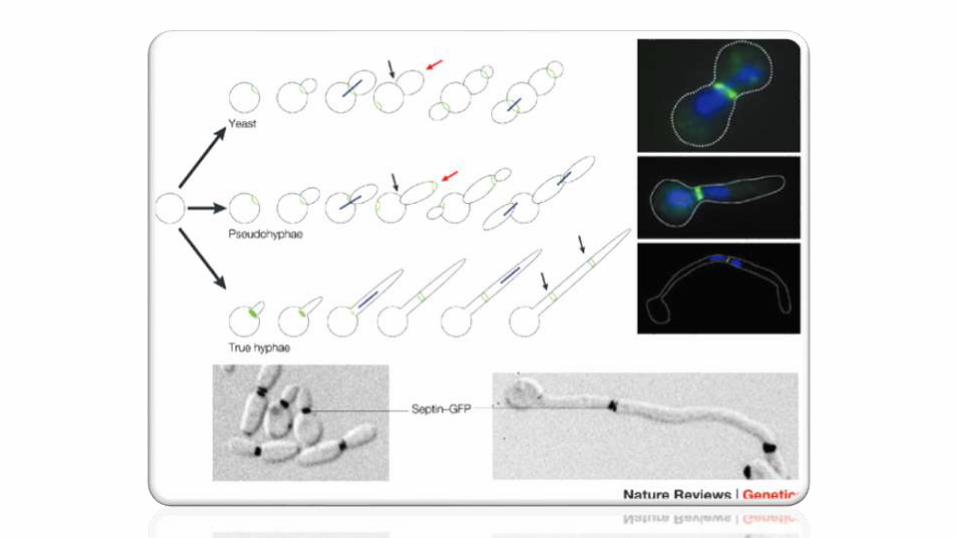
• Yeasts form a subtype of fungus characterized by clusters of round or oval cells.
• These bud out similar cells from their surface to divide and propagate. In some circumstances they form a chain of cells called a pseudomycelium.
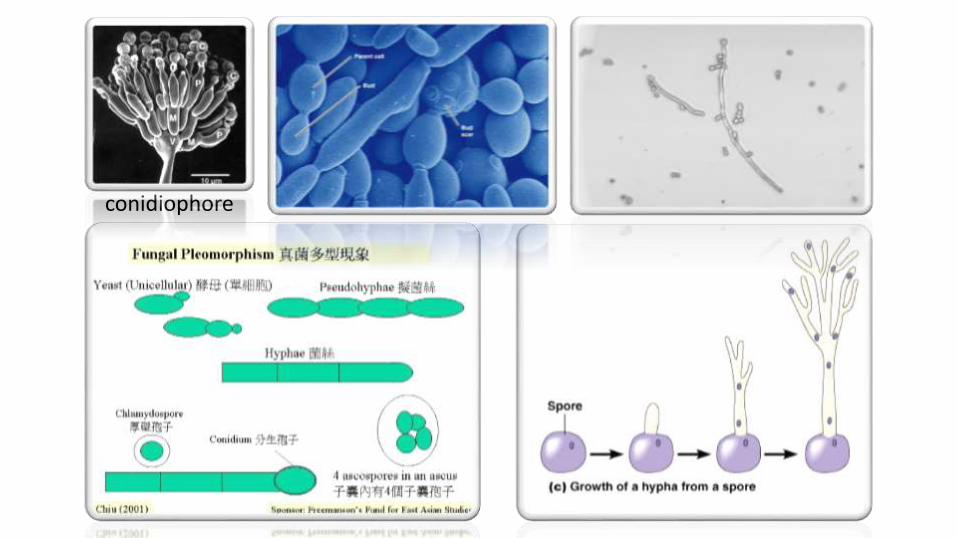
conidiophore
THE ORGANISMS ARE TRANSMITTED BY EITHER;
1. Direct contact with infected host (human or animal).
2. Indirect contact with infected exfoliated skin or hair in combs, hair brushes, clothing, furniture, theatre seats, caps, bed linens, towels, hotel rugs, and locker room floors.
• According to their appearance by microscopy and in culture or method of reproduction.
BY THE METHOD OF REPRODUCTION:
1. Sexual
2. Asexual.
I. SUPERFICIAL MYCOSESa) Non-inflammatory
b) Inflammatory
II. SUBCUTANEOUS MYCOSES
III. SYSTEMIC MYCOSES
Classification of Fungal Infections (mycoses)

• These affect the outer layers of the skin, the nails and hair. • The main groups of fungi causing
superficial fungal infections are: 1. Yeasts
i. Candidaii. Malassezia
2. Dermatophytes (ringworm/tinea) 3. Other Moulds e.g.
i. Aspergillus spp. ii. Fusarium spp.
Infections limited to the outermost layers of the skin and hair:
1. Pityriasis versicolor
2. Candidiasis
3. Tinea nigra
4. Black piedra
5. White piedra
• Infections that extend deeper into the epidermis, as well as hair and nail and caused by dermatophytes.
• They colonize the keratin and inflammation is caused by host response to metabolic by-products:
1. Tinea capitis (head)2. Tinea faciei (face) 3. Tinea barbae (beard) 4. Tinea corporis (body) 5. Tinea manus (hand) 6. Tinea cruris (groin) 7. Tinea pedis (foot) 8. Tinea unguium (nail)
THE MAIN 3 GENERA OF DERMATOPHYTES ARE:
1. Trichophyton (abbreviated as "T")
2. Epidermophyton (“E")
3. Microsporum (“M")
1. Anthropophilic dermatophytes are restricted to human hosts and produce a mild, chronic inflammation e.g.
T. rubrum ▪ M. audouinii T. interdigitale ▪ T. violaceum T. tonsurans ▪ T. schoenleinii
2. Zoophilic organisms are found primarily in animals and cause marked inflammatory reactions in humans who have contact with infected cats, dogs, cattle, horses, birds, or other animals e.g.
M. canis (originating from dogs and cats) T. equinum (originating from horses) T. verrucosum (originating from cattle)
3. Geophilic species are usually recovered from the soil but occasionally infect humans and animals. They cause a marked inflammatory reaction, which limits the spread of the infection and may lead to a spontaneous cure but may also leave scars e.g.
M. gypseum M. fulvum
• These involve the deeper layers of the skin (the dermis, subcutaneous tissue, muscle & fascia and even bone).
• The causative organisms normally live in the soil living on rotting vegetation. They can get pricked into the skin as a result of an injury but usually stay localized at the site of implantation.
• Deeper skin infections include: 1. Mycetoma2. Chromoblastomycosis3. Sporotrichosis
• May result from breathing in the spores of fungi, which normally live in the soil or rotting vegetation or as opportunistic disease in immune compromised individuals.
A. Inhaled fungal infection (By True pathogens)• Although uncommon, some may infect healthy
individuals. The result is most often a mild infection and long lasting resistance to further attack, but occasionally these infections are more serious and chronic (especially in the immune suppressed). The organisms causing systemic fungal infections include:
1. Histoplasmosis2. Coccidioidomycosis (North and South America).
B. Opportunistic infections• Other systemic mycoses only infect those who are already
sick or with an immunodeficiency disorder i.e. they are ‘opportunists’. Repeated infection may occur. Risks for systemic mycoses include: 1. Serious illness and debility 2. Cancer or leukemia
3. Diabetes mellitus 4. Transplant 5. Massive doses of antibiotics 6. Parenteral nutrition 7. Drug addiction 8. Infection with human immunodeficiency virus (HIV)
• Opportunistic fungal infections include: 1. Aspergillosis (found everywhere) 2. Zygomycosis3. Cryptococcosis (where there are pigeon droppings) 4. Trichosporon beigelii5. Pseudallescheria boydii

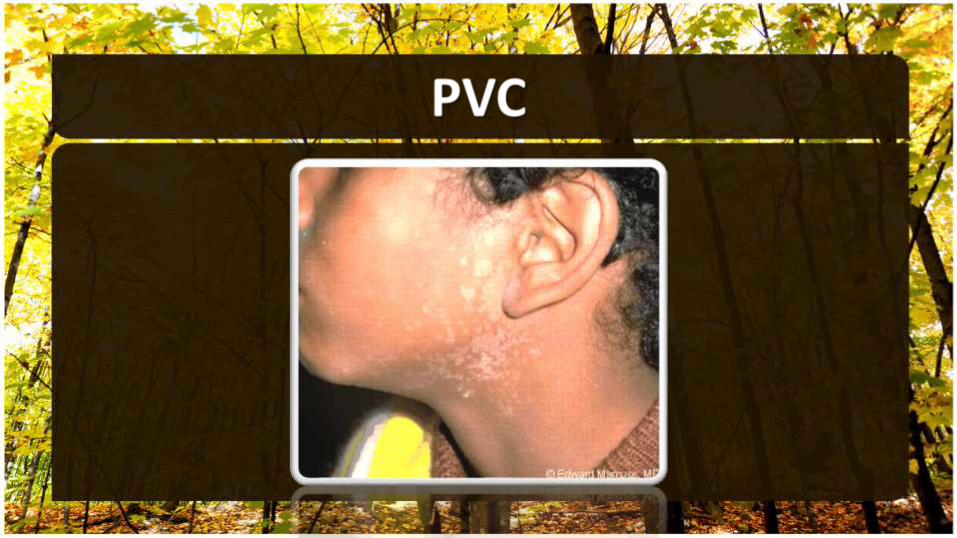
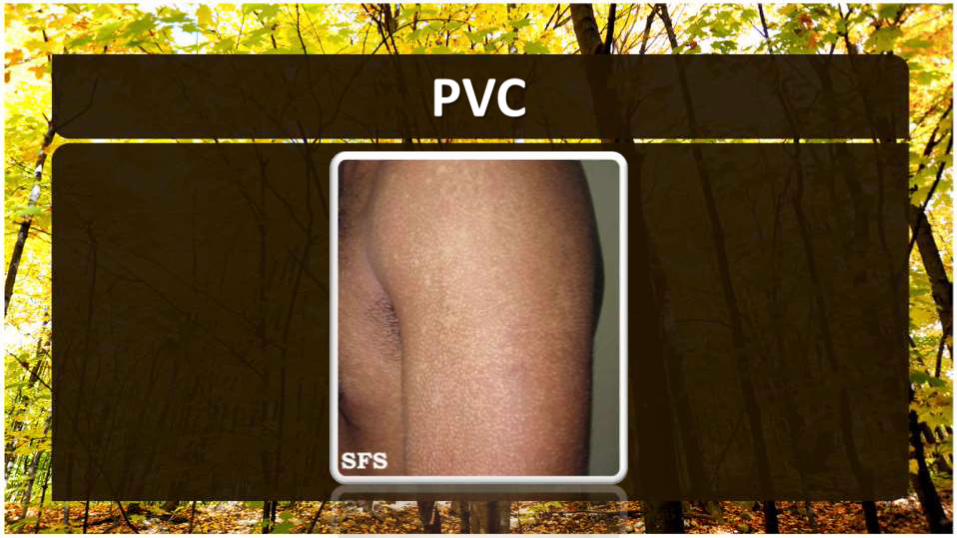
• It is a common, long-term (chronic) superficial fungal infection of the skin.
• Affected skin change color and become either lighter or darker than surrounding skin.
• Common in adolescent and young adult males. Malassezia requires oil to grow, accounting for the increased incidence in adolescents and preference for sebum-rich areas of the skin.
• Its occurrence before puberty or after age 65 years is uncommon.
• A member of normal human cutaneous flora, and it is found in 18% of infants and 90-100% of adults and it is NOT CONTAGIOUS.
• Worldwide distribution but prevalence reported to be as high as 50% in the humid, hot environmentand as low as 1.1% in the colder temperatures.
• The condition is more noticeable during the summer months.
• The causative fungus is Malassezia furfur (previously known asPityrosporon orbiculare and Pityrosporon ovale).
• In patients with clinical disease, the organism is found in both the yeast stage and the filamentous (mycelial/hyphae) form.
• Factors that lead to the conversion to the parasitic, mycelialmorphologic form include;
1. Genetic predisposition2. Oily skin (yeast is lipophilic)3. Excessive sweating4. Warm, humid environments
5. Immuno-suppression6. Malnutrition7. Pregnancy8. Cushing disease
• The reason why this organism causes PVC in some individuals while remains as normal flora in others is notentirely known.
• Several factors, such as the organism's nutritionalrequirements and the host's immune response to the organism, are significant.
• Lymphocyte function on stimulation with the organism has been shown to be impaired in patients who are affected.
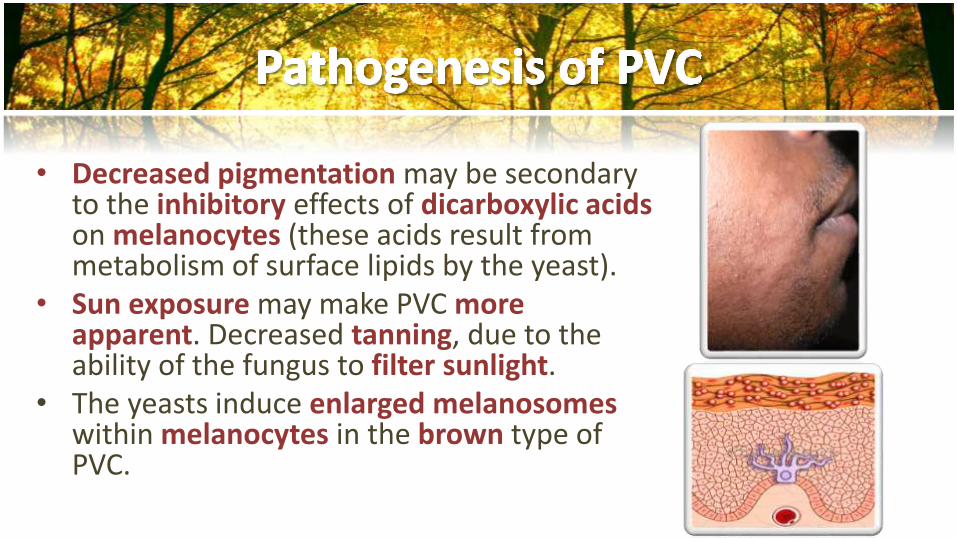
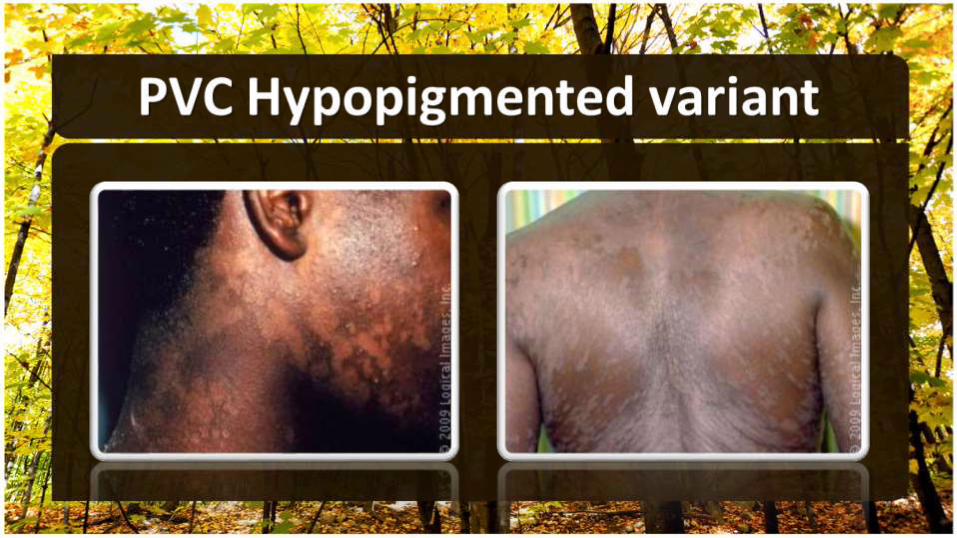
• Decreased pigmentation may be secondary to the inhibitory effects of dicarboxylic acidson melanocytes (these acids result from metabolism of surface lipids by the yeast).
• Sun exposure may make PVC moreapparent. Decreased tanning, due to the ability of the fungus to filter sunlight.
• The yeasts induce enlarged melanosomeswithin melanocytes in the brown type of PVC.
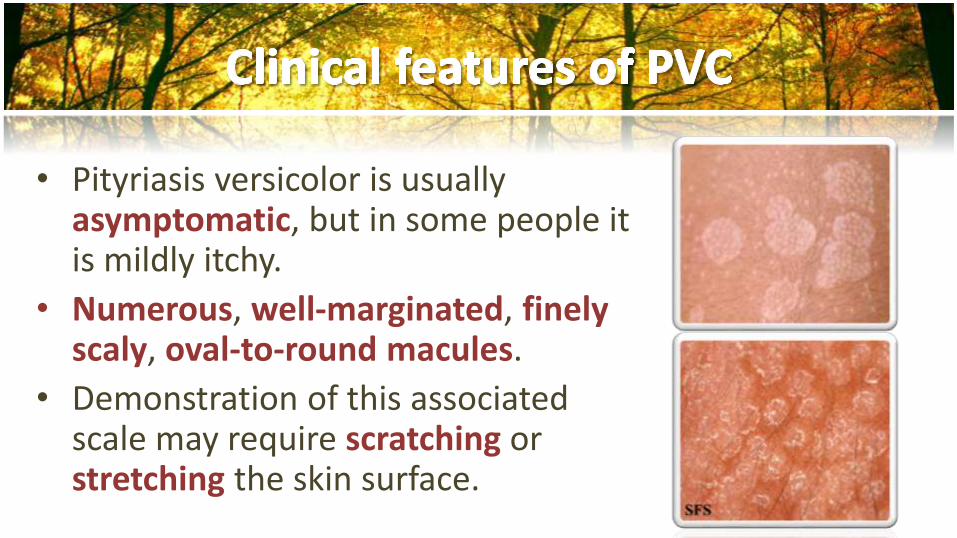
• Pityriasis versicolor is usually asymptomatic, but in some people it is mildly itchy.
• Numerous, well-marginated, finelyscaly, oval-to-round macules.
• Demonstration of this associated scale may require scratching or stretching the skin surface.
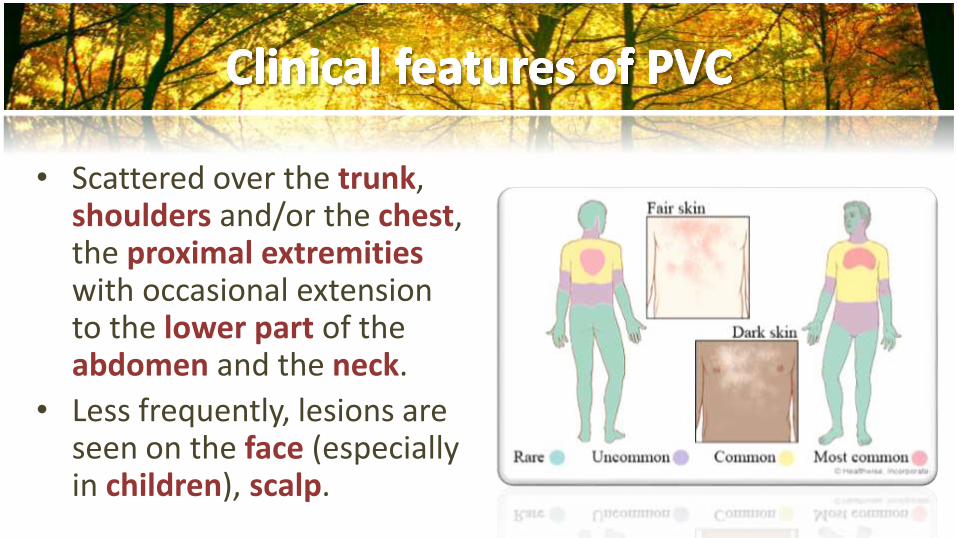
• Scattered over the trunk, shoulders and/or the chest, the proximal extremities with occasional extension to the lower part of the abdomen and the neck.
• Less frequently, lesions are seen on the face (especially in children), scalp.
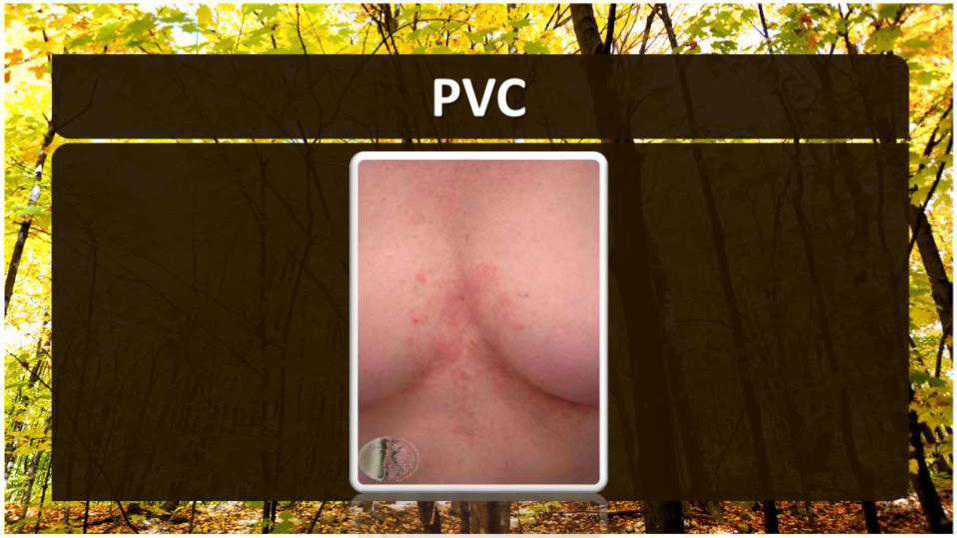


• The macules tend to coalesce, forming large irregularly shaped patches.
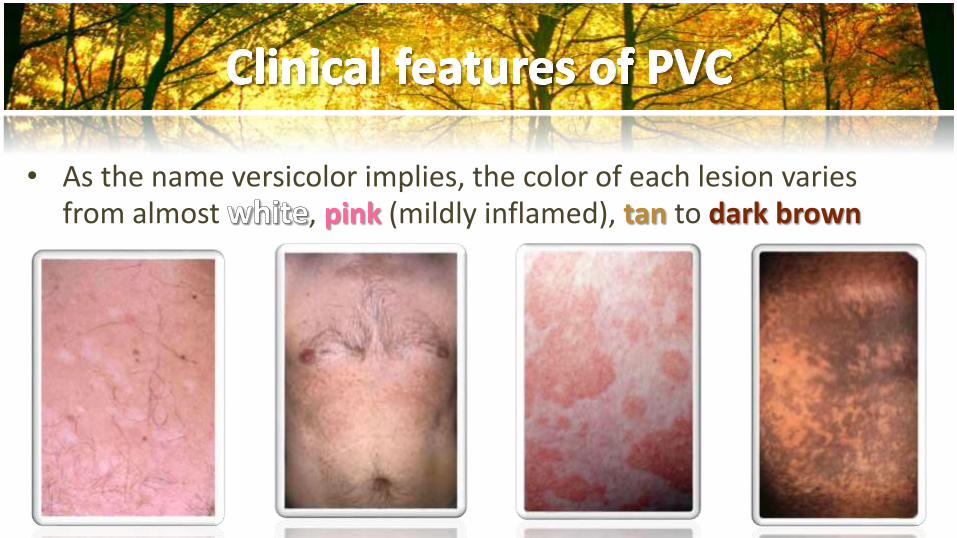
• As the name versicolor implies, the color of each lesion varies from almost , pink (mildly inflamed), tan to dark brown


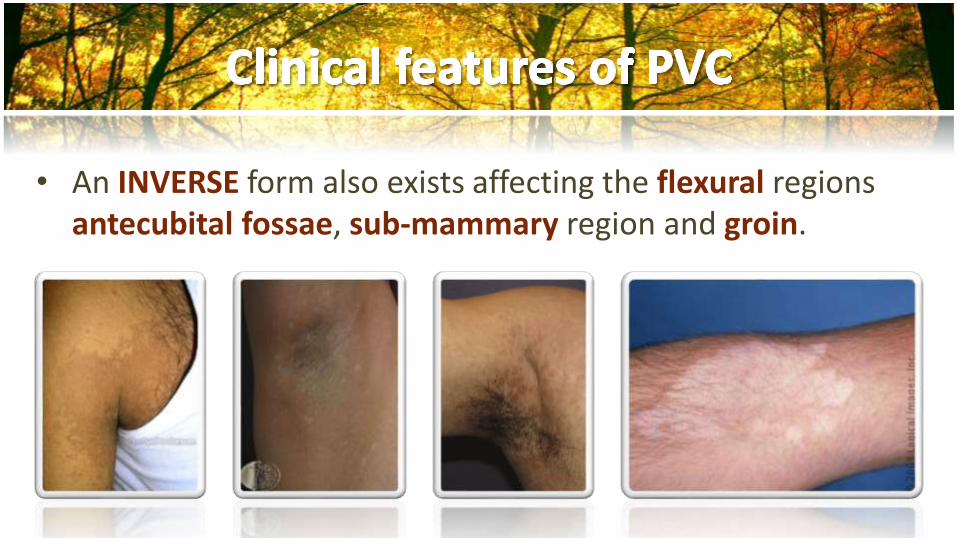
• An INVERSE form also exists affecting the flexural regions antecubital fossae, sub-mammary region and groin.
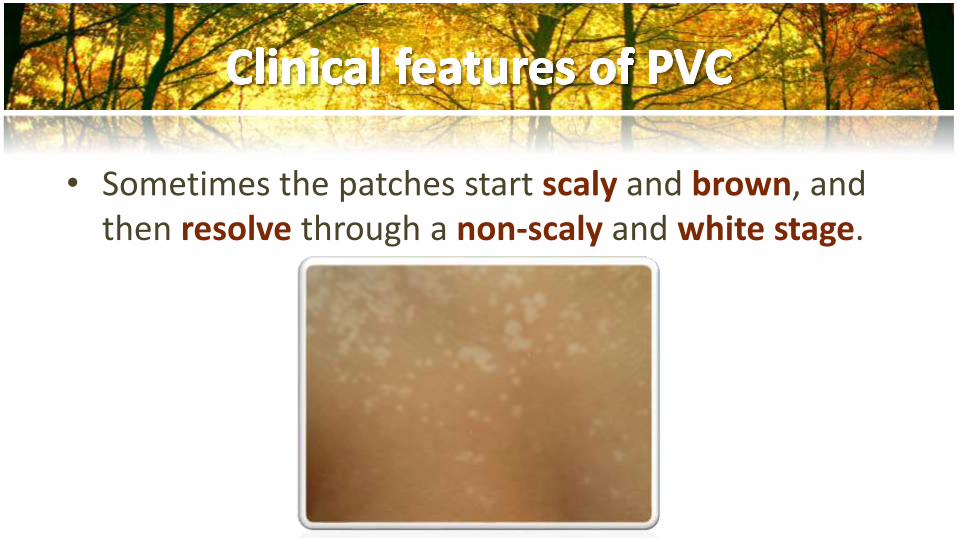
• Sometimes the patches start scaly and brown, and then resolve through a non-scaly and white stage.
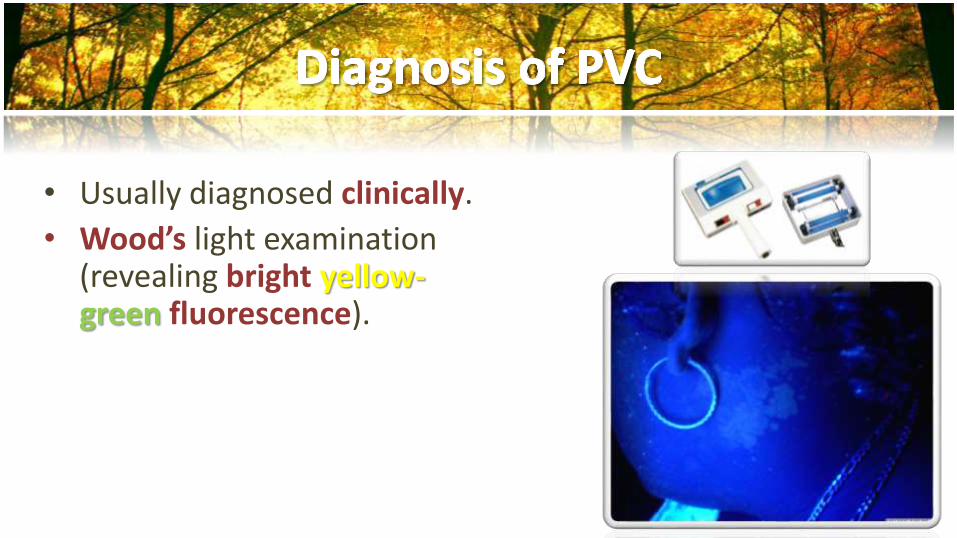
• Usually diagnosed clinically.
• Wood’s light examination (revealing bright yellow-green fluorescence).
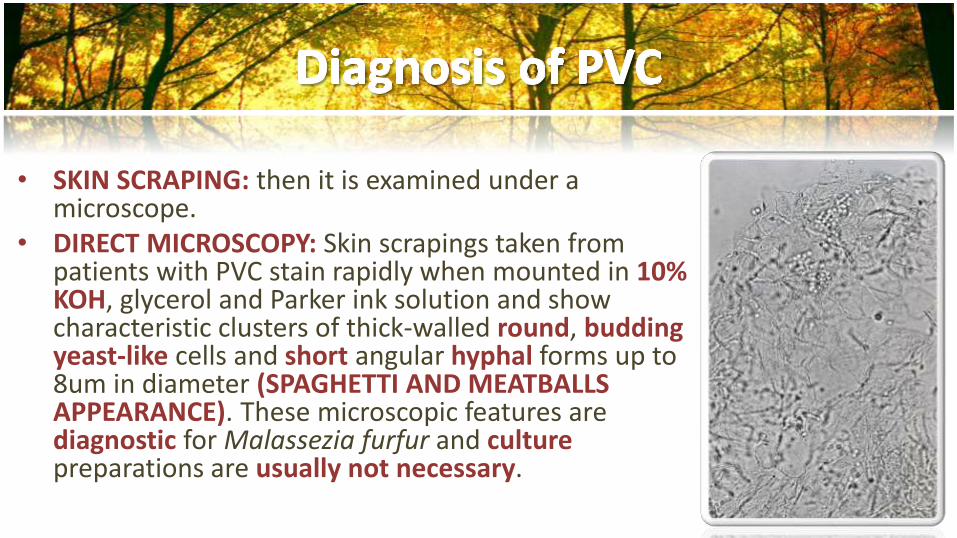
• SKIN SCRAPING: then it is examined under a microscope.
• DIRECT MICROSCOPY: Skin scrapings taken from patients with PVC stain rapidly when mounted in 10% KOH, glycerol and Parker ink solution and show characteristic clusters of thick-walled round, buddingyeast-like cells and short angular hyphal forms up to 8um in diameter (SPAGHETTI AND MEATBALLS APPEARANCE). These microscopic features are diagnostic for Malassezia furfur and culturepreparations are usually not necessary.

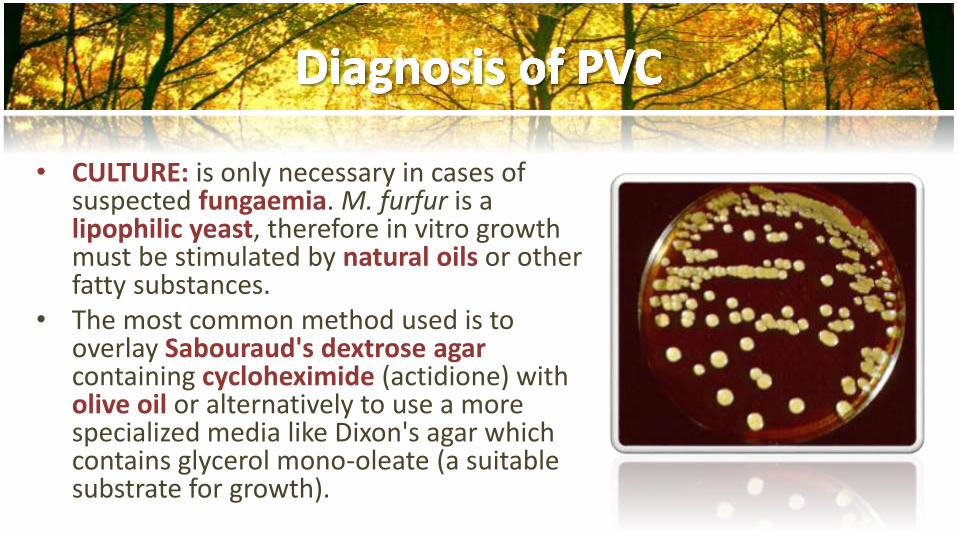
• CULTURE: is only necessary in cases of suspected fungaemia. M. furfur is a lipophilic yeast, therefore in vitro growth must be stimulated by natural oils or other fatty substances.
• The most common method used is to overlay Sabouraud's dextrose agar containing cycloheximide (actidione) with olive oil or alternatively to use a more specialized media like Dixon's agar which contains glycerol mono-oleate (a suitable substrate for growth).
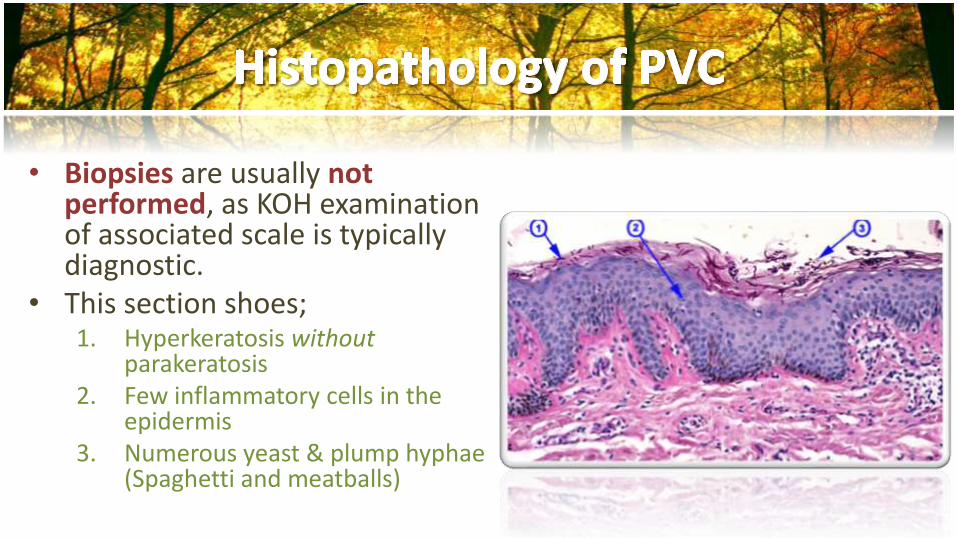
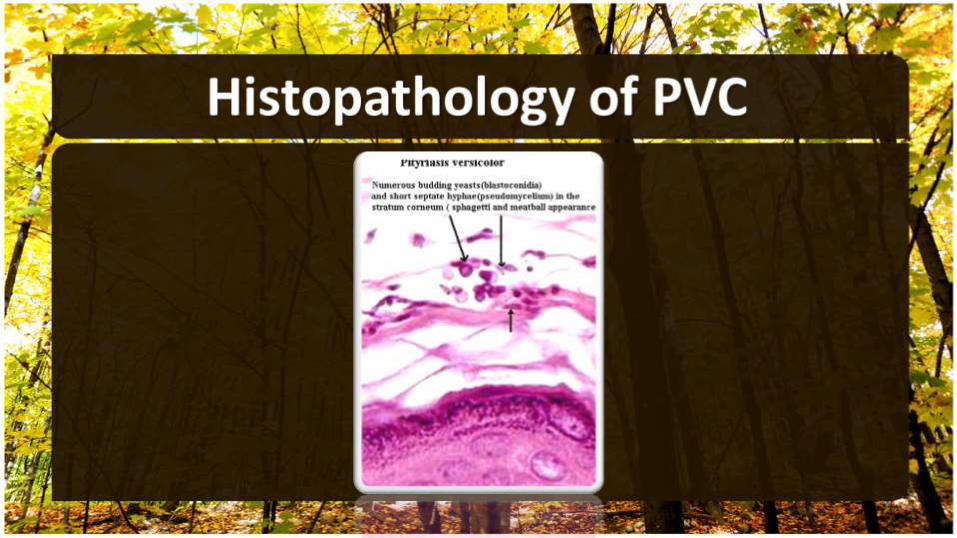
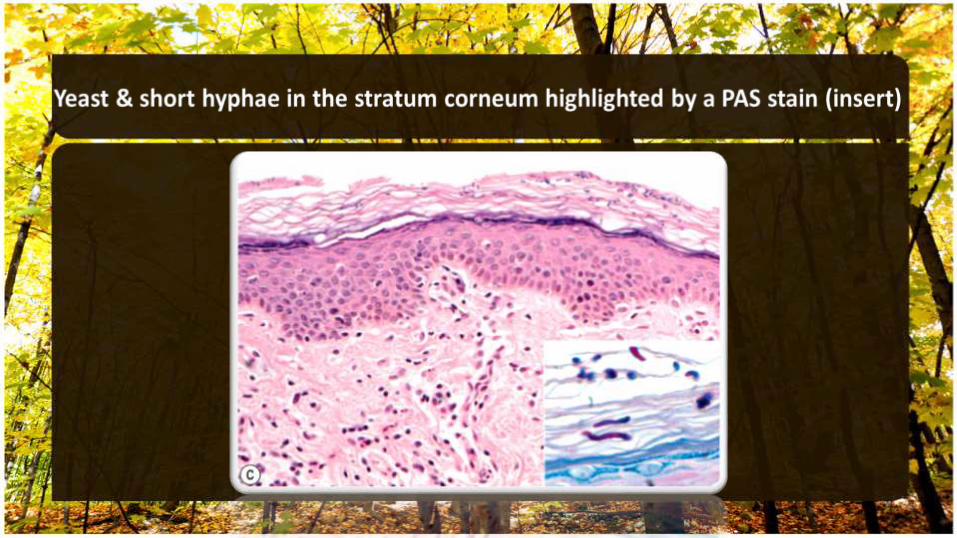
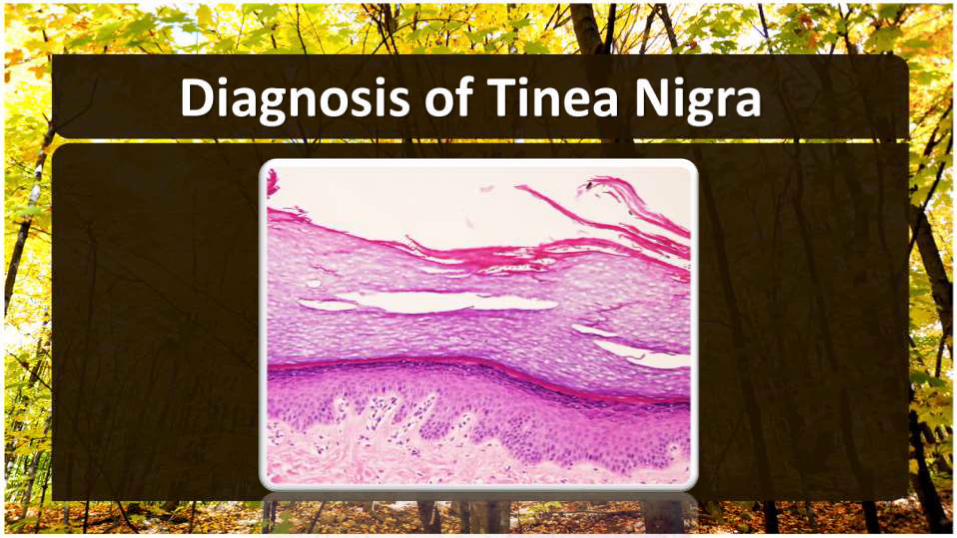
• Biopsies are usually notperformed, as KOH examination of associated scale is typically diagnostic.
• This section shoes;1. Hyperkeratosis without
parakeratosis2. Few inflammatory cells in the
epidermis3. Numerous yeast & plump hyphae
(Spaghetti and meatballs)
1. Pityriasis alba 2. Postinflammatory hypopigmentation3. Vitiligo 4. Seborrheic dermatitis 5. Pityriasis rosea 6. Tinea corporis 7. Secondary syphilis 8. Progressive macular hypomelanosis
TOPICAL TREATMENT 1. Azole creams and lotions; Clotrimazole,
Ketoconazole, Miconazole2. Dandruff shampoos Ketoconazole (1% or 2%) or
2.5% selenium sulfide twice weekly for 2 to 4 weeks; the preparation is left on the skin for 10–15 minutes before rinsing. Over-the-counter dandruff shampoo contain heavy metals e.g. Zinc, Mercury, Copper e.t.c. inhibition of growth of any fungi by reacting in their biosynthetic pathways. Treatment of all the skin from the neck down to the knees, even if only a small area is clinically involved.
3. Allylamine4. Nystatin5. Salicylic acid6. Sodium thiosulphate solution 7. Ciclopirox cream/solution8. 50% propylene glycol in water
SYSTEMIC TREATMENT • If the rash is extensive, oral antifungal medications may be needed they are;
1. Fluconazole (300 mg once weekly for 2 weeks)
2. Itraconazole (200 mg daily for 5-7 days)
3. Ketoconazole (200 mg 5 days-5 weeks),
• Vigorous exercise an hour after taking the medication may help sweat it onto the skin surface, where it can effectively eradicate the fungus. Avoid bathing for a few hours.
• Though it is easily treated, pigment changes may last for monthsafter treatment.
• Because this rash has a high recurrence rate, medication may be needed periodically to prevent recurrence. The rate of recurrence of pityriasis versicolor is very high, especially in hot humid climates so avoid heat in hot weather.
• Patients at high risk for recurrence may be helped by using ketoconazole shampoo once weekly as a body cleanser. Another preventative measure is once-monthly dosing of oral ketoconazole(400 mg), fluconazole (300 mg) or itraconazole (400 mg).

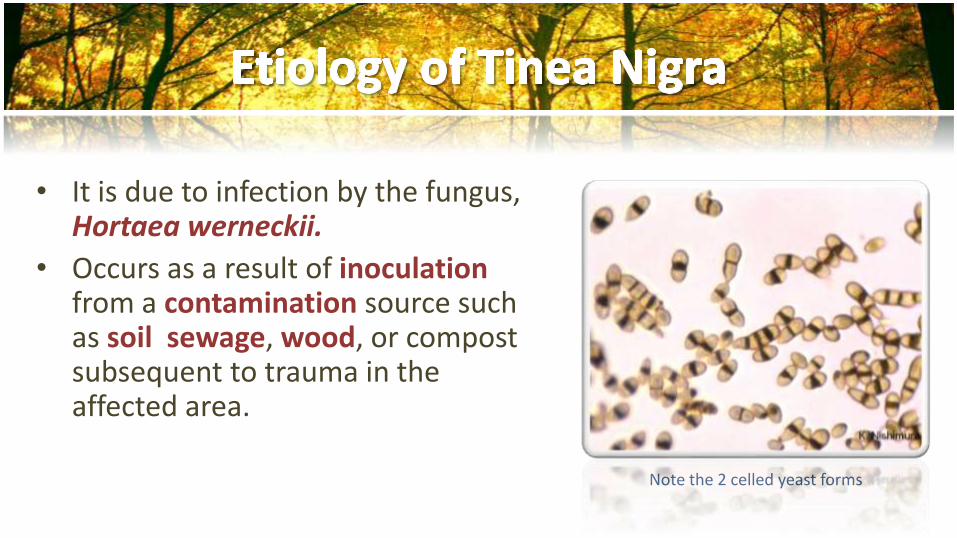
• It is due to infection by the fungus, Hortaea werneckii.
• Occurs as a result of inoculationfrom a contamination source such as soil sewage, wood, or compost subsequent to trauma in the affected area.
Note the 2 celled yeast forms
• Typically occur in tropical climates such as Central and South America, Africa, Asia and, occasionally, in the southeastern US.
• No predispositions have been identified.
• Typically, the incubation period is 10- to 15-day.
• A pigmentary change in the skin results from the accumulation of a melanin-like substance in the fungus.

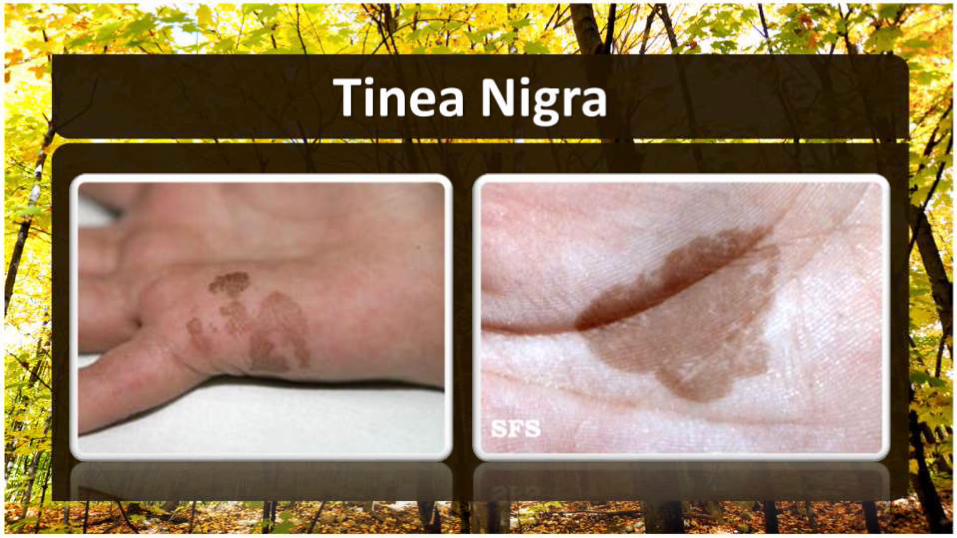
• Asymptomatic brown-to-black sharplymarginated macule or patch, resembling silver nitrate or India ink stains.
• The surface may appear mottled, velvety or have mild scale.
• The lesions are typically solitary, although may be multiple.
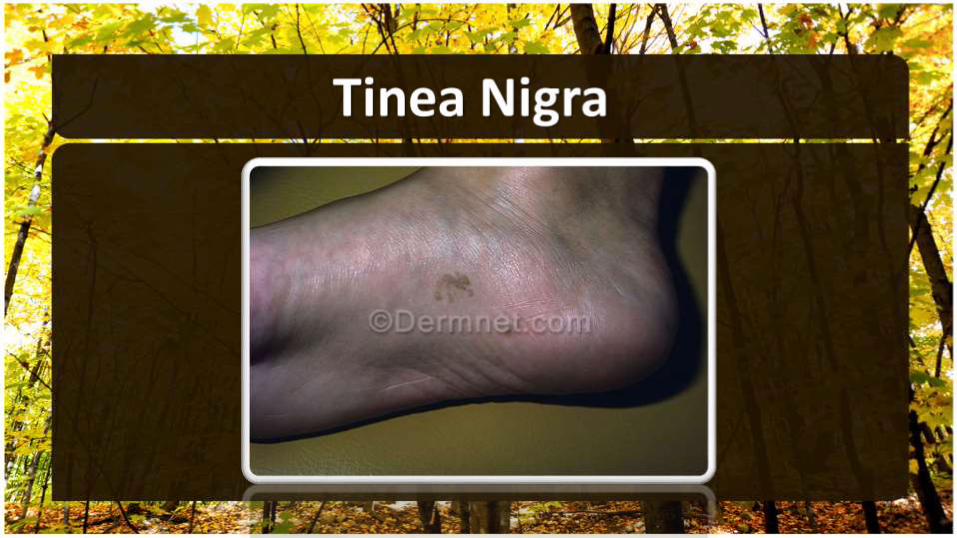
• Although most frequently seen on the palms, tinea nigra can also appear on the soles, neck and trunk.

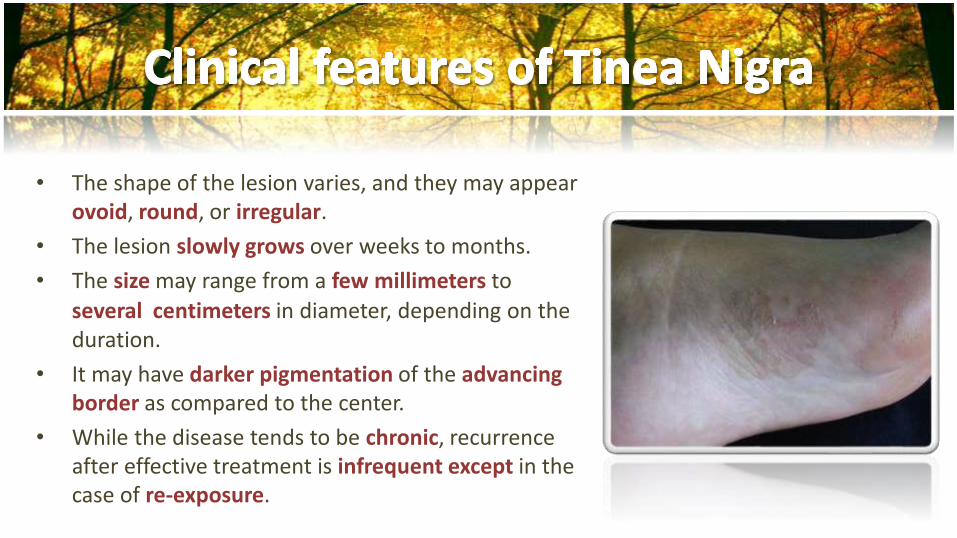
• The shape of the lesion varies, and they may appear ovoid, round, or irregular.
• The lesion slowly grows over weeks to months.
• The size may range from a few millimeters to
several centimeters in diameter, depending on the duration.
• It may have darker pigmentation of the advancingborder as compared to the center.
• While the disease tends to be chronic, recurrence after effective treatment is infrequent except in the case of re-exposure.
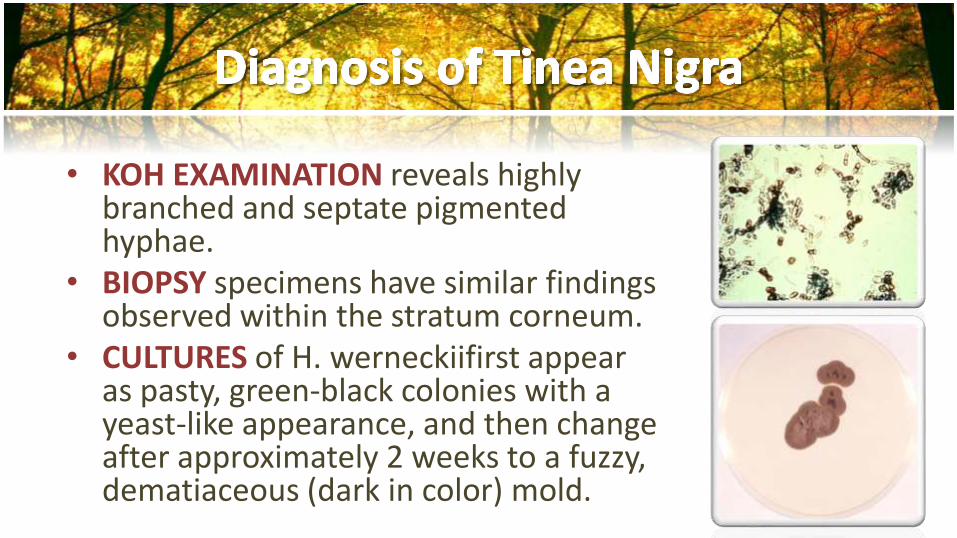
• KOH EXAMINATION reveals highly branched and septate pigmented hyphae.
• BIOPSY specimens have similar findings observed within the stratum corneum.
• CULTURES of H. werneckiifirst appear as pasty, green-black colonies with a yeast-like appearance, and then change after approximately 2 weeks to a fuzzy, dematiaceous (dark in color) mold.
1. Acral melanocytic nevi.
2. Fixed drug eruption.
3. Postinflammatory hyperpigmentation.
4. Staining from chemicals, pigments and dyes.
5. Melanoma.
1. Topical keratolytic agents such as Whitfield’s ointment(typically 6% benzoic acid plus 3% salicylic acid)
2. Topical azole
3. Topical Allylamine
• Several weeks of therapy may be required to preventrecurrence of disease.
• Systemic therapy is generally not indicated.

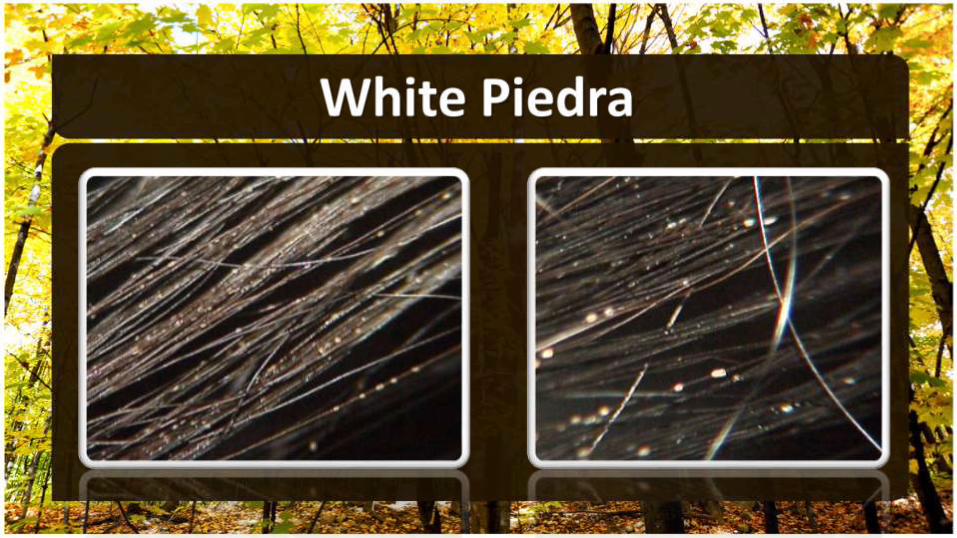
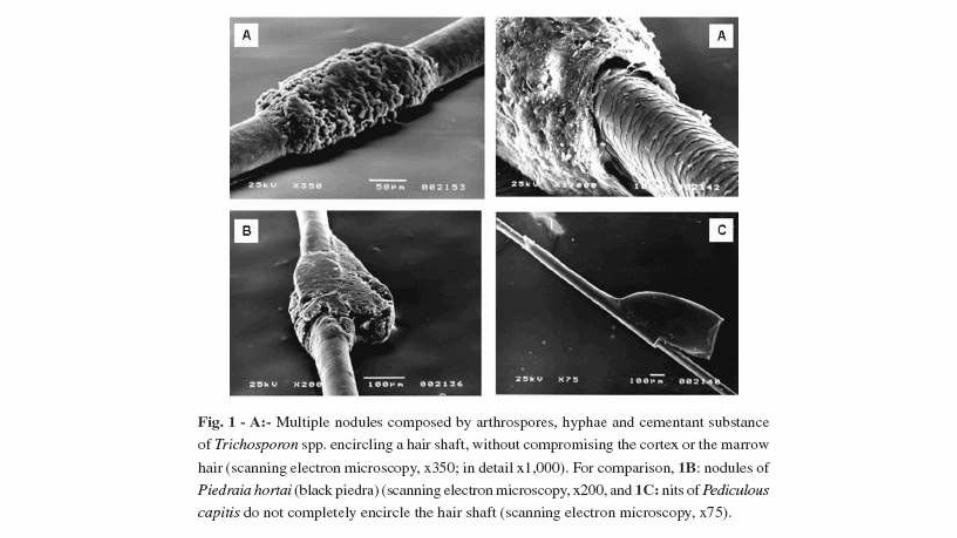
• It is a superficial non-inflammatory nodular fungal infection confined to hair shafts.
• “Piedra” means “stone”, reflecting the fungal elements’ adherence to one another to form nodules along the hair shaft, the surrounding skin is healthy.
• Favored climate; tropical areas.
• There are 2 types Black Piedra & White Piedra.

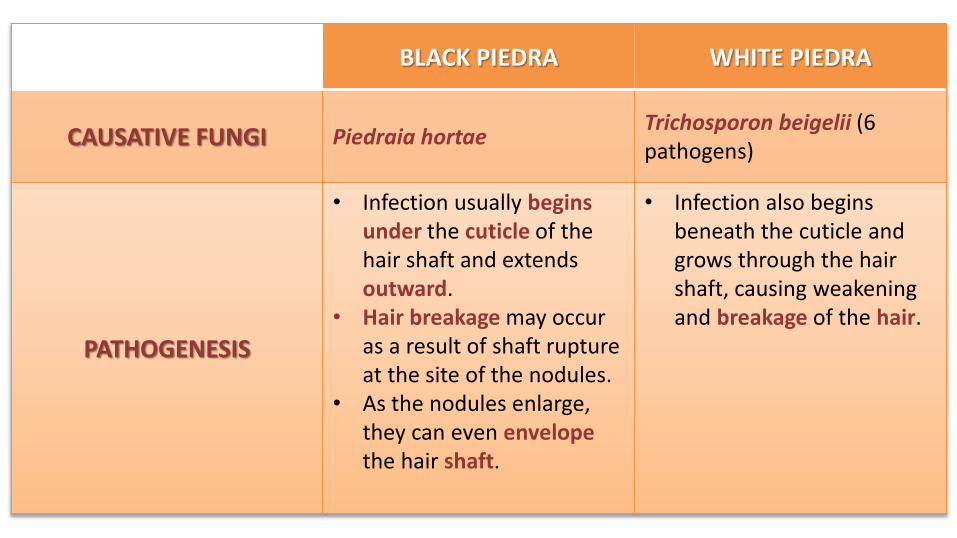
BLACK PIEDRA WHITE PIEDRA
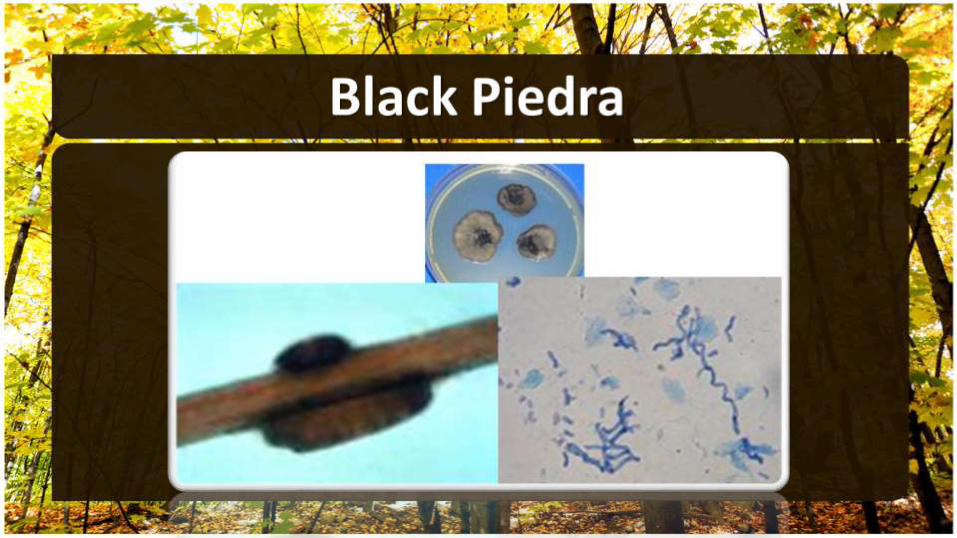
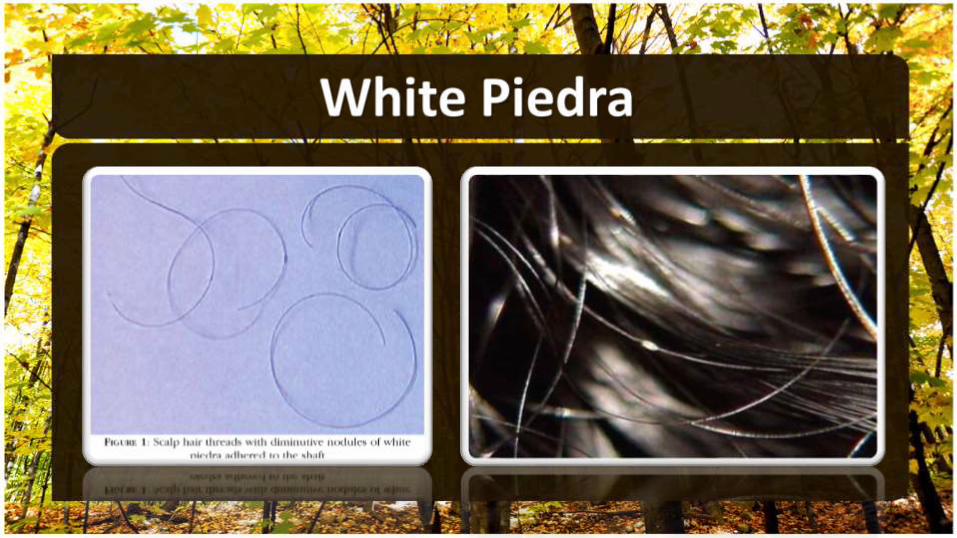
CAUSATIVE FUNGI Piedraia hortaeTrichosporon beigelii (6 pathogens)
PATHOGENESIS
• Infection usually beginsunder the cuticle of the hair shaft and extends outward.
• Hair breakage may occur as a result of shaft rupture at the site of the nodules.
• As the nodules enlarge, they can even envelopethe hair shaft.
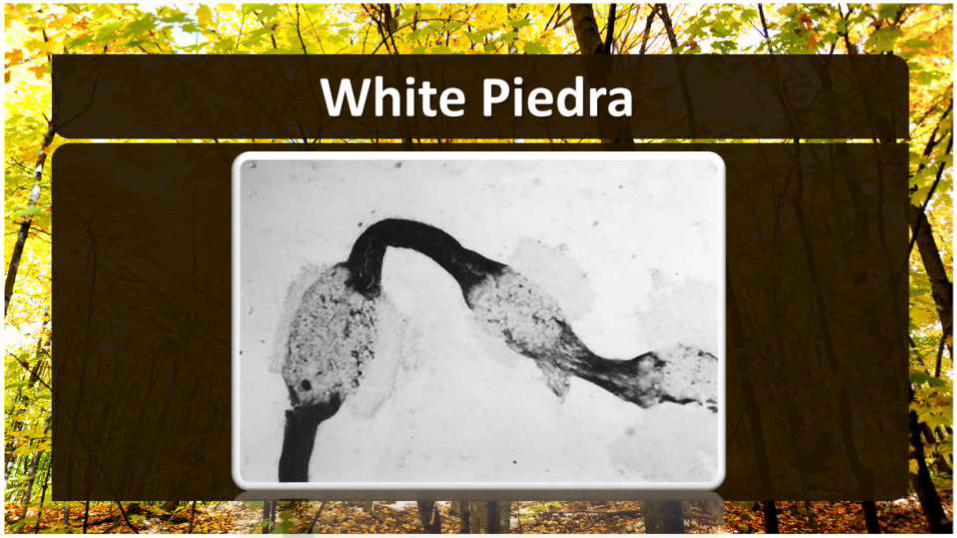
• Infection also begins beneath the cuticle and grows through the hair shaft, causing weakening and breakage of the hair.
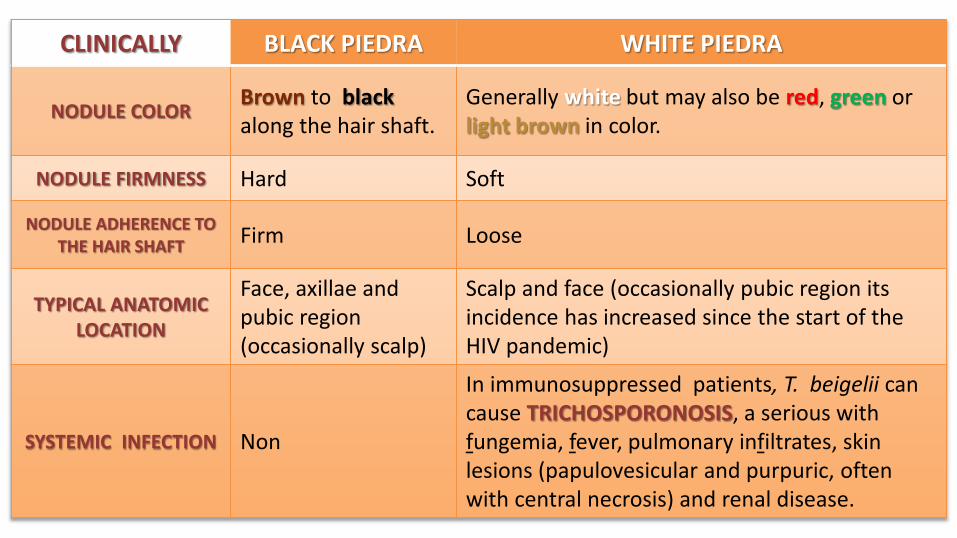
CLINICALLY BLACK PIEDRA WHITE PIEDRA
NODULE COLORBrown to blackalong the hair shaft.
Generally white but may also be red, green or light brown in color.
NODULE FIRMNESS Hard Soft
NODULE ADHERENCE TO THE HAIR SHAFT
Firm Loose
TYPICAL ANATOMICLOCATION
Face, axillae and pubic region (occasionally scalp)
Scalp and face (occasionally pubic region its incidence has increased since the start of the HIV pandemic)
SYSTEMIC INFECTION Non
In immunosuppressed patients, T. beigelii can cause TRICHOSPORONOSIS, a serious with fungemia, fever, pulmonary infiltrates, skin lesions (papulovesicular and purpuric, often with central necrosis) and renal disease.
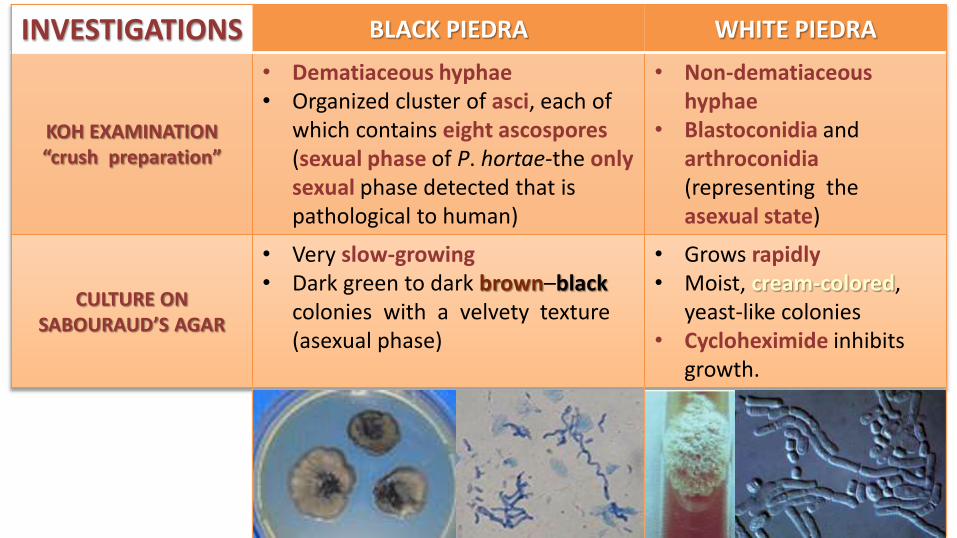
INVESTIGATIONS BLACK PIEDRA WHITE PIEDRA
KOH EXAMINATION“crush preparation”
• Dematiaceous hyphae• Organized cluster of asci, each of
which contains eight ascospores(sexual phase of P. hortae-the onlysexual phase detected that is pathological to human)
• Non-dematiaceoushyphae
• Blastoconidia andarthroconidia(representing the asexual state)
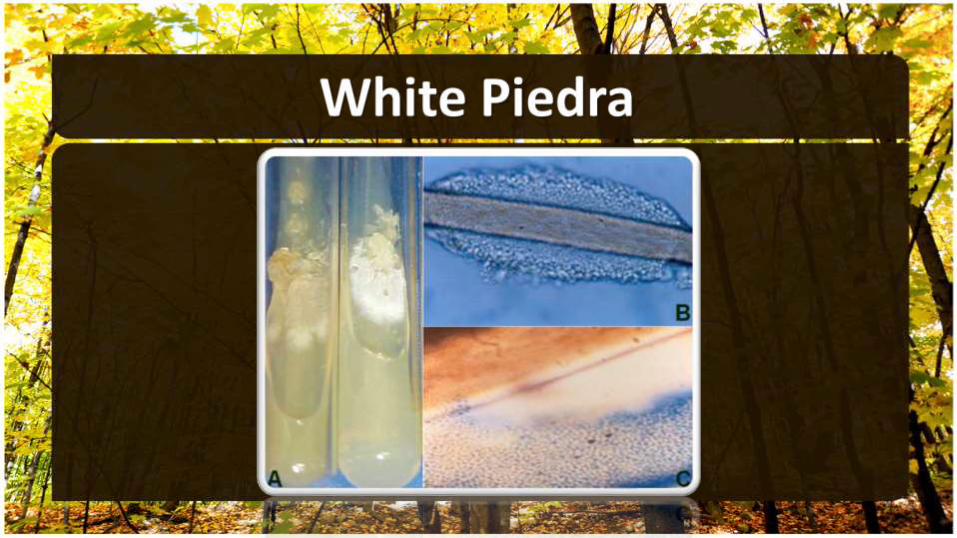
CULTURE ONSABOURAUD’S AGAR
• Very slow-growing• Dark green to dark brown–black
colonies with a velvety texture (asexual phase)
• Grows rapidly• Moist, cream-colored,
yeast-like colonies• Cycloheximide inhibits
growth.
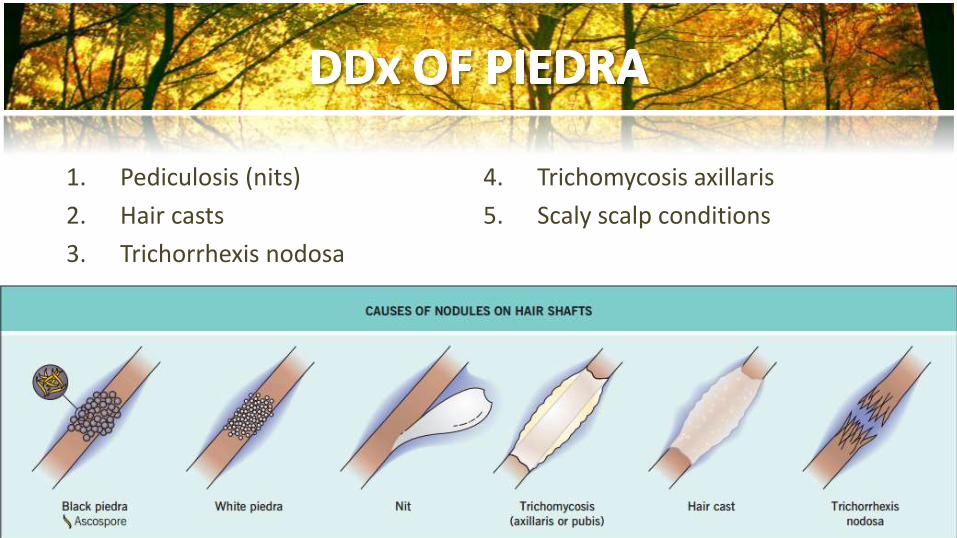
1. Pediculosis (nits)
2. Hair casts
3. Trichorrhexis nodosa
4. Trichomycosis axillaris
5. Scaly scalp conditions
1. Clip affected hairs.
2. Wash affected hairs with antifungal shampoo 2% ketoconazole shampoo or selenium sulfide.
3. Topical imidazole cream.
4. Oral terbinafine may also be used for black piedra.
5. Oral itraconazole may also be used for white piedra.