Embed Size (px)
Citation preview

Functional NeurologyWhat’s it all about?
Dr Naomi Warren

Content Background Clinical presentations Investigations Management Future aims

Background
Historically: hysteria (the “wandering womb”) conversion disorders dissociative disorders psychogenic medically unexplained non-organic psychosomatic functional

Functional symptomsCommon… 15% new outpatient neurology 1-10% of inpatient neurology admissions 50% of “status epilepticus” 10% of “first fits” 5% of movement disorders
Patients are just as distressed as patients with disease

Not specific to Neurology...Speciality SymptomCardiology non-cardiac CP
Gastroenterology IBS
Respiratory chronic cough
Renal/gynae recurrent loin/pelvic pain
Surgery chronic abdominal pain
Rheumatology fibromyalgia chronic fatigue syndrome
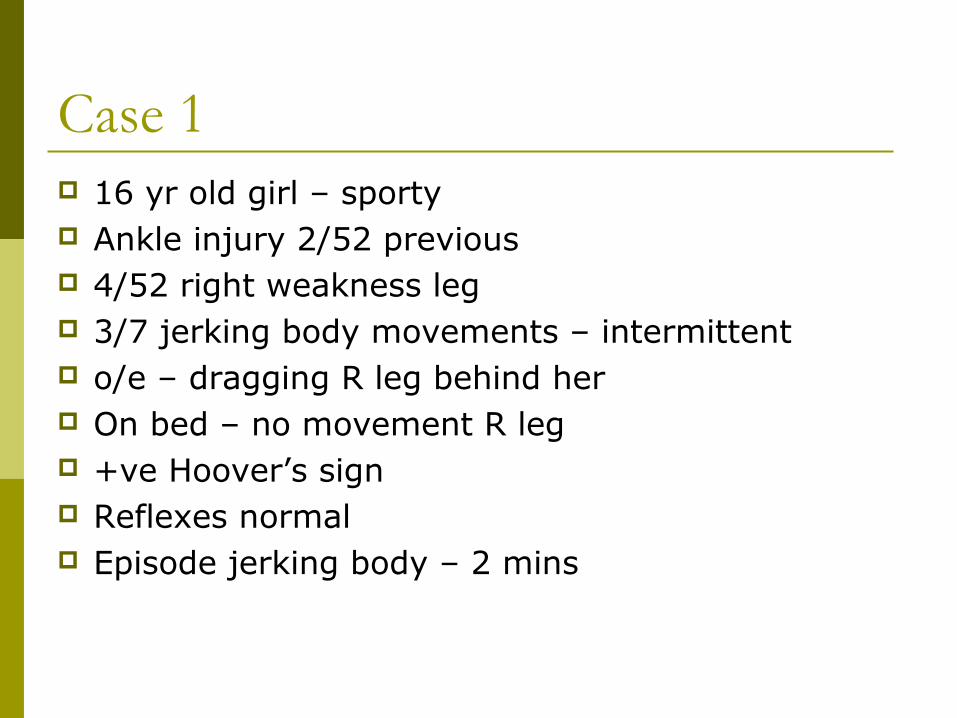
Case 1 16 yr old girl – sporty Ankle injury 2/52 previous 4/52 right weakness leg 3/7 jerking body movements – intermittent o/e – dragging R leg behind her On bed – no movement R leg +ve Hoover’s sign Reflexes normal Episode jerking body – 2 mins
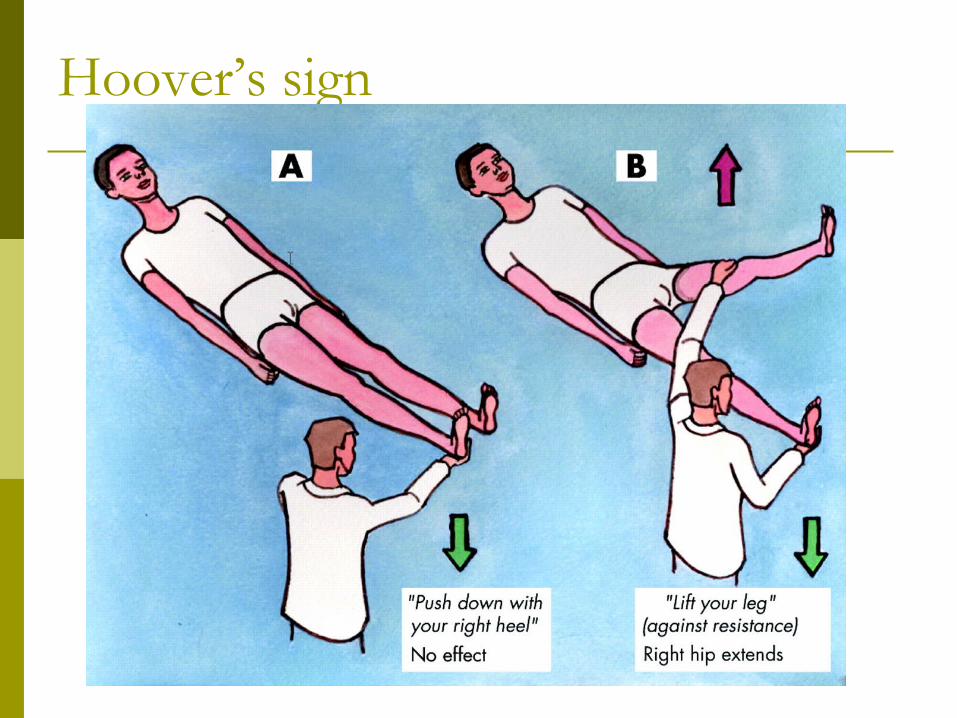
Hoover’s sign
Case cont…. Explained
Functional Not seizure
Denied stresses initially Parents – due to leave UK stress
Treatment Physio Snowboarding!! www.neurosymptoms.org
Good outcome

Functional weakness Half sudden onset Often with pain Examination
Look for inconsistencies bed/day to day
Hoovers sign Odd pattern Giving way Dragging leg Ass hemi sensory loss

Functional gait disorders gait disorders
dragging leg crouching gait tightrope gait without falling
Rhombergs Wibble and wobble but don’t fall down

Case 2 34 yr old R handed woman FT administrator Sudden onset tremor right hand 4 days
previous Present constantly No previous history

video

Functional movement disorders
Can be more difficult to identify
Mostly sudden onset Eg after injury
Tremor Disappears with distraction, entrainment,
variable

Other mvmt disorders - rarer Dystonia
Fixed, often painful Beware - often organic disease looks unusual
Myoclonus often axial
Tics

Non-epileptic attacks
Aura Not stereotyped Variable time
Attack Violent Long/multiple Violent No “tonic” phase Fast resp
Post ictal Crying No true confusion
• Not helpfulIncontinenceInjuries
• Some helpTongue biting - lateral

Other functional presentations Cognitive decline
subjective cognitive problems although can usually give a very clear account of themselves
Visual loss tunnel vision or blindness with preserved pupil reflexes and
optico-kinetic nystagmus Globus Dysphonia

Investigations? Minimal tests Often need MRI in weakness
Reassure pt/docs ?functional overlay
Explain You think the tests will be normal Incidental findings
Video EEG in seizures

Management Explanation
Key Psychiatry/ology
To help manage symps CBT
Antidepressants Physio Pain team www.neurosymptoms.
org
Give diagnosis Tell what don’t have Mechanism Understanding Emphasise common Reversible “stress/mood makes it
worse” Self help Consistency

PrognosisGood Bad
Acceptance Strong belief permanent
Young age Long history
Short history Delayed diagnosis
Lack other symps Anger at diagnosis
Change in marital status after diagnosis
Multiple other symps
Anx/depression Pampering carer
Helpful family Personality disorder
Financial benefit

Primary + secondary care aims To understand/believe the condition To provide swift diagnosis To give a consistent message
(limit 2nd opinions) To give appropriate psychological and
physical therapies
Unless self limiting and clearly functional – refer to neurology
Conclusion Very common problem in neurology Huge cause disability Needs swift investigation and mgmt Careful explanation Appropriate psychological help
Questions?









![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://img.pdfslide.us/doc/110x75/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)